



Almost half of all people in the United States report sleep-related problems. Disordered sleep can cause emotional disturbance, memory difficulty, poor motor skills, decreased work efficiency, and increased risk of traffic accidents. It can even contribute to cardiovascular disorders and mortality.
The most commonly reported sleep-related symptoms are insomnia and excessive daytime sleepiness (EDS).
Insomnia is difficulty falling or staying asleep, early awakening, or a sensation of unrefreshing sleep.
EDS is the tendency to fall asleep during normal waking hours.
EDS is not a disorder but a symptom of various sleep-related disorders. Insomnia can be a disorder, even if it exists in the context of other disorders, or can be a symptom of other disorders.
Parasomnias are abnormal sleep-related events (eg, night terrors, sleepwalking).
(See also Sleep Apnea and Sleep Problems in Children.)
Pathophysiology of Sleep
There are 2 states of sleep, each marked by characteristic physiologic changes:
Nonrapid eye movement (NREM): NREM sleep constitutes approximately 75 to 80% of total sleep time in adults. Heart rate and body temperature tend to decrease. NREM sleep consists of 3 stages (N1 to N3) in increasing depth of sleep. Slow, rolling eye movements, which characterize quiet wakefulness and early stage N1 sleep, disappear in deeper sleep stages. Muscle activity also decreases. Stage N2 sleep is characterized by K complexes (high-amplitude short spikes, which look like a QRS complex on an EKG) and sleep spindles (rhythmic high-frequency brainwave oscillations lasting 0.5 to 3 seconds in the shape of a football on an EEG) (see figure Nonrapid Eye Movement [NREM] EEG). Stage N3 is referred to as deep sleep because arousal threshold is high; people may perceive this stage as high-quality sleep.
Rapid eye movement (REM): REM sleep follows each cycle of NREM sleep. It is characterized by low-voltage fast activity on the EEG and postural muscle atonia. Respiration rate and depth fluctuate dramatically. Most dreams occur during REM sleep. Normally, 20 to 25% of sleep is REM.
Progression through the 3 stages, typically followed by a brief interval of REM sleep, occurs cyclically 5 to 6 times a night (see figure ). Brief periods of wakefulness (stage W) occur periodically.
Nonrapid Eye Movement (NREM) EEG
These EEG tracings show characteristic theta waves, sleep spindles, and K complexes during stages 1 (N1), 2 (N2), and 3 (N3) NREM sleep. |


Rapid Eye Movement (REM) EEG
This figure includes an EEG tracing (showing characteristic sawtooth waves) and an eye tracing (showing rapid eye movements), which occur during REM sleep. In the bottom panel, the arrows represent sharply peaked conjugate eye movements from the right and left eyes during REM sleep. |

Individual sleep requirements vary widely, ranging from 6 to 10 hours/24 hours. Infants sleep a large part of the day; with aging, total sleep time and deep sleep (stage N3) tend to decrease, and sleep becomes more interrupted. In older adults, stage N3 may disappear. These changes may account for increasing EDS and fatigue with aging, but their clinical significance is unclear.
Typical Sleep Pattern in Young Adults
Rapid eye movement (REM) sleep occurs cyclically throughout the night every 90–120 minutes. Brief periods of wakefulness (stage W) occur periodically. Sleep time is spent as follows:
|


Etiology of Sleep or Wakefulness Disorders
Some disorders can cause either insomnia or EDS (and sometimes both), and some cause only one or the other (see table ).
Some Causes of Insomnia and Excessive Daytime Sleepiness
Disorder | Insomnia | Excessive Daytime Sleepiness |
|---|---|---|
√ | ||
√ | √ | |
√ | √ | |
Drug-dependent and drug-induced sleep disorders | √ | √ |
Inadequate sleep hygiene | √ | √ |
√ | ||
√ | ||
√ | √ | |
√ | √ | |
√ | √ | |
√ | ||
√ | ||
√ = commonly present (but insomnia and/or excessive daytime sleepiness can occur in any of these disorders). | ||
Insomnia is most often caused by
An insomnia disorder (eg, adjustment sleep disorder, psychophysiologic insomnia)
Inadequate sleep hygiene
Psychiatric disorders, particularly mood, anxiety, and substance use disorders
Miscellaneous medical disorders such as cardiopulmonary disorders, musculoskeletal conditions, and chronic pain
EDS is most often caused by
Miscellaneous medical, neurologic (eg, narcolepsy, periodic limb movement disorder, and psychiatric disorders)
Circadian rhythm sleep disorders such as jet lag and shift work sleep disorders
Inadequate sleep hygiene refers to behaviors that are not conducive to sleep. They include
Consumption of caffeine or sympathomimetic or other stimulant drugs (typically near bedtime, but even in the afternoon for people who are particularly sensitive)
Exercise or excitement (eg, a thrilling television show, sports event) late in the evening
An irregular sleep-wake schedule
Patients who compensate for lost sleep by sleeping late or by napping may further fragment their nocturnal sleep.
Adjustment insomnia results from acute emotional stressors (eg, job loss, hospitalization, loss of a family member) that disrupt sleep.
Psychophysiologic insomnia is insomnia (regardless of cause) that persists well beyond resolution of precipitating factors, usually because patients feel anticipatory anxiety about the prospect of another sleepless night followed by another day of fatigue. Typically, patients spend hours in bed focusing on and brooding about their sleeplessness, and they have greater difficulty falling asleep in their own bedroom than falling asleep away from home.
Physical disorders that cause pain or discomfort (eg, arthritis, cancer, herniated discs), particularly those that worsen with movement, can cause transient awakenings and poor sleep quality. Nocturnal seizures can also interfere with sleep.
Most major mental disorders are associated with EDS and insomnia. Approximately 80% of patients with major depression report EDS and insomnia; conversely, 40% of patients with chronic insomnia have a major mental disorder, most commonly a mood disorder (1).
Insufficient sleep syndrome involves not sleeping enough at night despite adequate opportunity to do so, typically because of various social or employment commitments.
Drug-related sleep disorders result from chronic use of or withdrawal from various medications, illicit drugs, or other substances.
Circadian rhythm sleep disorders result in misalignment between endogenous sleep-wake rhythms and environmental light-darkness cycle. The cause may be external (eg, jet lag disorder, shift work disorder) or internal (eg, delayed or advanced sleep phase disorder).
Central sleep apnea consists of repeated episodes of breathing cessation or shallow breathing during sleep, lasting at least 10 seconds and caused by diminished respiratory effort. The disorder typically manifests as disturbed and unrefreshing sleep.
Obstructive sleep apnea consists of episodes of partial or complete closure of the upper airway during sleep, leading to cessation of breathing for ≥ 10 seconds. Most patients snore, and sometimes patients awaken, gasping. These episodes disrupt sleep and result in unrefreshing sleep and EDS.
Narcolepsy is characterized by chronic EDS. There are 2 types of narcolepsy. Type 1 narcolepsy is often accompanied by cataplexy, sleep paralysis, and hypnagogic or hypnopompic hallucinations:
Cataplexy is momentary (seconds to a few minutes) muscular weakness or paralysis without loss of consciousness that is evoked by sudden emotional reactions (eg, laughter, anger, fear, joy, surprise). Weakness may be confined to the limbs (eg, patients may drop the rod when a fish strikes their line) or may cause a limp fall during hearty laughter (as in “weak with laughter”) or sudden anger. Cataplexy can also manifest as blurred vision, knee buckling, or slurred speech.
Sleep paralysis is the momentary inability to move when just falling asleep or immediately upon awakening.
Hypnagogic and hypnopompic phenomena are vivid auditory, tactile, or visual illusions or hallucinations that occur when just falling asleep (hypnagogic) or, less often, immediately after awakening (hypnopompic).
Periodic limb movement disorder is characterized by repetitive (usually every 20 to 40 seconds) twitching or kicking of the lower or upper extremities during sleep. Patients usually complain of interrupted nocturnal sleep or EDS. They are typically unaware of the movements and brief arousals that follow, and they have no abnormal sensations in the extremities.
Restless legs syndrome is characterized by an irresistible urge to move the legs and, less frequently, the arms, usually accompanied by paresthesias (eg, creeping or crawling sensations) in the limbs when reclining. To relieve symptoms, patients move the affected extremity by stretching, kicking, or walking. As a result, they have difficulty falling asleep, repeated nocturnal awakenings, or both.
Etiology reference
1. Geoffroy PA, Hoertel N, Etain B, et al. Insomnia and hypersomnia in major depressive episode: Prevalence, sociodemographic characteristics and psychiatric comorbidity in a population-based study. J Affective Dis. 226:132-141.doi.org/10.1016/j.jad.2017.09.032
Evaluation of Sleep or Wakefulness Disorders
History
History of present illness should include duration and age at onset of symptoms and any events (eg, a life or work change, new medication, new medical disorder) that coincided with onset. Symptoms during sleeping and waking hours should be noted.
The quality and quantity of sleep are identified by determining
Bedtime
Latency of sleep (time from bedtime to falling asleep)
Number and time of awakenings
Final morning awakening and arising times
Frequency and duration of naps
Quality of sleep (whether it is refreshing)
Having patients keep a sleep log for several weeks is more accurate than questioning them. Bedtime events (eg, food or alcohol consumption, physical or mental activity) should be evaluated. Intake of and withdrawal from medications, alcohol, caffeine, marijuana, and nicotine as well as level and timing of physical activity should also be included.
If excessive daytime sleepiness is the problem, severity should be quantified based on the propensity for falling asleep in different situations (eg, resting comfortably versus when driving a car). The Epworth Sleepiness Scale may be used; a cumulative score ≥ 10 represents excessive daytime sleepiness.
Review of systems should check for symptoms of specific sleep disorders, including
Snoring, interrupted breathing patterns, witnessed apneic events, nocturnal gasping and choking, and nocturia (sleep apnea syndromes)
Depression, anxiety, mania, and hypomania (psychiatric sleep disorders)
Restlessness in the legs, an irresistible desire to move them, and jerking leg or arm movements (restless legs syndrome, periodic limb movement disorder)
Cataplexy, sleep paralysis, and hypnagogic hallucinations (narcolepsy)
Bed partners or other family members can best identify some of these symptoms.
Past medical history should check for known disorders that can interfere with sleep, including chronic obstructive pulmonary disease (COPD), asthma, heart failure, hyperthyroidism, gastroesophageal reflux, neurologic disorders (particularly movement and degenerative disorders), urinary incontinence, other urinary disorders, and painful disorders (eg, rheumatoid arthritis). Risk factors, symptoms, and diseases associated with obstructive sleep apnea include obesity, heart disorders, hypertension, stroke, smoking, snoring, retrognathia, tonsillar hypertrophy, and macroglossia. Drug history should include questions about use of any medications, substances, or caffeinated beverages associated with sleep disturbance.

Physical examination
The physical examination is useful mainly for identifying signs associated with obstructive sleep apnea:
Obesity with fat distributed around the neck or midriff
Large neck circumference (≥ 43.2 cm [17 in] in males, ≥ 40.6 cm [16 in] in females)
Mandibular hypoplasia and retrognathia
Nasal obstruction
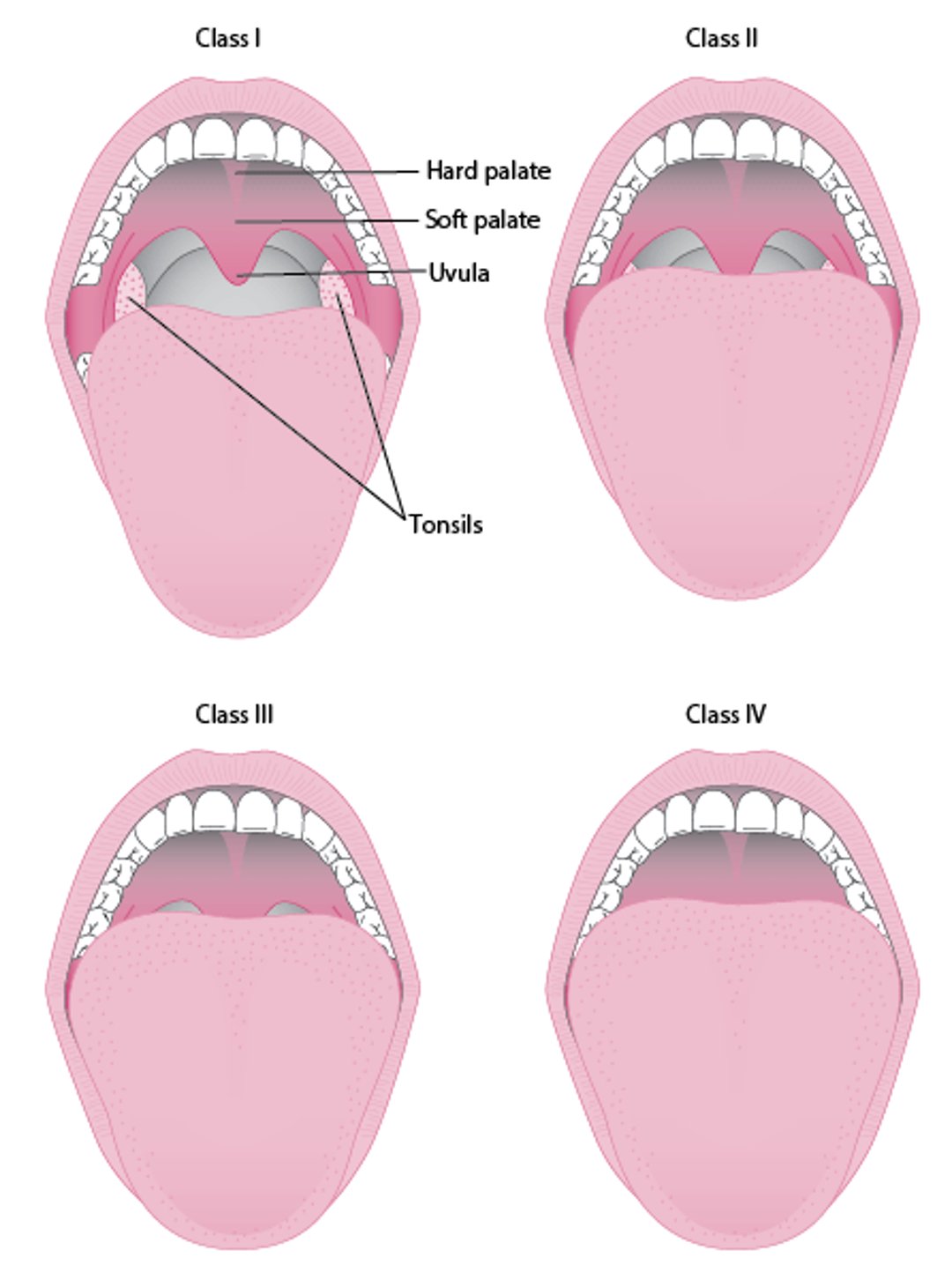
Enlarged tonsils (palatine or lingual), adenoid, tongue, uvula, lateral walls of the pharynx or soft palate (modified Mallampati score 3 or 4—see figure Modified Mallampati Scoring)
Decreased pharyngeal patency
Redundant lateral pharyngeal mucosa
Modified Mallampati Scoring
Modified Mallampati scoring is as follows:
|

The chest should be examined for expiratory wheezes and kyphoscoliosis. Signs of right ventricular failure, including lower-extremity edema, should be noted. A thorough neurologic examination should be performed.
Red flags
The following findings are of particular concern:
Falling asleep while driving or other potentially dangerous situations
Repeated sleep attacks (falling asleep without warning)
Breathing interruptions or awakening with gasping reported by bed partner
Unstable cardiac or pulmonary status
Recent stroke
Status cataplecticus (continuous cataplexy attacks)
History of violent behaviors or injury to self or others during asleep
Frequent sleepwalking or other out-of-bed behavior
Interpretation of findings
Inadequate sleep hygiene and situational stressors are usually apparent in the history. EDS that disappears when sleep time is increased (eg, on weekends or vacations) suggests inadequate sleep syndrome. EDS that is accompanied by cataplexy, hypnagogic/hypnopompic hallucinations, or sleep paralysis suggests narcolepsy.
Difficulty falling asleep (sleep-onset insomnia) should be distinguished from difficulty maintaining sleep and early awakening (sleep maintenance insomnia).
Sleep-onset insomnia suggests delayed sleep phase syndrome, chronic psychophysiologic insomnia, restless legs syndrome, or childhood phobias.
Sleep maintenance insomnia suggests major depression, central sleep apnea, obstructive sleep apnea, periodic limb movement disorder, or aging.
Falling asleep early and awakening early suggest advanced sleep phase syndrome.
Clinicians should suspect obstructive sleep apnea in patients with significant snoring, frequent awakenings, and other risk factors. The STOP-BANG score can help predict risk of obstructive sleep apnea (see table ).
STOP-BANG Risk Score* for Obstructive Sleep Apnea
Item Evaluated | Finding |
|---|---|
Snoring | Loud snoring (louder than talking or loud enough to be heard through a closed door) |
Tired | Often fatigue or sleepiness during the daytime |
Observed | Observed to stop breathing during sleep |
BP | High blood pressure or current treatment for hypertension |
BMI | > 35 kg/m2 |
Age | > 50 years |
Neck circumference (typically measured at the bottom of the Adam's apple) | > 40 cm (> 15 3/4 in) |
Gender | Male |
* ≥ 3 or 4 findings = high risk of OSA. < 3 findings = low risk of OSA. | |
BMI = body mass index; OSA = obstructive sleep apnea. | |
Testing
Sleep tests are usually performed when specific symptoms or signs suggest obstructive sleep apnea, nocturnal seizures, narcolepsy, periodic limb movement disorder, or other disorders whose diagnosis relies on identification of characteristic polysomnographic findings. If symptoms or signs strongly suggest certain causes (eg, restless legs syndrome, poor sleep habits, transient stress, shift work disorder), testing is not required.
Polysomnography is particularly useful when obstructive sleep apnea, narcolepsy, nocturnal seizures, periodic limb movement disorder, or parasomnias are suspected. It also helps clinicians evaluate violent and potentially injurious sleep-related behaviors (REM behavioral disorder). It monitors brain activity (via EEG), eye movements, heart rate, respirations, oxygen saturation, and muscle tone and activity during sleep. Video recording is used to identify abnormal movements during sleep (1). Polysomnography is typically performed in a sleep laboratory; home sleep studies are now commonly used to diagnose obstructive sleep apnea, but not other sleep disorders (1–3).
Multiple sleep latency testing assesses the latency of sleep onset in 4 to 5 daytime nap opportunities 2 hours apart during the patient’s typical daytime. Patients lie in a darkened room and are asked to sleep. Onset and stage of sleep (including REM) are monitored by polysomnography to determine the degree of sleepiness. This test’s main use is in the diagnosis of narcolepsy.
For the maintenance of wakefulness test, patients are asked to stay awake in a quiet room during 4 wakefulness opportunities 2 hours apart while they sit in a bed or a recliner.
Patients with EDS may require laboratory tests of renal, liver, and thyroid function.
Evaluation references
1. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3):479-504. Published 2017 Mar 15. doi:10.5664/jcsm.6506
2. Rosen IM, Kirsch DB, Chervin RD, et al. Clinical use of a home sleep apnea test: An American Academy of Sleep Medicine Position Statement. J Clin Sleep Med. 13 (10):1205-1207, 2017. doi: 10.5664/jcsm.6774
3. Veasey SC, Rosen IM. Obstructive Sleep Apnea in Adults. N Engl J Med. 2019;380(15):1442-1449. doi:10.1056/NEJMcp1816152
Treatment of Sleep or Wakefulness Disorders
Specific conditions are treated. The primary treatment for insomnia is cognitive-behavioral therapy (CBT), when available, instead of hypnotics (1). Good sleep hygiene, which is important whatever the cause, is a component of cognitive-behavioral therapy and is often the only treatment patients with mild insomnia need.
Cognitive-behavioral therapy
Cognitive-behavioral therapy for insomnia focuses on managing the common thoughts, worries, and behaviors that interfere with sleep. It is typically performed in 4 to 8 individual or group sessions and can be performed face-to-face, via telehealth remotely, or digitally. Most studies show that telehealth is noninferior to in-person CBT-I (2, 3). Digital CBT-I is also effective, compared to sleep hygiene education (4), but more data are needed to compare its effectiveness to other modes of CBT.
Cognitive-behavioral therapy for insomnia consists of the following:
Helping patients improve sleep hygiene, particularly restricting time spent in bed, establishing a regular sleep schedule, and controlling stimuli
Teaching patients about the effects of sleeplessness and helping them identify inappropriate expectations about how much sleep they should get
Teaching patients relaxation techniques
Using other cognitive therapy techniques as needed
Restricting the amount of time spent in bed aims to limit the time patients spend lying in bed trying unsuccessfully to sleep. Initially, time in bed is limited to the average nightly total sleep time, but not to < 5.5 hours. Patients are asked to get out of bed in the morning at a fixed time and then calculate a bed time based on total sleep time and remaining awake until that time (called sleep restriction therapy). After a week, this approach typically improves quality of sleep. Then, the time spent in bed can be increased by gradually making bed time earlier, as long as awakenings in the middle of the night remain minimal.
Sleep Hygiene
Measure | Implementation |
|---|---|
Regular sleep/wake schedule | Bedtime and particularly wake-up time should be the same each day, including weekends. Patients should not spend excessive time in bed. |
Appropriate use of the bed | Limiting time in bed improves sleep continuity. If unable to fall sleep within 20 minutes, patients should get out of bed and return when sleepy. The bed should not be used for activities other than sleep or sex (eg, not for reading, eating, watching television, reviewing email, working on a computer, or paying bills). |
Avoidance of daytime naps, except by shift workers and patients with narcolepsy | Daytime naps may aggravate sleeplessness in patients with insomnia. However, naps decrease the need for stimulants in patients with narcolepsy and improve performance in shift workers. Naps should be taken at the same time each day and limited to 30 minutes. |
Regular routine before bedtime | A pattern of activities—brushing teeth, washing, setting the alarm clock—can set the mood for sleep. Bright lights and blue light (eg, with phones, televisions, computer screens) should be avoided before bedtime and during nocturnal awakenings. |
Sleep-conducive environment | The bedroom should be dark, quiet, and reasonably cool; it should be used only for sleep and sexual activity. Heavy curtains or a sleep mask can eliminate light, and earplugs, fans, or white-noise devices can help eliminate disturbing noise. |
Pillows | Pillows between the knees or under the waist can increase comfort. For patients with back problems, helpful positions include lying supine with a large pillow under the knees and sleeping on one side with a pillow between the knees. |
Regular exercise | Exercise promotes sleep and reduces stress, but if performed in the late evening, it can stimulate the nervous system and interfere with falling asleep. |
Relaxation | Stress and worry interfere with sleep. Reading or taking a warm bath before bedtime can aid relaxation. Techniques such as visual imagery, progressive muscle relaxation, and breathing exercises can be used. Patients should not watch the clock. |
Avoidance of stimulants and diuretics | Drinking alcoholic or caffeinated beverages, smoking, eating caffeinated foods (eg, chocolate), and taking appetite suppressants or diuretics—especially near bedtime—should be avoided. |
Bright light exposure while awake | Light exposure during the day can help rectify circadian rhythms, but if light exposure is too close to bedtime, it can interfere with sleep. Not using devices that have blue light a few hours before bedtime is recommended. |
Hypnotics
General guidelines for use of hypnotics (see table ) aim at minimizing misuse and addiction.
Guidelines for the Use of Hypnotics
Define a clear indication and treatment goal. |
Prescribe the lowest effective dose. |
Except for specific hypnotics and patients, limit duration of use to a few weeks. |
Individualize the dose for each patient. |
Use lower doses in patients also taking a central nervous system depressant, in older adults, and in patients with hepatic or renal disorders. |
Avoid* if patients have sleep apnea or respiratory disorders or a history of sedative misuse, if they drink alcohol, or if they are pregnant. |
For patients who need longer-term treatment, consider intermittent therapy. |
Avoid abruptly stopping the hypnotic if possible (ie, taper it). |
Reevaluate hypnotic treatment regularly; assess efficacy and adverse events. |
* Ramelteon is an exception; it can be given to patients with mild to moderate obstructive sleep apnea or chronic obstructive pulmonary disease (COPD) or a history of sedative misuse. Low-dose doxepin also has no abuse liability. |
For commonly used hypnotics, see table . All hypnotics (except ramelteon, low-dose doxepin, and orexin receptor antagonists) act at the benzodiazepine recognition site on the gamma-aminobutyric (GABA) receptor and augment the inhibitory effects of GABA.
Hypnotics differ primarily in elimination half-life and onset of action. Medications with a short half-life are used for sleep-onset insomnia. Medications with a longer half-life are useful for both sleep-onset and sleep maintenance insomnia, or, in the case of low-dose doxepin, primarily for sleep maintenance insomnia. Some hypnotics (eg, older benzodiazepines) have greater potential for daytime carryover effects, especially after prolonged use and/or in older adults. Newer medications with a very short duration of action (eg, low-dose sublingual zolpidem) can be taken in the middle of the night, during a nocturnal awakening, as long as patients stay in bed for at least 4 hours after use. Zolpidem can have serious side effects including fall risk, memory impairment, and complex sleep behaviors (sleep-walking, sleep-driving, and sleep-texting).
Patients who experience daytime sedation, incoordination, or other daytime effects should avoid activities requiring alertness (eg, driving), and the dose should be reduced, the medication stopped, or, if needed, another medication used. Other adverse effects include amnesia, hallucinations, incoordination, and falls. Falling is a significant risk with all hypnotics.
When benzodiazepines are to be stopped, they should be tapered and not stopped abruptly.
Oral Hypnotics in Common Use
Medication | Half Life* (hours) | Comments |
|---|---|---|
Benzodiazepine receptor agonists: Benzodiazepines | ||
Triazolam | 1.5−5.5 | May cause anterograde amnesia; high likelihood of tolerance and rebound after repeated use |
Temazepam | 9.5–12.4 | Longest latency for sleep induction |
Estazolam | 10–24 | Effective for sleep induction and maintenance |
Quazepam | 39–100 | High lipophilicity, which may mitigate residual sedation in first 7–10 days of continuous use |
Flurazepam | 47–100 | High risk of next-day residual sedation; not recommended for older adults |
Benzodiazepine receptor agonists: Nonbenzodiazepines | ||
Zaleplon | 1 | Ultrashort-acting; can be given for sleep-onset insomnia or after nocturnal awakening (if patients can spend at least 4 hours in bed after taking the medication) When given at normal bedtime, least likely to have residual effects |
Zolpidem, tablets | 2.5 | Effective for sleep-onset insomnia only |
Zolpidem oral spray | 2.7 | Used for sleep-onset insomnia; has a rapid onset of action |
Zolpidem, extended-release | 2.8 | Effective for sleep-onset insomnia and sleep maintenance insomnia; no tolerance with up to 6 months of use 3 to 7 nights/week |
Zolpidem, sublingual | 2.9 | More rapid onset of action than zolpidem tablets Higher doses used for sleep-onset insomnia Lower doses used for early awakening (should not be taken unless patients can spend at least 4 hours in bed after taking the medication) |
Eszopiclone | 6 | Effective for sleep-onset insomnia and sleep maintenance insomnia; no tolerance with up to 6 months nightly use |
Melatonin receptor agonists | ||
Tasimelteon | 0.9–1.7 | Can increase nighttime sleep duration and decrease daytime sleep duration in totally blind patients who have non–24-hour sleep-wake syndrome Can cause headaches and abnormal dreams or nightmares (most common adverse effects); no apparent abuse liability |
Ramelteon | 1–5 | Useful only for sleep-onset insomnia; one of a few hypnotics that are not associated with abuse liability Can be safely given to patients with mild to moderate obstructive sleep apnea or chronic obstructive pulmonary disease (COPD) No difficulties with long-term use |
Orexin receptor antagonists | ||
Daridorexant | About 8 | Used for sleep-onset and/or sleep maintenance insomnia Can cause headaches, somnolence, fatigue (most common), and suicidal ideation, worsening of depression, sleep paralysis, and complex sleep-related behaviors (eg, sleepwalking, sleep driving) |
Lemborexant | 17 (with 5 mg) 19 (with 10 mg) | Used for sleep-onset and/or sleep maintenance insomnia Can cause somnolence (most common) and suicidal ideation, worsening of depression, sleep paralysis, and complex sleep-related behaviors (eg, sleepwalking, sleep driving) Contraindicated in patients with narcolepsy |
Suvorexant | 12 | Useful for sleep-onset and maintenance insomnia Use lowest effective dose; may be increased to a maximum of 20 mg once a day if the 10-mg dose is well-tolerated but not effective |
Tricyclic antidepressant | ||
Doxepin, ultra low dose | 15.3 | Indicated for sleep maintenance insomnia; no abuse liability |
* Includes parent and active metabolites. Arranged in order from shortest to longest half-life. | ||
Three dual orexin receptor antagonists (daridorexant, lemborexant, suvorexant) can be used to treat sleep-onset and maintenance insomnia. They block orexin receptors in the brain, thereby blocking orexin-induced wakefulness signals and enabling sleep initiation. Dual orexin receptor antagonists block orexin receptors-1 and -2. The orexin receptor-1 is involved in suppressing the onset of rapid eye movement (REM) sleep; the orexin receptor-2 is involved in suppressing non-REM sleep onset and, to some extent, in controlling REM sleep. However, the mechanism of action for dual orexin receptor antagonists is not fully understood. They are used to treat sleep-onset and/or sleep-maintenance insomnia and may improve cognitive performance in patients with mild cognitive impairment or Alzheimer disease (5).
Daridorexant is taken once a day within 30 minutes of going to bed (has the shortest half-life [8 hours] of the dual oxexin receptor antagonists)
Lemborexant is taken once a day within 30 minutes of going to bed (can be increased based on patient response and tolerability)
Suvorexant is taken no more than once a night and taken within 30 minutes of going to bed, with at least 7 hours before the planned time of awakening (somnolence is most common adverse effect)
Low-dose doxepin (3 mg, 6 mg), a tricyclic antidepressant with antihistaminic activity, is also indicated for sleep maintenance insomnia. Doxepin has not been directly compared with other hypnotics, but a risk-benefit analysis suggested it had the most favorable profile when making indirect comparisons with other hypnotics (6). Doxepin is potentially the best first-line therapy (6).
Hypnotics should be used cautiously in patients with pulmonary insufficiency. In older patients, any hypnotic, even in small doses, can cause restlessness, excitement, falls, or exacerbation of delirium and dementia. Rarely, hypnotics can cause complex sleep-related behaviors, such as sleepwalking and even sleep driving; use of higher-than-recommended doses and concurrent consumption of alcoholic beverages may increase risk of such behaviors. Rarely, severe allergic reactions occur.
Prolonged use of hypnotics is typically discouraged because tolerance can develop and because abrupt discontinuation can cause rebound insomnia or even anxiety, tremor, and seizures. These effects are more common with benzodiazepines (particularly triazolam) and less common with nonbenzodiazepines. Difficulties can be minimized by using the lowest effective dose for brief periods and by tapering the dose before stopping the medication (see also Withdrawal and detoxification).
Other medications and substances used to treat insomnia
Many medications and substances not specifically indicated for insomnia are used to induce and maintain sleep (7).
Some antidepressants (other than low-dose doxepin) taken in low doses at bedtime (eg, paroxetine 5 to 20 mg, trazodone 50 mg, trimipramine 75 to 200 mg) may improve sleep because of their sedating side effects. However, their use in these low doses should be limited to when standard hypnotics are not tolerated (rare) or in higher (antidepressant) doses when depression is present.
Melatonin is a hormone that is secreted by the pineal gland (and that occurs naturally in some foods). Darkness stimulates secretion, and light inhibits it. By binding with melatonin receptors in the suprachiasmatic nucleus, melatonin mediates circadian rhythms, especially during physiologic sleep onset.
Oral melatonin (typically 0.5 to 5 mg at bedtime) may be effective for sleep problems due to delayed sleep phase syndrome. When used to treat this disorder, it must be taken at the appropriate time (a few hours before the evening increase in endogenous melatonin secretion—in early evening for most people, typically 3 to 5 hours before the intended bedtime); taken at the wrong time, it can aggravate sleep problems. There are delayed-release preparations of melatonin but it is not clear if these preparations are more effective than the normal-release versions.
For other forms of insomnia, melatonin's efficacy is largely unproved.
Melatonin can cause headache, dizziness, nausea, and drowsiness. However, after widespread use, no other worrisome adverse effects have been reported. Available preparations of melatonin are unregulated, so content and purity cannot be ensured, and the effects of long-term use are unknown.
Over-the-counter (OTC) antihistamines (eg, doxylamine, diphenhydramine) can induce sleep but should not be used to treat insomnia. Efficacy is unpredictable. Additionally, these agents have a long half-life and are associated with adverse effects (daytime sedation, confusion, urinary retention, and other systemic anticholinergic effects), which are particularly worrisome in older adults.
Alcohol should also not be used to help with sleep because it produces unrefreshing, disturbed sleep with frequent nocturnal awakenings, often increasing daytime sleepiness. Alcohol can further impair respiration during sleep in patients with obstructive sleep apnea and other pulmonary disorders such as chronic obstructive pulmonary disease (COPD).
Cannabinoids include the following (8):
CBD oil (cannabidiol), which causes sedation and reduced sleep latency but no euphoria
CBN (cannabinol), which causes sedation, reduces pain, and increases appetite
THC (tetrahydrocannabinol), which causes euphoria, reduces pain and nausea, and has variable effects on sleep stages
Dronabinol, which is a synthetic analog
Whether cannabis is effective for insomnia is unclear, but it is useful for chronic pain.
Tolerance can develop; stopping cannabis after long-term use results in insomnia.
Treatment references
1. Qaseem A, Kansagara D, Forciea MA, C et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 165(2):125-133, 2016. doi: 10.7326/M15-2175
2. Arnedt JT, Conroy DA, Mooney A, et al. Telemedicine versus face-to-face delivery of cognitive behavioral therapy for insomnia: a randomized controlled noninferiority trial. Sleep. 44(1):zsaa136, 2021. doi: 10.1093/sleep/zsaa136
3. Gehrman P, Gunter P, Findley J, et al. Randomized noninferiority trial of telehealth delivery of cognitive behavioral treatment of insomnia compared to in-person care. J Clin Psychiatry. 82(5):20m13723, 2021. doi: 10.4088/JCP.20m13723
4. Espie CA, Emsley R, Kyle SD, et al. Effect of Digital Cognitive Behavioral Therapy for Insomnia on Health, Psychological Well-being, and Sleep-Related Quality of Life: A Randomized Clinical Trial. JAMA Psychiatry. 2019;76(1):21-30. doi:10.1001/jamapsychiatry.2018.2745
5. Zhou M, Tang S. Effect of a dual orexin receptor antagonist on Alzheimer's disease: Sleep disorders and cognition. Front Med (Lausanne). 9:984227, 2023. doi: 10.3389/fmed.2022.984227
6. Cheung JMY, Scott H, Muench A, et al. Comparative short-term safety and efficacy of hypnotics: A quantitative risk-benefit analysis. J Sleep Res. e14088, 2023. doi: 10.1111/jsr.14088
7. Winkelman JW. CLINICAL PRACTICE. Insomnia Disorder. N Engl J Med. 2015;373(15):1437-1444. doi:10.1056/NEJMcp1412740
8. Hsu M, Shah A, Jordan A, Gold MS, Hill KP. Therapeutic Use of Cannabis and Cannabinoids: A Review. JAMA. 2026;335(4):345-359. doi:10.1001/jama.2025.19433
Key Points
Poor sleep hygiene and situational disruptors (eg, shift work, emotional stressors) are common causes of insomnia.
Consider medical disorders (eg, sleep apnea syndromes, pain disorders) and psychiatric disorders (eg, mood disorders) as possible causes.
Usually, perform sleep studies (eg, polysomnography) when sleep apnea syndromes, periodic limb movements, or other sleep disorders are suspected.
Good sleep hygiene, sometimes as part of cognitive-behavioral therapy, is first-line treatment for insomnia.
Use hypnotics and sedatives with caution, especially in older adults.
Drug Information for the Topic





