





Urinary incontinence is involuntary loss of urine.
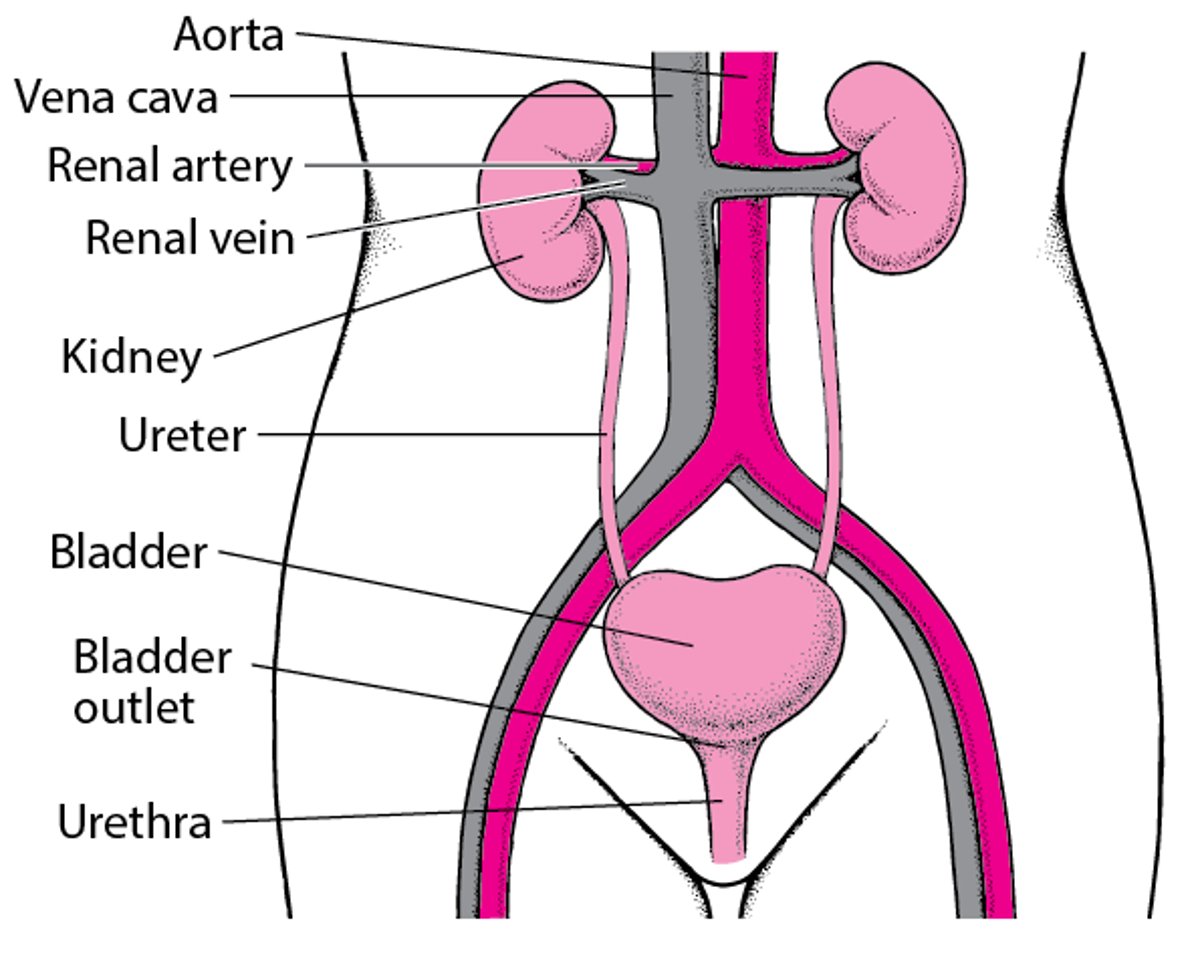
The Urinary Tract

Incontinence can occur in both men and women at any age, but it is more common among women and older adults, affecting about 37% of older women worldwide and 15% of older men in the United States. Although incontinence is more common among older adults, it is not a normal part of aging. (See also Control of Urination.) Incontinence may be sudden and temporary, as when a person is taking a medication that has a diuretic effect, or it may be long lasting (chronic). Even chronic incontinence may sometimes be successfully treated.
Urinary incontinence in children is discussed separately.


Types of Incontinence
There are several types of incontinence:
Urge incontinence is uncontrolled urine leakage (of moderate to large volume) that occurs immediately after an urgent, irrepressible need to urinate. Getting up to urinate during the night (nocturia) and nocturnal incontinence are common.
Stress incontinence is urine leakage due to abrupt increases in intra-abdominal pressure (for example, those that occur with coughing, sneezing, laughing, bending, or lifting). Leakage volume is usually low to moderate.
Overflow incontinence is dribbling of urine from an overly full bladder. Volume is usually small, but leaks may be constant, resulting in large total losses.
Functional incontinence is loss of urine because of a problem with thinking or a physical impairment unrelated to the control of urination. For example, a person with dementia due to Alzheimer disease may not recognize the need to urinate or not know where the toilet is. People who are bedridden may be unable to walk to the toilet or reach a bedpan.
Often, however, a person has more than one type of incontinence. People are then described as having mixed incontinence.
Causes of Urinary Incontinence
Several mechanisms can lead to urinary incontinence. Often, more than one mechanism is present:
Weakness of the urinary sphincter or pelvic muscles (called bladder outlet incompetence)
Something blocking the exit path of urine from the bladder (called bladder outlet obstruction)
Spasm or overactivity of the bladder wall muscles (sometimes called overactive bladder)
Weakness or underactivity of the bladder wall muscles
Poor coordination of the bladder wall muscles with the urinary sphincter
An increase in the volume of urine
Functional problems
Weakness or underactivity of the bladder wall muscles, bladder outlet obstruction, or particularly both can lead to inability to urinate (urinary retention). Urinary retention can paradoxically lead to overflow incontinence because of leaking from an overly full bladder.
An increase in the volume of urine (for example, caused by diabetes, use of diuretics, or excessive intake of alcohol or caffeinated drinks) can increase the amount of urine lost with incontinence, trigger an episode of incontinence, or even cause temporary incontinence to develop. However, it should not cause chronic incontinence. Functional problems, which are conditions that affect the function of other organs in the body, commonly increase the volume of urine lost among people who are incontinent. However, functional problems are rarely the only cause of permanent incontinence.
Overall, the most common causes of incontinence are:
Pelvic muscle weakness in women as a result of childbirth
Bladder outlet obstruction in middle-aged men
Functional disorders such as stroke and dementia in older adults
Some Mechanisms of Incontinence
Mechanism | Examples |
|---|---|
Weakness of the urinary sphincter or pelvic muscles (bladder outlet incompetence) | Atrophic urethritis, atrophic vaginitis, or both Medications Pelvic muscle weakness (for example, caused by having had several vaginal deliveries or pelvic surgery) Prostate surgery (most often complete removal of the prostate) |
Blockage (bladder outlet obstruction) | Prostate enlargement (benign prostatic hyperplasia) or cancer Medications |
Overactivity of bladder wall muscles (overactive bladder) | Bladder irritation (for example, caused by infection, stones, or rarely cancer) Disorders that can affect brain centers that control urination (such as stroke, dementia, or multiple sclerosis) Cervical spondylosis or spinal cord dysfunction (which can put pressure on the spinal cord and thus impair bladder function) Bladder outlet obstruction |
Underactivity of bladder wall muscles | Nerve damage (for example, by herniated discs, other spinal cord disorders, surgery, tumors, injury, diabetes, or alcohol use disorder) Medications Longstanding bladder outlet obstruction In women, often no identifiable cause |
Poor coordination of the bladder wall with the sphincter muscles | Damage to spinal cord or brain nerve pathways to the bladder |
Functional problems | Dementia Depression Psychoactive medications that can decrease awareness of the need to urinate (for example, antipsychotic medications, benzodiazepines, medications that cause drowsiness such as sedatives and sleep aids, or tricyclic antidepressants) Restricted mobility (for example, caused by injury, weakness, restraints, stroke, other neurologic disorders, or musculoskeletal disorders) Situational limitations (such as not having a toilet nearby or traveling) |
Increase in the volume of urine | Disorders such as diabetes mellitus or arginine vasopressin deficiency (previously known as diabetes insipidus) Use of diuretics (usually furosemide, bumetanide) Excessive intake of caffeinated beverages (such as coffee, tea, cola, or some other soft drinks) or alcohol |
Some Medications That Can Cause Incontinence
Mechanism | Examples |
|---|---|
Weakness of the urinary sphincter or pelvic muscles (bladder outlet incompetence) | Alpha-adrenergic blockers (such as alfuzosin, doxazosin, prazosin, tamsulosin, or terazosin), which relax the urinary sphincter Hormone therapy (usually estrogen/progestin combination therapy taken by mouth), which can contribute to thinning of the pelvic muscles and supporting tissues Misoprostol, which relaxes the urinary sphincter |
Blockage (bladder outlet obstruction) | Alpha-adrenergic stimulants (such as pseudoephedrine), which can cause muscles in the bladder and prostate to contract |
Underactivity of bladder wall muscles | Medications with anticholinergic effects (such as antihistamines, antipsychotic medications, benztropine, or tricyclic antidepressants), which inhibit bladder muscle contractions Calcium channel blockers (such as diltiazem, nifedipine, or verapamil), which inhibit bladder muscle contractions Opioids, which seem to inhibit bladder contractility |
Did You Know...
|
Evaluation of Urinary Incontinence
Urinary incontinence usually does not indicate a disorder that is life threatening; nevertheless, incontinence may cause embarrassment or lead people to restrict their activities unnecessarily, contributing to a decline in quality of life. Also, rarely, sudden incontinence can be a symptom of a spinal cord disorder. The following information can help people decide when a doctor's evaluation is needed and help them know what to expect during the evaluation.
Warning signs
In people with urinary incontinence, certain symptoms and characteristics are cause for concern. They include:
Symptoms of spinal cord damage (for example, weakness in the legs or loss of sensation in the legs or around the genitals or anus)
When to see a doctor
People with warning signs should go to an emergency department at once. People without warning signs should let their doctor know about their incontinence when they have their next routine visit, or call their doctor to be seen sooner if their symptoms are very troublesome to them.
Most people are embarrassed to mention incontinence to their doctors. Some people believe that incontinence is a normal part of aging. However, incontinence, even incontinence that has been present for some time or that occurs in an older adult, may be helped by treatment. If symptoms of urinary incontinence are bothersome, interfere with activities of daily living, or cause people to curtail their social activities, people should see a doctor.
What the doctor does
Doctors first ask questions about the person's symptoms and medical history. Doctors then do a physical examination. What they find during the history and physical examination often suggests a cause of the incontinence and the tests that may need to be done.
Doctors ask questions about the circumstances of urine loss, including amount, time of day, and any precipitating factors (such as coughing, sneezing, or straining). People are asked whether they can sense the need to urinate and, if so, whether the sensation is normal or comes with sudden urgency. Doctors may also ask the person to estimate the amount of urine leakage. Doctors will also ask whether the person has any additional problems with urination, such as pain or burning during urination, a frequent need to urinate, difficulty starting urination, or a weak urine stream.
Sometimes doctors may ask people to keep a record of their urination habits over a day or two. This record is called a voiding diary. Each time the person urinates, the volume and time are recorded. After an episode of incontinence, the person also records any related activities, especially eating, drinking, medication use, or sleeping.
Doctors ask about whether the person has other disorders that are known to cause incontinence, such as dementia, stroke, urinary tract stones, spinal cord or other neurologic disorders, and prostate disorders. Doctors need to know what medications a person is taking because some medications cause or contribute to incontinence. Women are asked about number and types of deliveries and any complications. All are asked about previous pelvic and abdominal surgery, particularly prostate surgery in men.
The physical examination can help doctors narrow possible causes. Doctors test strength, sensation and reflexes in the legs, and sensation around the genitals and anus to detect nerve and muscle problems that may make it difficult for the person to remain continent.
In women, doctors do a pelvic examination to detect abnormalities that could cause incontinence, such as vaginal atrophy (menopausal changes in which the lining of the vagina becomes thinner, drier, and less elastic and may be accompanied by urinary tract changes) or weakness of pelvic muscles. In men and women, doctors do a rectal examination to look for signs of constipation or damage to the nerves supplying the rectum. In men, the rectal examination allows doctors to check the prostate because an enlarged prostate or occasionally prostate cancer can contribute to incontinence. The person may be asked to cough with a full bladder to detect whether stress incontinence is present. Women may be asked to repeat this procedure during a pelvic examination, to see whether supporting some pelvic structures (with the doctor's fingers) eliminates the leakage of urine.
Testing
Often findings during the physical examination can help doctors determine the cause or identify factors that contribute to incontinence. However, some tests are often needed so doctors can make a firm diagnosis. Routinely obtained tests include:
Blood tests of kidney function and sometimes others
Postvoid residual volume (a catheter or ultrasound is used to determine how much urine is left in the bladder after a person urinates)
Sometimes urodynamic testing

Urodynamic testing includes cystometry, urinary flow rate testing, and cystometrography and is done when the doctor's examination and the initial tests do not reveal the cause of incontinence.
Cystometry is done to confirm urge incontinence and to determine whether the cause is overactive bladder. A bladder catheter is placed through the urethra. A doctor measures how much water can be injected into the bladder until the person develops a sense of urgency or bladder contractions.
Peak urinary flow rate is measured in men to determine whether incontinence is caused by bladder outlet obstruction (usually caused by prostate disease). Men urinate into a special device (uroflowmeter) that measures the speed of urine flow and how much urine is released.
Cystometrography is done if all other evaluation fails to reveal the cause of incontinence. Cystometrography is a test that measures bladder pressures when the bladder is filled with various volumes of water. Cystometrography is often done with electromyography, a test that can assess sphincter function. In certain centers with specialized equipment, bladder contraction strength can also be measured at the same time as sphincter and other bladder pressures.
Although urodynamic testing is important, results do not always predict response to medication or indicate the relative importance of multiple causes.
Treatment of Urinary Incontinence
Treatment of specific causes
Sometimes medications to treat certain types of incontinence
General measures to reduce the inconvenience of incontinence
The specific cause of incontinence can often be treated. There are also general measures that doctors may suggest to all people to reduce the inconvenience of incontinence.
When a medication is causing a problem, doctors may be able to switch the person to a different medication or change the dosing schedule to provide relief (for example, a diuretic dose may be timed so that a bathroom is near when the medication takes effect). However, people should talk with their doctor before they stop taking a medication or change the amount or dosing schedule.
Medications are often useful for some types of incontinence but should supplement rather than replace general measures. Medications include those that relax the bladder wall muscle and those that increase sphincter tone. Medications that relax the urinary sphincter may be used to treat outlet obstruction in men with urge or overflow incontinence.
General measures
Regardless of the type and cause of incontinence, some general measures are usually helpful.
Modifying fluid intake
Bladder training
Pelvic muscle exercises
Fluid intake can be limited at certain times (for example, before going out or 3 to 4 hours before bedtime). Doctors may suggest that people avoid fluids that irritate the bladder (such as caffeine-containing fluids). However, people should drink 48 to 64 oz (1500 to 2000 mL) of fluid a day because concentrated urine irritates the bladder.
Bladder training is a technique that involves having the person follow a fixed schedule for urination while awake. The doctor works with the person to establish a schedule of urinating every 2 to 3 hours and suppressing the urge to urinate at other times (for example, by relaxing and breathing deeply). As the person becomes better able to suppress the urge to urinate, the interval is gradually lengthened. A similar technique, called prompted voiding, can be used by people who care for a person with dementia or other cognitive problems. With this technique, the person is asked whether they need to urinate and whether they are wet or dry at specific intervals.
Pelvic muscle exercises (Kegel exercises) are often effective, especially for stress incontinence. People must be certain to exercise the correct muscles, the muscles around the urethra and rectum that stop the flow of urine. The muscles are tightly squeezed for 1 to 2 seconds and then relaxed for about 10 seconds. The exercises are repeated about 10 times three times each day. People are gradually able to increase the time the muscles are tightly squeezed until the contraction is held for about 10 seconds each time. Because it can be difficult to learn to control the correct muscles, doctors may need to provide instruction or recommend the use of biofeedback or electrical stimulation (an electronic version of pelvic floor exercises in which an electric current is used to stimulate the correct muscles).
In addition to Kegel exercises, other pelvic floor exercises, often taught by a physical therapist, can help strenghten the pelvic floor and reduce incontinence.
Some Medications Used to Treat Urinary Incontinence
Medication | How It Works | Comments |
|---|---|---|
For weakness of the urinary sphincter or pelvic muscles (bladder outlet incompetence) causing stress incontinence | ||
Duloxetine | Helps strengthen contractions of the urinary sphincter | Not as thoroughly studied as many other medications Not approved for this use in the United States |
Imipramine (a tricyclic antidepressant) | Helps strengthen urinary sphincter contractions and relax an overactive bladder (an anticholinergic effect*) | Also used for overactive bladder and urge incontinence Used as temporary therapy for reducing nighttime incontinence (enuresis) in children aged 6 years and older |
Pseudoephedrine (an alpha-adrenergic stimulant) | Helps strengthen urinary sphincter contractions | Can cause anxiety, insomnia, and, in men, inability to urinate Over-the-counter medication used primarily as a decongestant |
For bladder outlet obstruction in men causing urge or overflow incontinence | ||
Alpha-adrenergic blockers:
| Help relax the urinary sphincter | Tend to increase the speed of urine flow and help the bladder empty more completely May decrease blood pressure or cause fatigue |
5-Alpha reductase inhibitors:
| Help shrink an enlarged prostate | Can take weeks or months to become effective Sometimes decrease sex drive or contribute to erectile dysfunction |
Phosphodiesterase type 5 (PDE5) inhibitor:
| Doctors are not certain how this medication affects an enlarged prostate | Low dose taken daily (also used to treat erectile dysfunction) |
For overactive bladder with urge or stress incontinence | ||
Darifenacin | Increases the bladder's filling capacity and decreases bladder wall muscle spasms (anticholinergic effects†) | — |
Dicyclomine | Relaxes involuntary muscles Increases the bladder's filling capacity and decreases bladder wall muscle spasms (anticholinergic effects*) | Not as thoroughly studied as many other medications |
Fesoterodine | Increases the bladder's filling capacity and decreases bladder wall muscle spasms (anticholinergic effects†) | Not as thoroughly studied as many other medications |
Hyoscyamine | Increases the bladder's filling capacity and decreases bladder wall muscle spasms (anticholinergic effects*) | Not as thoroughly studied as many other medications |
Imipramine (a tricyclic antidepressant) | Helps strengthen urinary sphincter contractions Increases the bladder's filling capacity and decreases bladder wall muscle spasms (an anticholinergic effect*) | Particularly useful for nighttime incontinence |
Mirabegron (a beta-adrenergic stimulant) | Relaxes the bladder wall | May increase blood pressure |
OnabotulinumtoxinA (a type of botulinum toxin) | Blocks the nerve activity in the bladder muscle that causes the bladder to contract involuntarily | Injected into the bladder wall through a cystoscope inserted in the bladder Used to treat incontinence in adults with overactive bladder caused by a neurologic disorder (such as multiple sclerosis) when other medications are ineffective or have too many side effects |
Oxybutynin | Many effects, such as relaxation of involuntary muscles and anticholinergic effects*, which include increasing the bladder's filling capacity and decreasing the bladder wall muscle spasms | May be the most effective medication Available as a tablet, skin patch, and gel |
Solifenacin | Increases the bladder's filling capacity and decreases bladder wall muscle spasms (anticholinergic effects†) | — |
Tolterodine | Increases the bladder's filling capacity and decreases bladder wall muscle spasms (anticholinergic effects†) | — |
Trospium | Increases the bladder's filling capacity and decreases bladder wall muscle spasms (anticholinergic effects*) | — |
Vibegron (a beta-adrenergic stimulant) | Relaxes the bladder wall | No apparent effect on blood pressure |
For weak bladder wall muscles with overflow incontinence | ||
Bethanechol | Helps bladder wall muscles contract | Usually ineffective Can cause flushing, abdominal cramps, and an increased heart rate |
* Anticholinergic effects (such as dry mouth, constipation, and sometimes blurred vision or confusion) can be bothersome, particularly in older adults. | ||
† These medications have anticholinergic effects that target the urinary system, so they tend to have fewer other anticholinergic side effects than other medications with anticholinergic effects. | ||
Urge incontinence
The goal is to relax the bladder wall muscles. Bladder training, Kegel exercises, and relaxation techniques are tried first. Biofeedback also can be tried. With the urge to urinate, the person can try relaxing, standing in place or sitting down, or tightening the pelvic muscles. The most commonly used medications are oxybutynin and tolterodine. Oxybutynin is available as a skin patch or skin gel as well as a pill. Mirabegron, vibegron, fesoterodine, solifenacin, darifenacin, and trospium are alternative medications.
If other treatments are ineffective for urge incontinence, further treatments can be tried, such as gentle electrical stimulation of the sacral nerves by a device similar to a pacemaker, instillation of chemicals into the bladder (when the cause is a spinal cord or brain disorder), or, rarely, surgery.
Stress incontinence
Treatment usually begins with bladder training and Kegel exercises. Avoiding physical stresses that cause loss of urine (for example, heavy lifting) and losing weight may help control incontinence. Pseudoephedrine may be useful in women with bladder outlet incompetence. Imipramine may be used for mixed stress and urge incontinence or for either separately. Duloxetine is also used for stress incontinence. If stress incontinence is caused by atrophic urethritis or atrophic vaginitis, estrogen cream is often effective. For people with stress incontinence, urinating frequently to avoid a full bladder is often helpful.
For stress incontinence that is not relieved with medications and behavioral measures, surgery or devices such as pessaries may be helpful. The vaginal sling procedure creates a hammock of support to help prevent the urethra from opening during coughing, sneezing, or laughing. Most commonly, a sling is created from synthetic mesh. Mesh implants are effective, but a few people with mesh implants have serious complications. Alternatively, doctors can create a sling using tissue from the abdominal wall or leg. Devices that may be tried in women include caps over the urethral meatus, pessaries and other intravaginal and intraurethral devices. In men with stress incontinence, a mesh sling or an artificial urinary sphincter implant may be placed around the urethra to prevent leakage of urine.
Overflow incontinence
Treatment depends on whether the cause is bladder outlet obstruction, weak bladder wall muscles, or both. For overflow incontinence caused by bladder outlet obstruction, specific treatments may help relieve obstruction (for example, surgery or medications for prostate disease, surgery for cystocele, and dilation or stenting for urethral narrowing).
For overflow incontinence caused by weak bladder wall muscles, treatments can include reducing the amount of urine in the bladder by intermittent insertion of a bladder catheter or, rarely, insertion of a catheter that remains in the bladder. The goal is to reduce the bladder's size, allowing its walls to regain some capacity to prevent it from overflowing. Other measures that can help empty the bladder after urinating include trying to urinate again after urination has ended (called double voiding), bearing down at the end of urination, and/or pressing over the lower abdomen at the end of urination. Occasionally, electrical stimulation can be used to help empty the bladder more completely.
Essentials for Older Adults: Urinary Incontinence
Although incontinence is more common among older adults, it is not a normal part of aging.
With aging, bladder capacity decreases, ability to delay urination declines, involuntary bladder contractions occur more often, and bladder contractions weaken. Thus, urination becomes more difficult to postpone and tends to be incomplete. The muscles, ligaments, and connective tissue of the pelvis weaken, contributing to incontinence. In postmenopausal women, decreased estrogen levels lead to atrophic urethritis and atrophic vaginitis and to decreasing the strength of the urethral sphincter. In men, prostate size increases, partially obstructing the urethra and leading to incomplete bladder emptying and strain on the bladder muscle. These changes occur in many normal, continent older adults and may facilitate incontinence but do not cause it.
Incontinence greatly reduces quality of life, causing embarrassment, isolation, and depression. Incontinence is often a reason older adults require care in a long-term care facility. Urine irritates the skin, contributing to the formation of pressure sores in people who are bedbound or chairbound. Older adults with urge incontinence are at increased risk of falls and fractures as they rush to the toilet.
The most effective medications for many kinds of incontinence have anticholinergic effects (see sidebar Anticholinergic: What Does It Mean?). These effects, such as constipation, dry mouth, blurred vision, and sometimes even confusion, can be particularly troublesome in older adults.
Key Points
Incontinence is common and can greatly reduce a person's quality of life, so people should be evaluated by a doctor.
Although incontinence is more common among older adults, it is not a normal consequence of aging.
Some causes are reversible, even if long-standing.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
Drug Information for the Topic





