

Chronic obstructive pulmonary disease (COPD) management involves treatment of chronic stable COPD and treatment of exacerbations.
Treatment of chronic stable COPD aims to prevent exacerbations and improve lung and physical function through
Medication therapy
Enhancement of nutrition
Pulmonary rehabilitation, including exercise
Surgical treatment of COPD is indicated for selected patients. This may include lung volume reduction procedures or lung transplantation.
Smoking Cessation in Stable COPD
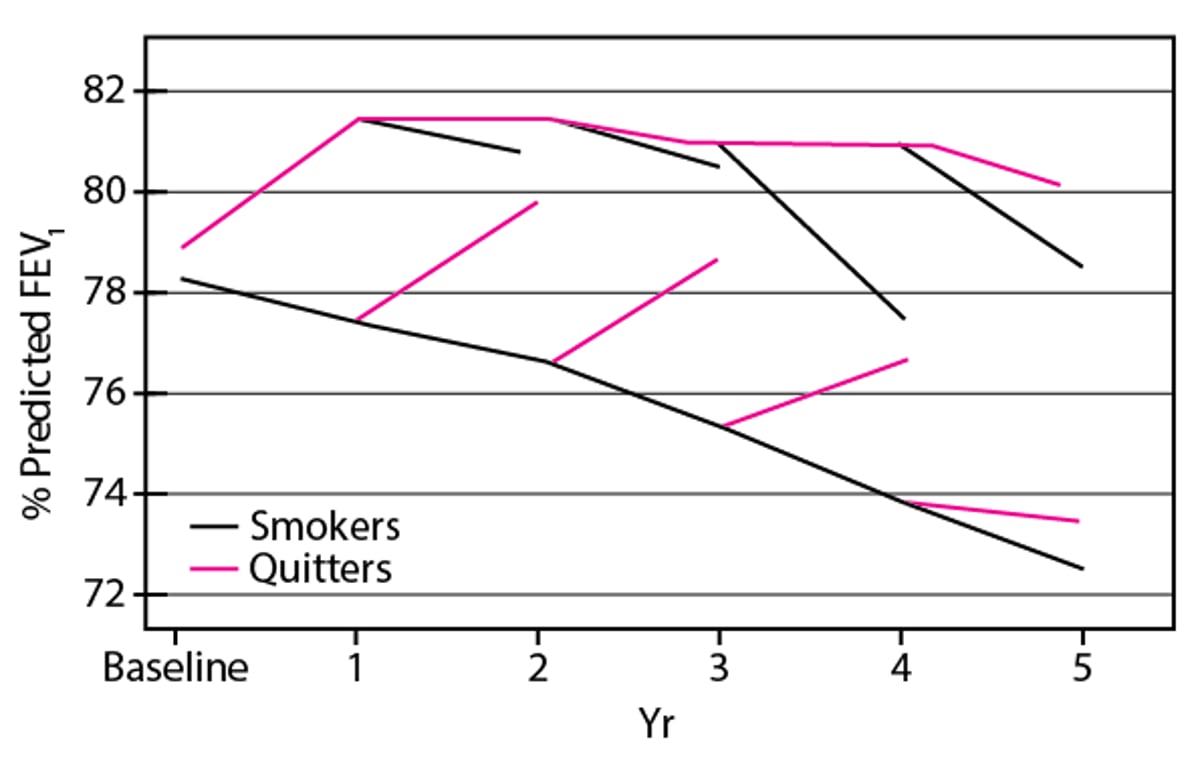
Smoking cessation is both extremely difficult and extremely important; it slows but does not halt the rate of FEV1 decline (see figure ) and increases long-term survival. Simultaneous use of multiple strategies is most effective:
Establishment of a quit date
Behavior modification techniques
Group sessions
Nicotine replacement therapy (by gum, transdermal patch, inhaler, lozenge, or nasal spray)
Varenicline or bupropionVarenicline or bupropion
Physician encouragement
Quit rates are generally low among patients with COPD (1), even with the most effective interventions, such as use of bupropion combined with ), even with the most effective interventions, such as use of bupropion combined withnicotine replacement or use of varenicline alone.replacement or use of varenicline alone.
Changes in Lung Function (Percentage of Predicted FEV1) in Patients Who Quit Smoking Compared With Those Who Continue
During the first year, lung function improved in patients who quit smoking and declined in those who continued. Subsequently, the rate of decline in those who continued was twice that of those who quit. Function declined in those who relapsed and improved in those who quit regardless of when the change occurred. Based on data from Scanlon PD et al: Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease; the Lung Health Study. American Journal of Respiratory and Critical Care Medicine 161:381–390, 2000. |

Smoking cessation reference
1. Liu Y, Greenlund KJ, VanFrank B, et al: Smoking Cessation Among U.S. Adult Smokers With and Without Chronic Obstructive Pulmonary Disease, 2018. Am J Prev Med 62(4):492–502, 2022. doi:10.1016/j.amepre.2021.12.001
Medication Therapy for Stable COPD
Recommended medication therapy is summarized in the table Pharmacotherapy of COPD.
Inhaled bronchodilators are the mainstay of COPD management; medications include
Beta-agonists
Anticholinergics (antimuscarinics)
These 2 classes of drugs are equally effective. Patients with mild disease are treated only when symptomatic. Patients with moderate to severe COPD should be taking medications from one or both of these classes regularly to improve pulmonary function and increase exercise capacity.
The frequency of exacerbations can be reduced with the use of anticholinergics, inhaled corticosteroids, or long-acting beta-agonists. However, there is no convincing evidence that regular bronchodilator use slows deterioration of lung function. The initial choice among short-acting beta-agonists, long-acting beta-agonists, anticholinergics, and combination beta-agonist and anticholinergic therapy is often a matter of tailoring cost and convenience to the patient’s preferences and symptoms.
For home treatment of chronic stable disease, medication administration by metered-dose inhaler or dry-powder inhaler is preferred over administration by nebulizer; home nebulizers are prone to contamination when cleaning and drying are incomplete. Nebulizers deliver medication to more proximal airways due to tidal breathing compared to total lung capacity maneuvers with inhalers, leading to inefficient medication administration. Therefore, nebulizers should be reserved for people who cannot coordinate activation of the metered-dose inhaler with inhalation or cannot develop enough inspiratory flow for dry powder inhalers.
For metered-dose inhalers, patients should be taught to exhale to functional residual capacity, inhale the aerosol slowly to total lung capacity, and hold the inhalation for 3 to 4 seconds before exhaling. Spacers help ensure optimal delivery of medication to the distal airways and reduce the importance of coordinating activation of the inhaler with inhalation. Some spacers alert patients if they are inhaling too rapidly. New or not recently used metered-dose inhalers require 2 to 3 priming doses (different manufacturers have slightly different recommendations for what is considered "not recently used," ranging from 3 to 14 days).
Dry powder inhalers, in contrast to metered-dose inhalers, require a rapid deep inspiratory effort in order to disaggregate the powder so that the smallest particles are deposited in the terminal airspaces.
Pharmacotherapy of COPD
Approach to Therapy | Dyspnea without exacerbations | Exacerbations with or without dyspnea |
|---|---|---|
Initial therapy* | LABA or LAMA | LABA or LAMA |
Initial escalation of therapy | LABA + LAMA | LABA + LAMA or LABA + LAMA + ICS† |
Subsequent approach to therapy for persistent symptoms | Consider changing inhaler device or medication Implement or escalate non-pharmacological treatments Evaluation for other causes of dyspnea | LABA + LAMA + ICS + roflumilast or azithromycin‡ LABA + LAMA + ICS + roflumilast or azithromycin‡ |
* Rescue short-acting bronchodilators should be prescribed to all patients for immediate symptom relief. | ||
† ICS is most effective in patients with eosinophilia ≥ 150/mcL (≥ 0.15 × 109/L). May need to de-escalate ICS if the patient develops pneumonia or does not respond to treatment. In patients with eosinophilia ≥ 300 mcL (≥ 0.30 × 109/L), de-escalation is more likely to cause an exacerbation. | ||
‡ For recurrent exacerbations, add either a PDE4 inhibitor (eg, roflumilast) or long-term azithromycin. Roflumilast is indicated in patients with COPD (FEV1 ‡ For recurrent exacerbations, add either a PDE4 inhibitor (eg, roflumilast) or long-term azithromycin. Roflumilast is indicated in patients with COPD (FEV1< 50%) with chronic bronchitis. Azithromycin is preferred for former smokers and is less effective in current smokers.50%) with chronic bronchitis. Azithromycin is preferred for former smokers and is less effective in current smokers. | ||
FEV1 = The volume of air forcefully expired during the first second after taking a full breath; LABA = long-acting beta agonist; LAMA = long-acting antimuscarinic antagonist; ICS = inhaled corticosteroid; PDE4 = phosphodiesterase-4 inhibitor. | ||
Adapted from the Global Initiative for Chronic Obstructive Lung Disease (GOLD): Global Strategy for the Prevention, Diagnosis, and Management of COPD: 2024 report. Available at http://www.goldcopd.org. | ||
Beta-agonists
Beta-agonists relax bronchial smooth muscle and increase mucociliary clearance. Albuterol aerosol, 2 puffs inhaled from a metered-dose inhaler 4 to 6 times a day as needed, is usually the medication of choice for episodic dyspnea or early treatment of exacerbations. Beta-agonists relax bronchial smooth muscle and increase mucociliary clearance. Albuterol aerosol, 2 puffs inhaled from a metered-dose inhaler 4 to 6 times a day as needed, is usually the medication of choice for episodic dyspnea or early treatment of exacerbations.
Long-acting beta-agonists are preferable for patients with nocturnal symptoms or for those who find frequent dosing inconvenient, and may be used as initial therapy for COPD. Options include salmeterol powder, 1 puff (50 mcg) inhaled twice a day, indacaterol 1 puff (75 mcg) inhaled once a day (150 mcg once a day in Europe), and olodaterol 2 puffs once a day at the same time each day. Vilanterol and formoterol are available in combination with an inhaled corticosteroid. Also available are nebulized forms of arformoterol and formoterol. The dry-powder formulations may be more effective for patients who have trouble coordinating use of a metered-dose inhaler. are preferable for patients with nocturnal symptoms or for those who find frequent dosing inconvenient, and may be used as initial therapy for COPD. Options include salmeterol powder, 1 puff (50 mcg) inhaled twice a day, indacaterol 1 puff (75 mcg) inhaled once a day (150 mcg once a day in Europe), and olodaterol 2 puffs once a day at the same time each day. Vilanterol and formoterol are available in combination with an inhaled corticosteroid. Also available are nebulized forms of arformoterol and formoterol. The dry-powder formulations may be more effective for patients who have trouble coordinating use of a metered-dose inhaler.
Patients should be taught the difference between short-acting and long-acting medications, because long-acting medications that are used as needed or more than twice a day increase the risk of cardiac arrhythmias.
Adverse effects commonly result from use of any beta-agonist and include tremor, anxiety, tachycardia, and mild, temporary hypokalemia.
Anticholinergics
Anticholinergics (antimuscarinics) relax bronchial smooth muscle through competitive inhibition of muscarinic receptors (M1, and M3). Long-acting antimuscarinic antagonists are a reasonable alternative as first-line therapy for patients with COPD. Adverse effects of all anticholinergics are pupillary dilation (and risk of triggering or worsening acute angle closure glaucoma), urinary retention, and dry mouth.
Ipratropium is a short-acting anticholinergic; dose is 2 to 4 puffs (17 mcg/puff) from a metered-dose inhaler every 4 to 6 hours. Ipratropium is a short-acting anticholinergic; dose is 2 to 4 puffs (17 mcg/puff) from a metered-dose inhaler every 4 to 6 hours.Ipratropium has a slower onset of action (within 30 minutes; peak effect in 1 to 2 hour), so a beta-agonist is often prescribed with it in a single combination inhaler or as a separate as-needed rescue medication.
Tiotropium is a long-acting quaternary anticholinergic inhaled as a powder formulation (18 mcg/puff) or as a soft mist inhaler (2.5 mcg/puff). Dose is 1 puff (18 mcg) once a day by dry powder inhaler and 2 puffs (5 mcg) once a day by soft mist inhaler.Tiotropium is a long-acting quaternary anticholinergic inhaled as a powder formulation (18 mcg/puff) or as a soft mist inhaler (2.5 mcg/puff). Dose is 1 puff (18 mcg) once a day by dry powder inhaler and 2 puffs (5 mcg) once a day by soft mist inhaler.
Aclidinium is available as a multidose dry-powder inhaler. Dose is 1 puff (400 mcg/puff) twice a day. Aclidinium is available as a multidose dry-powder inhaler. Dose is 1 puff (400 mcg/puff) twice a day.Aclidinium is also available in combination with a long-acting beta-agonist as a dry-powder inhaler.
Umeclidinium can be used as a once a day combination with vilanterol (a long-acting beta-agonist) in a dry-powder inhaler.Umeclidinium can be used as a once a day combination with vilanterol (a long-acting beta-agonist) in a dry-powder inhaler.
Glycopyrrolate (an anticholinergic) can be used twice a day in combination with indacaterol or formoterol (long-acting beta-agonists) in a dry-powder or metered-dose inhaler. Glycopyrrolate (an anticholinergic) can be used twice a day in combination with indacaterol or formoterol (long-acting beta-agonists) in a dry-powder or metered-dose inhaler.
Revefenacin is given once a day via nebulizer. Revefenacin is given once a day via nebulizer.
Inhaled corticosteroids
Corticosteroids are often part of treatment. Inhaled corticosteroids seem to reduce airway inflammation, reverse beta-receptor down-regulation, and inhibit leukotriene and cytokine production. They do not alter the course of pulmonary function decline in patients with COPD who continue to smoke, but they do relieve symptoms and improve short-term pulmonary function in some patients, are additive to the effect of bronchodilators, and diminish the frequency of COPD exacerbations. They are indicated for patients who have repeated exacerbations or symptoms despite optimal bronchodilator therapy. Inhaled corticosteroids are of greatest benefit in patients who have eosinophilia (1). In patients with exacerbations, addition of an inhaled corticosteroid reduces exacerbation frequency and prolongs survival (2, 3).
The long-term risks of inhaled corticosteroids in older adults are not proved but probably include osteoporosis, cataract formation, and an increased risk of nonfatal pneumonia. Long-term users therefore should undergo periodic ophthalmologic and bone densitometry screening if indicated (eg, by a history of changes in night vision, frailty, or bone fractures) and should possibly receive supplemental calcium, vitamin D, and a bisphosphonate as indicated.
De-escalation of inhaled corticosteroid therapy may be necessary if patients develop pneumonia or do not respond to treatment.
Use of a combination of a long-acting beta-agonist and an inhaled corticosteroid without the use of a long-acting anticholinergic is no longer recommended for patients with COPD unless they have concomitant asthma.
Oral or systemic corticosteroids should usually not be used to treat chronic stable COPD.
Theophylline
Theophylline is no longer recommended for the treatment of chronic stable COPD now that safer, more effective medications are available. Theophylline decreases smooth muscle spasm, enhances mucociliary clearance, improves right ventricular function, and decreases pulmonary vascular resistance and arterial pressure. Its mode of action is poorly understood but appears to differ from that of beta-2-agonists and anticholinergics. Its role in improving diaphragmatic function and dyspnea during exercise is unclear.Theophylline is no longer recommended for the treatment of chronic stable COPD now that safer, more effective medications are available. Theophylline decreases smooth muscle spasm, enhances mucociliary clearance, improves right ventricular function, and decreases pulmonary vascular resistance and arterial pressure. Its mode of action is poorly understood but appears to differ from that of beta-2-agonists and anticholinergics. Its role in improving diaphragmatic function and dyspnea during exercise is unclear.
Theophylline can be used for patients who have not adequately responded to inhaled medications and who have shown symptomatic benefit during a trial of theophylline. Serum levels need not be monitored unless the patient does not respond to the medication, develops symptoms of toxicity, or is questionably adherent; slowly absorbed oral theophylline preparations, which require less frequent dosing, enhance adherence. Theophylline can be used for patients who have not adequately responded to inhaled medications and who have shown symptomatic benefit during a trial of theophylline. Serum levels need not be monitored unless the patient does not respond to the medication, develops symptoms of toxicity, or is questionably adherent; slowly absorbed oral theophylline preparations, which require less frequent dosing, enhance adherence.
Toxicity is common and includes sleeplessness and gastrointestinal upset, even at low blood levels. More serious adverse effects, such as supraventricular and ventricular arrhythmias and seizures, tend to occur at blood levels > 20 mg/L (111 micromol/L).
Hepatic metabolism of theophylline varies greatly and is influenced by genetic factors, age, cigarette smoking, hepatic dysfunction, diet, and some medications, such as macrolide and fluoroquinolone antibiotics and nonsedating histamine 2 blockers.Hepatic metabolism of theophylline varies greatly and is influenced by genetic factors, age, cigarette smoking, hepatic dysfunction, diet, and some medications, such as macrolide and fluoroquinolone antibiotics and nonsedating histamine 2 blockers.
Phosphodiesterase-4 inhibitors
Phosphodiesterase-4 inhibitors are more specific than theophylline for pulmonary phosphodiesterase and have fewer adverse effects. They have anti-inflammatory properties and are mild bronchodilators. Phosphodiesterase-4 inhibitors such as roflumilast can be used in addition to other bronchodilators for reduction of exacerbations in patients who have symptomatic COPD with chronic bronchitis..Phosphodiesterase-4 inhibitors are more specific than theophylline for pulmonary phosphodiesterase and have fewer adverse effects. They have anti-inflammatory properties and are mild bronchodilators. Phosphodiesterase-4 inhibitors such as roflumilast can be used in addition to other bronchodilators for reduction of exacerbations in patients who have symptomatic COPD with chronic bronchitis..
Common adverse effects include nausea, headache, and weight loss, but these effects may subside with continued use.
Macrolide antibiotics
Long-term azithromycin therapy is an effective adjunct to prevent COPD exacerbations in patients who are prone to repeated or severe exacerbations, particularly those who are not currently smoking. An Long-term azithromycin therapy is an effective adjunct to prevent COPD exacerbations in patients who are prone to repeated or severe exacerbations, particularly those who are not currently smoking. Anazithromycin dose of 250 mg orally once a day has demonstrated efficacy (4). Erythromycin can be an alternative. ). Erythromycin can be an alternative.
Medication therapy references
1. Pascoe S, Barnes N, Brusselle G, et al: Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: analysis of the IMPACT trial. Lancet Respir Med 7(9):745–756 2019. doi: 10.1016/S2213-2600(19)30190-0
2. Lipson DA, Crim C, Criner GJ, et al: Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 201(12):1508–1516, 2020. doi: 10.1164/rccm.201911-2207OC
3. Rabe KF, Martinez FJ, Ferguson GT, et al: Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med 383(1):35–48, 2020. doi: 10.1056/NEJMoa1916046
4. Albert RK, Connett J, Bailey WC, et al: Azithromycin for prevention of exacerbations of COPD [published correction appears in N Engl J Med 2012 Apr 5;366(14):1356]. N Engl J Med 365(8):689–698, 2011. doi:10.1056/NEJMoa1104623
Oxygen Therapy for Stable COPD
Long-term oxygen therapy prolongs life in patients with COPD whose partial pressure of arterial oxygen (PaO2) is chronically < 55 mm Hg. Continual 24-hour use is more effective than a 12-hour nocturnal regimen. Oxygen therapy does the following:
Brings hematocrit toward normal levels
Improves neuropsychologic factors, possibly by facilitating sleep
Ameliorates pulmonary hemodynamic abnormalities
Increases exercise tolerance in some patients
Oxygen saturation should be measured during exercise and while at rest. Similarly, a sleep study should be considered for patients with advanced COPD who do not meet the criteria for long-term oxygen therapy while they are awake (see table ) but whose clinical assessment suggests pulmonary hypertension in the absence of daytime hypoxemia. Nocturnal oxygen may be prescribed if a sleep study shows episodic desaturation to ≤ 88%. Such treatment prevents progression of pulmonary hypertension, but its effects on survival are unknown. In patients with moderate hypoxemia above 88% or exercise desaturation, oxygen therapy may reduce symptoms, but there is no improvement in survival or reduction in hospitalizations (1).
Some patients need supplemental oxygen during air travel because flight cabin pressure in commercial airliners is below sea level air pressure (often equivalent to 1830 to 2400 m [6000 to 8000 ft]). Patients with COPD who are eucapnic and have a PaO2 > 68 mm Hg at sea level generally have an in-flight PaO2 > 50 mm Hg and do not require supplemental oxygen. All patients with COPD with a PaO2 ≤ 68 mm Hg at sea level, hypercapnia, significant anemia (hematocrit < 30), or a coexisting heart or cerebrovascular disorder should use supplemental oxygen during long flights and should notify the airline when making their reservation. Because portable oxygen concentrators are ubiquitous, very few airlines still provide oxygen. Patients are advised to rent or purchase a portable oxygen concentrator for use during air travel, including enough spare batteries to account for the flight time and possible delays.
All patients must be taught the dangers of smoking or cooking over an open flame during oxygen use.
Indications for Long-Term Oxygen Therapy in COPD
PaO2 ≤ 55 mm Hg or SaO2 ≤ 88%* in patients receiving optimal medical regimen for at least 30 days† |
PaO2 = 55 to 59 mm Hg or SaO2 ≤ 89%* for patients with cor pulmonale or erythrocytosis (> 55%) |
Can be considered for patients with exercise desaturation or severe dyspnea if there is symptomatic improvement; however, there is no improvement in survival or hospitalization. May also be considered for patients with nocturnal desaturation.‡ |
* Arterial oxygen levels are measured at rest during air breathing. |
† Patients who are recovering from an acute respiratory illness and who meet the listed criteria should be given oxygen and rechecked while breathing room air after 60 to 90 days. |
‡ See also Long-Term Oxygen Treatment Trial Research Group: A randomized trial of long-term oxygen for COPD with moderate desaturation. N Engl J Med 375:1617–1627, 2016. |
Hct = hematocrit; PaO2 = arterial oxygen partial pressure; SaO2 = oxygen saturation. |
Oxygen administration
Oxygen is administered by nasal cannula at a flow rate sufficient to achieve a PaO2 > 60 mm Hg (oxygen saturation > 90%), usually ≤ 3 L/minute at rest (frequently higher at higher altitudes, such as in Denver, Colorado).
Oxygen is supplied by electrically driven oxygen concentrators, liquid oxygen systems, or cylinders of compressed gas. Stationary concentrators, which limit mobility but are the least expensive, are preferable for patients who spend most of their time at home. Such patients require small oxygen tanks for backup in case of an electrical failure and for portable use. Portable concentrators that allow mobility can be used for patients who do not require high flow rates.
A liquid system is preferable for patients who spend much time out of their home. Portable canisters of liquid oxygen are easier to carry and have more capacity than portable cylinders of compressed gas.
Large compressed oxygen cylinders are the most expensive way of providing oxygen and should be used only if no other source is available.
Various oxygen-conserving devices can reduce the amount of oxygen used by the patient, either by using a reservoir system or by permitting oxygen flow only during inspiration. Systems with these devices may correct resting hypoxemia as effectively as continuous flow devices. However, intermittent flow devices may not be as effective as continuous flow for exercise-associated hypoxemia.
Oxygen therapy reference
1. Long-Term Oxygen Treatment Trial Research Group: A randomized trial of long-term oxygen for COPD with moderate desaturation. N Engl J Med 375:1617–1627, 2016.
Vaccinations in Stable COPD
All patients with COPD should be given annual influenza vaccinations. If COPD increases the risk of respiratory complications from influenza, prophylactic treatment with a neuraminidase inhibitor (oseltamivir or zanamivir) is recommended after close exposure to influenza-infected people. Treatment with a neuraminidase inhibitor or an endonuclease inhibitor (balaxovir marboxil) should be started at the first sign of an influenza-like illness and within 2 days of the exposure. . If COPD increases the risk of respiratory complications from influenza, prophylactic treatment with a neuraminidase inhibitor (oseltamivir or zanamivir) is recommended after close exposure to influenza-infected people. Treatment with a neuraminidase inhibitor or an endonuclease inhibitor (balaxovir marboxil) should be started at the first sign of an influenza-like illness and within 2 days of the exposure.
Pneumococcal vaccines should be administered because they are effective in reducing community-acquired pneumonia and invasive pneumococcal infections in older adults.
Respiratory syncytial virus (RSV) vaccine is recommended for adults over the age of 60 years regardless of COPD diagnosis, but COPD patients are likely to have significant benefit from RSV vaccination.
COVID-19 vaccination is also recommended for patients with COPD.
Nutrition in Stable COPD
Patients with COPD are at risk of weight loss and nutritional deficiencies because of a higher energy cost of daily activities, reduced caloric intake relative to need because of dyspnea, and the catabolic effect of inflammatory cytokines such as tumor necrosis factor (TNF)-alpha. Generalized muscle strength and efficiency of oxygen use are impaired. Patients with poorer nutritional status have a worse prognosis, so it is prudent to recommend a balanced diet with adequate caloric intake in conjunction with exercise to prevent or reverse undernutrition and muscle atrophy. Split-meal feeding can be helpful.
Excessive weight gain should be avoided, and patients who have obesity should strive to gradually reduce body fat.
Nutritional supplementation should be limited to patients who are undernourished, who may experience benefits in respiratory muscle strength and quality of life with from such intervention (1).
Trials of appetite stimulants, anabolic steroids, growth hormone supplementation, and TNF antagonists in reversing undernutrition and improving functional status and prognosis in COPD have been disappointing.
Nutrition reference
1. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2012;12:CD000998. Published 2012 Dec 12. doi:10.1002/14651858.CD000998.pub3
Pulmonary Rehabilitation in Stable COPD
Pulmonary rehabilitation programs serve as adjuncts to medication treatment to improve physical function; many hospitals and health care organizations offer formal multidisciplinary rehabilitation programs. Pulmonary rehabilitation includes
Exercise
Education
Behavioral interventions
Treatment should be individualized; patients and family members are taught about COPD and medical treatments, and patients are encouraged to take as much responsibility for personal care as possible.
The benefits of rehabilitation are greater independence and improved quality of life and exercise capacity. Pulmonary rehabilitation typically does not improve pulmonary function. A carefully integrated rehabilitation program helps patients with severe COPD accommodate to physiologic limitations while providing realistic expectations for improvement. Patients with severe disease require a minimum of 3 months of rehabilitation to benefit and should continue with maintenance programs.
An exercise program can be helpful in the home, in the hospital, or in institutional settings.
Graded exercise can ameliorate skeletal muscle deconditioning resulting from inactivity or prolonged hospitalization for respiratory failure. Specific training of respiratory muscles is less helpful than general aerobic conditioning.
A typical training program begins with slow walking on a treadmill or unloaded cycling on an ergometer for a few minutes. Duration and exercise load are progressively increased over 4 to 6 weeks until the patient can exercise for 20 to 30 minutes nonstop with manageable dyspnea. Patients with very severe COPD can usually achieve an exercise regimen of walking for 30 minutes at 1 to 2 mph (1.6 to 3.2 km per hour). Maintenance exercise should be done 3 to 4 times/week to maintain fitness levels. Oxygen saturation is monitored, and supplemental oxygen is provided as needed.
Upper extremity resistance training helps the patient in doing daily tasks (eg, bathing, dressing, house cleaning). The usual benefits of exercise are modest increases in lower extremity strength, endurance, and maximum oxygen consumption.
Patients should be taught ways to conserve energy during activities of daily living and to pace their activities. Difficulties in sexual function should be discussed and advice should be given on using energy-conserving techniques for sexual gratification.
Pulmonary rehabilitation can also be offered using telehealth models with variable types of access and supervision. In general, these programs lead to similar improvements in exercise capacity, but are less well proven to improve quality of life and dyspnea. Because of difficulty in accessing formal in-person pulmonary rehabilitation programs, it is recommended that virtual rehabilitation be offered to patients as an alternative to an in-person program (1).
Pulmonary rehabilitation reference
1. Rochester CL, Alison JA, Carlin B, et al. Pulmonary Rehabilitation for Adults with Chronic Respiratory Disease: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med 2023;208(4):e7-e26. doi:10.1164/rccm.202306-1066ST
Surgery in Stable COPD
Surgical options for treatment of severe COPD include
Lung volume reduction
Lung transplantation
Lung volume reduction surgery
Lung volume reduction surgery consists of resecting nonfunctioning emphysematous areas. The procedure improves lung function, exercise tolerance, and quality of life in patients with severe, predominantly upper-lung emphysema who have low baseline exercise capacity after pulmonary rehabilitation (1).
The effect on arterial blood gas measurements is variable and not predictable, but most patients who require oxygen therapy before surgery continue to need it. Improvement is less than that with lung transplantation. The mechanism of improvement is believed to be enhanced lung recoil and improved diaphragmatic function.
The best candidates for lung volume reduction surgery are patients with an FEV1 (the volume of air forcefully expired during the first second after taking a full breath) 20 to 40% of predicted, a diffusing capacity for carbon monoxide (DLCO) > 20% of predicted, significantly impaired exercise capacity, heterogeneous pulmonary disease on CT with an upper-lobe predominance, partial pressure of arterial carbon dioxide (PaCO2) < 50 mm Hg, and absence of severe pulmonary hypertension and coronary artery disease.
Rarely, patients have extremely large bullae that compress the functional lung. These patients can be helped by surgical resection of these bullae, with resulting relief of symptoms and improved pulmonary function. Generally, resection is most beneficial for patients with bullae affecting more than one third of a hemithorax and an FEV1 approximately half of the predicted normal value. Improved pulmonary function is related to the amount of normal or minimally diseased lung tissue that was compressed by the resected bullae. Serial chest radiographs and CT scans are the most useful procedures for determining whether a patient’s functional status is due to compression of viable lung by bullae or to generalized emphysema. A markedly reduced DLCO (< 40% predicted) indicates widespread emphysema and suggests a poorer outcome from surgical resection.
Endobronchial valve placement
Endobronchial valves that are inserted with a bronchoscope and cause atelectasis of emphysematous target regions of the lung in selected patients who do not have collateral ventilation to these regions are available in selected centers (2). Placement of an endobronchial valve is an alternative to lung volume reduction surgery in some patients. Surgical lung volume reduction is usually bilateral, whereas bronchoscopic procedures are usually unilateral and therefore result in less improvement.
Lung transplantation
Lung transplantation can be single or double. Perioperative complications tend to be lower with single-lung transplantation, but some evidence shows that survival time is increased with double-lung transplantation. Candidates for transplantation are patients < 65 years with an FEV1 < 25% predicted after bronchodilator therapy or with severe pulmonary hypertension. The goal of lung transplantation is to improve quality of life, because survival time is not necessarily increased. Lifelong immunosuppression is required, with the attendant risk of opportunistic infections.
Surgery references
1. Fishman A, Martinez F, Naunheim K, et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med 2003;348(21):2059-2073. doi:10.1056/NEJMoa030287
2. Criner GJ, Sue R, Wright S, et al. A Multicenter Randomized Controlled Trial of Zephyr Endobronchial Valve Treatment in Heterogeneous Emphysema (LIBERATE). Am J Respir Crit Care Med 2018;198(9):1151-1164. doi:10.1164/rccm.201803-0590OC
Key Points
Relieve symptoms of chronic obstructive pulmonary disease rapidly with primarily short-acting beta-adrenergic drugs and decrease exacerbations with inhaled corticosteroids, long-acting beta-adrenergic drugs, long-acting anticholinergic drugs, or a combination.
Encourage smoking cessation using multiple interventions (eg, behavior modification, support groups, nicotine replacement, medication therapy).
Optimize use of supportive treatments (eg, nutrition, pulmonary rehabilitation, self-directed exercise).





