



Diphtheria is an acute pharyngeal or cutaneous infection caused mainly by toxigenic strains of the gram-positive bacillus Corynebacterium diphtheriae and rarely by other, less common Corynebacterium species. Symptoms are either nonspecific skin infections or pseudomembranous pharyngitis followed by myocardial and neural tissue damage secondary to the exotoxin. An asymptomatic carrier state also exists. Diagnosis is based on a combination of characteristic clinical findings and confirmed by culture and testing for toxin; cultures should be repeated for confirmation of cure. Treatment is with antitoxin and penicillin, erythromycin, or azithromycin. Childhood vaccination and booster doses should be routine to prevent the infection.
Diphtheria is an acute bacterial infection caused mostly by toxin-producing Corynebacterium diphtheriae and rarely by toxin-producing strains of C. ulcerans and C. pseudotuberculosis. C. diphtheriae usually infects the nasopharynx (respiratory diphtheria) or skin (cutaneous diphtheria).
According to the Centers for Disease Control and Prevention's National Notifiable Diseases Surveillance System (NNDSS), the number of reported cases of diphtheria are extremely low (1). From 1996 to 2018, 14 cases and 1 death (in an older adult returning from an endemic area) were reported in the United States (2). Diphtheria is rare in places where childhood immunization is widespread. However, susceptibility, increases in places in which booster immunization rates in adults are declining. Infection with nontoxigenic C. diphtheriae is not prevented by vaccination and may also be increasing in areas of the United States (3).
Diphtheria may be present in returning travelers or migrants from countries where diphtheria is endemic. Diphtheria is endemic in many countries in Asia, the South Pacific, the Middle East, Eastern Europe, Venezuela, Haiti, and the Dominican Republic. Outbreaks in Indonesia, Thailand, Vietnam, Laos, Myanmar, South Africa, Sudan, India, and Pakistan have sporadically occurred in recent decades.
Diphtheria is a nationally notifiable disease in the United States. Clinicians with definitive cases should contact their state health department (4) or the CDC Emergency Operations Center (5) to connect with diphtheria subject matter experts for more information on all case investigations and to initiate investigations of close contacts (5). Outside the United States, clinicians should report confirmed cases to their local or national health authorities so that they may then notify the World Health Organization through established protocols.
Diphtheria toxin
Diphtheria strains infected by a beta-phage (a lysogenic bacteriophage that can replicate without immediately causing host-cell death), which carries a toxin-encoding gene (tox+), produce a potent toxin (6). Diphtheria toxin appears to use a growth-factor precursor as a receptor to initiate cell-binding and entry (7). This toxin first causes inflammation and necrosis of local tissues allowing for dissemination of toxin in the blood, which can then, upon binding and entry into host cells, damage the heart, nerves, and sometimes the kidneys (2).
Nontoxigenic strains of C. diphtheriae can also cause exudative pharyngitis, bacteremia, and sometimes systemic disease (eg, endocarditis, septic arthritis).
Transmission
Humans are the major reservoir for C. diphtheriae. Horses, cattle and domestic cats may also carry C. diphtheriae. The organism is spread by
Respiratory droplets
Contact with nasopharyngeal secretions (including from asymptomatic carriers)
Contact with infected skin lesions
Fomites (rare)
A carrier state is common in endemic regions but not in high-income countries. Immunity derived from vaccination or active infection may not prevent patients from becoming carriers; however, most patients who are adequately treated do not become carriers. Patients with clinical illness or asymptomatic carriers may transmit the infection.
Poor personal and communal hygiene contributes to the spread of cutaneous diphtheria.
General references
1. Centers for Disease Control and Prevention: Diphtheria: Diphtheria Surveillance and Trends. May 12, 2025. Accessed July 15, 2025.
2. Acosta AM, Moro PL, Hariri S, Tiwari TSP: Chapter 7: Diphtheria. In Centers for Disease Control and Prevention: Epidemiology and Prevention of Vaccine-Preventable Diseases (the "pink book").April 23, 2024. Accessed July 15, 2025.
3. Xie AG, Yomogida K, Berry I, et al. Notes from the Field: Increase in Nontoxigenic Corynebacterium diphtheriae - Washington, 2018-2023. MMWR Morb Mortal Wkly Rep. 2024;73(17):405-407. Published 2024 May 2. doi:10.15585/mmwr.mm7317a4
4. Centers for Disease Control and Prevention: Health Department Directories. May 15, 2024. Accessed July 15,
5. Centers for Disease Control and Prevention: Infectious Diseases Laboratories: Our Formulary. May 29, 2024. Accessed August 1, 2025.
6. Murphy JR. Corynebacterium Diphtheriae. In: Baron S, editor. Medical Microbiology. 4th edition. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 32. Available from: https://www.ncbi.nlm.nih.gov/books/NBK7971/
7. Naglich JG, Metherall JE, Russell DW, Eidels L. Expression cloning of a diphtheria toxin receptor: identity with a heparin-binding EGF-like growth factor precursor. Cell. 1992;69(6):1051-1061. doi:10.1016/0092-8674(92)90623-k
Symptoms and Signs of Diphtheria
Symptoms of diphtheria vary depending on:
The organ system or tissue affected
Strain toxigenicity
Most respiratory infections are caused by toxigenic strains. Cutaneous infections are caused by toxigenic and nontoxigenic strains. Toxin is poorly absorbed from the skin; thus, toxin complications are rare in cutaneous diphtheria.
Pharyngeal infection
After an incubation period, of between 2 and 5 days (range: 1 to 10 days) and a prodromal period of between 12 and 36 hours (1), patients develop mild sore throat, dysphagia, low-grade fever, and tachycardia. Nausea, emesis, chills, headache, and fever are more common among children (1). In untreated people, organisms can be present in discharges and lesions 2 to 6 weeks after infection.
If a toxigenic strain is involved, the characteristic pseudomembrane appears in the tonsillar area. It may initially appear as a white, glossy exudate but typically becomes dirty gray, tough, fibrinous, and adherent so that removal causes bleeding. The membrane may extend to the larynx, trachea, and bronchi and may partially obstruct the airway or suddenly detach, causing complete obstruction. Local edema may cause a visibly swollen neck (bull neck), hoarseness, stridor, and dyspnea.
If a large amount of toxin is absorbed, severe fatigue, pallor, tachycardia, stupor, and coma may occur; toxemia may cause death within 6 to 10 days.
Mild disease with a serosanguineous or purulent discharge and irritation of the external nares and upper lip occurs in patients who have only nasal diphtheria.

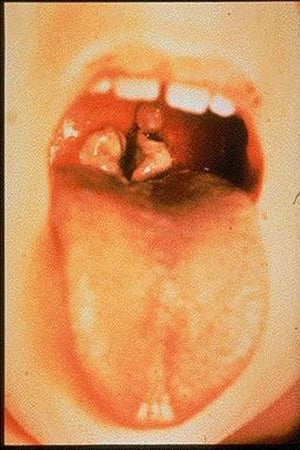
Toxigenic strains of Corynebacterium diphtheriae may cause a thick pharyngeal exudate. The exudate is dirty gray and is tough, fibrinous, and adherent to the mucosae.
Toxigenic strains of Corynebacterium diphtheriae may cause a thick pharyngeal exudate. The exudate is dirty gray and is
Image courtesy of the Centers for Disease Control and Prevention.

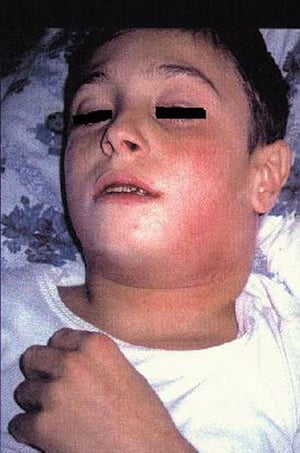
In acute nasopharyngeal diphtheria, local edema may cause a visibly swollen neck (bull neck).
In acute nasopharyngeal diphtheria, local edema may cause a visibly swollen neck (bull neck).
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

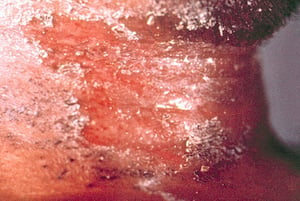
The scaling rash of cutaneous diphtheria, as seen on the neck in this image, may be indistinguishable from more common skin conditions, such as eczema, psoriasis, and impetigo.
The scaling rash of cutaneous diphtheria, as seen on the neck in this image, may be indistinguishable from more common
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


In a few cases, cutaneous diphtheria may undergo central ulceration; occasionally, a grayish membrane forms.
In a few cases, cutaneous diphtheria may undergo central ulceration; occasionally, a grayish membrane forms.
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Toxigenic strains of Corynebacterium diphtheriae may cause a thick pharyngeal exudate. The exudate is dirty gray and is tough, fibrinous, and adherent to the mucosae.
Toxigenic strains of Corynebacterium diphtheriae may cause a thick pharyngeal exudate. The exudate is dirty gray and is
Image courtesy of the Centers for Disease Control and Prevention.
In acute nasopharyngeal diphtheria, local edema may cause a visibly swollen neck (bull neck).
In acute nasopharyngeal diphtheria, local edema may cause a visibly swollen neck (bull neck).
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
The scaling rash of cutaneous diphtheria, as seen on the neck in this image, may be indistinguishable from more common skin conditions, such as eczema, psoriasis, and impetigo.
The scaling rash of cutaneous diphtheria, as seen on the neck in this image, may be indistinguishable from more common
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
In a few cases, cutaneous diphtheria may undergo central ulceration; occasionally, a grayish membrane forms.
In a few cases, cutaneous diphtheria may undergo central ulceration; occasionally, a grayish membrane forms.
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Skin infection
Skin lesions usually occur on the extremities and are varied in appearance, often indistinguishable from chronic skin conditions (eg, eczema, psoriasis, impetigo). A few patients have nonhealing, punched-out ulcers, occasionally with an overlying grayish pseudomembrane. Pain, tenderness, erythema, and exudate are typical. If exotoxin is produced, lesions may be numb. Concomitant nasopharyngeal infection occurs in approximately 20% of patients by direct or indirect inoculation with the organism, often from preexisting chronic skin lesions (2).
Complications
The main complications of diphtheria are cardiac and neurologic. Bacteremia due to nontoxigenic strains of C. diphtheriae may result in endocarditis, septic arthritis, and mycotic cerebral aneurysms.
Myocarditis is usually evident by the 10th to 14th day but can appear any time during the first to the sixth week, even while local respiratory symptoms are subsiding; risk of cardiac toxicity is related to degree of local infection. Insignificant ECG changes (eg,ST-segment and T-wave changes, and QT interval prolongation) occur in 20 to 30% of patients, but atrioventricular dissociation, complete heart block, and ventricular arrhythmias may occur and are associated with a high mortality rate. Heart failure may develop.
Nervous system toxicity is uncommon (approximately 5%) and limited to patients with severe respiratory diphtheria. The toxin causes a demyelinating polyneuropathy that affects cranial and peripheral nerves. The toxic effects usually begin during the first week of illness with loss of ocular accommodation and bulbar palsy, causing dysphagia and nasal regurgitation. Peripheral neuropathy appears during the third to sixth week. It is both motor and sensory, although motor symptoms predominate. The diaphragm may become paralyzed, sometimes causing respiratory failure. Resolution occurs over many weeks. Autonomic dysfunction in the form of loss of vasomotor tone (tachycardia, arrhythmias, and arterial hypotension) is also a complication of diphtheria.
In severe cases, acute kidney failure may occur because the toxin damages the kidneys.
Overall estimated case-fatality ratio is 5 to 10% (1). Mortality is higher in patients with any of the following (3, 4):
Delayed presentation
Unvaccinated or partially vaccinated patients
Acute kidney failure
Myocarditis
Symptoms and signs references
1. Acosta AM, Moro PL, Hariri S, Tiwari TSP: Chapter 7: Diphtheria. In Centers for Disease Control and Prevention: Epidemiology and Prevention of Vaccine-Preventable Diseases (the "pink book").April 23, 2024. Accessed July 15, 2025.
2. Koopman JS, Campbell J. The role of cutaneous diphtheria infections in a diphtheria epidemic. J Infect Dis. 1975;131(3):239-244. doi:10.1093/infdis/131.3.239
3. Gampa M, Karna PN, Reddy KV, et al. Study of Diphtheria and Its Complications: A Retrospective Study from a Tertiary Care Hospital. Pediatr Inf Dis 2021;3(4):140–142. doi: 10.5005/jp-journals-10081-1307
4. Kadirova R, Kartoglu HU, Strebel PM. Clinical characteristics and management of 676 hospitalized diphtheria cases, Kyrgyz Republic, 1995. J Infect Dis. 2000;181 Suppl 1:S110-S115. doi:10.1086/315549
Diagnosis of Diphtheria
Gram stain and culture
Tests for toxin production
Pharyngeal diphtheria needs to be considered in patients with nonspecific findings of pharyngitis, cervical adenopathy, and low-grade fever if they also have systemic toxicity plus hoarseness, palatal paralysis, or stridor. The appearance of the characteristic pseudomembrane suggests the diagnosis.

Gram stain of a specimen from the pseudomembrane may reveal gram-positive bacilli with metachromatic (beaded) staining in typical Chinese-character configuration, with club-shaped swelling at one or both ends. Material for culture should be obtained from below the pseudomembrane, or a portion of the pseudomembrane itself should be submitted. The laboratory should be notified that C. diphtheriae is suspected, so that special selective tellurite-containing culture media (Loeffler or Tinsdale) can be used.


This photomicrograph shows numerous gram-positive, club-shaped, C. diphtheriae bacteria, which cause the disease diphtheria.
CDC/ Graham Heid
Cutaneous diphtheria should be considered when a patient develops skin lesions during an outbreak of respiratory diphtheria. Skin swab or biopsy specimens should be cultured. Cutaneous diphtheria lesions may be coinfected with group A streptococci or Staphylococcus aureus.
ECG should be performed to look for ST-T wave changes, QTc prolongation, and/or first-degree heart block related to myocarditis, which often becomes evident as the respiratory symptoms resolve.
In vitro testing for toxin production (modified Elek immunodiffusion test) is performed to differentiate toxigenic from nontoxigenic strains. Polymerase chain reaction testing for the diphtheria toxin gene can also be done. An enzyme immunoassay (EIA) test using a monoclonal antibody against a component of the exotoxin is also available.
Treatment of Diphtheria
Diphtheria antitoxin
Penicillin, erythromycin, or azithromycin
In asymptomatic patients, daily monitoring for the development of signs and symptoms of diphtheria for 7 days after the last exposure should also be implemented.
Symptomatic patients with respiratory diphtheria should be hospitalized in an intensive care unit to monitor for respiratory and cardiac complications. Isolation with respiratory-droplet and contact precautions is required and must continue until 2 sequential cultures, taken starting 24 and 48 hours after antibiotics are stopped (after at least 14 days of treatment), are negative (1).
Diphtheria antitoxin
Diphtheria antitoxin must be administered empirically in all cases of diphtheria without waiting for culture confirmation because the antitoxin neutralizes only circulating toxin not yet bound to or within cells (2). Early administration of antitoxin mitigates the effects of the toxin and improves outcomes, because the severity of diphtheria-related complications is inversely proportional to the duration of illness before antitoxin administration (3). Although toxic sequelae are rarely reported in cutaneous diphtheria, the administration of diphtheria antitoxin is still advised by some experts to neutralize circulating toxin and prevent potential systemic complications (eg, myocarditis, neuropathy).
In the United States, antitoxin must be obtained through an expanded access investigational new drug (EA-IND) from the Centers for Disease Control and Prevention (CDC) (4).
CAUTION: Diphtheria antitoxin is of equine origin (ie, derived from horses); therefore, a skin (or conjunctival) test to rule out sensitivity should always precede administration.
The dose of antitoxin, ranging from 20,000 to 100,000 units IM or IV, is determined by the following:
Site and severity of symptoms
Duration of the disease
Complications
Allergic reactions include anaphylaxis occurring within 30 minutes of administration and delayed allergic reactions (serum sickness, a type III hypersensitivity reaction). If anaphylaxis occurs, 0.3 to 1 mL epinephrine 1:1000 (0.01 mL/kg) should immediately be injected subcutaneously, IM, or slowly IV. IV administration of antitoxin is contraindicated in patients who are allergic to the antitoxin.
Antibiotics
Antibiotics are required to eradicate the organism and prevent spread; they are not substitutes for antitoxin.
Patients may be given any of the following:
Erythromycin 500 mg in adults or (10 mg/kg orally or by injection for children) every 6 hours (maximum, 2 g a day) for 14 days
Procaine penicillin G IM (300,000 units every 12 hours for those weighing ≤ 10 kg and 600,000 units every 12 hours for those weighing > 10 kg) for 14 days
Azithromycin 10 to 12 mg/kg once daily (maximum 500 mg daily) or in adults 500 mg daily, IV or oral, for 14 days
When patients are able to tolerate oral antibiotics, they should be switched to penicillin 250 mg orally 4 times a day or erythromycin 500 mg (10 mg/kg for children) orally every 6 hours for a total of 14 days of treatment. Azithromycin is the preferred agent in some guidelines (5).
Vancomycin or linezolid can be used if antibiotic resistance is detected. Organism elimination should be documented by 2 consecutive negative throat and/or nasopharyngeal cultures performed at least 24 hours apart and no earlier than 14 days after the completion of antibiotic therapy.
Other treatments
For cutaneous diphtheria, thorough cleansing of the lesion with soap and water and administration of systemic antibiotics for 10 to 14 days, depending on the severity of the infection are recommended.
Recovery from severe diphtheria is slow, and patients must be advised against resuming activities too soon. Even normal physical exertion may harm patients recovering from myocarditis.
Vaccination is required after recovery for patients who had diphtheria because infection does not guarantee immunity.
Treatment references
1. Centers for Disease Control and Prevention: Diphtheria. Infection Control in Healthcare Personnel: Epidemiology and Control of Selected Infections Transmitted Among Healthcare Personnel and Patients (2024). April 12, 2024. Accessed July 15, 2025.
2. Truelove SA, Keegan LT, Moss WJ, et al. Clinical and Epidemiological Aspects of Diphtheria: A Systematic Review and Pooled Analysis. Clin Infect Dis. 2020;71(1):89-97. doi:10.1093/cid/ciz808
3. Adler NR, Mahony A, Friedman ND. Diphtheria: forgotten, but not gone. Intern Med J. 2013;43(2):206-210. doi:10.1111/imj.12049
4. Centers for Disease Control and Prevention. Diphtheria. Diphtheria Antitoxin. December 18, 2024. Accessed July 15, 2025.
5. Médecins Sans Frontières: Clinical Guidelines Diagnosis and Treatment Manual: Diphtheria. June 2025. Accessed July 15, 2025.
Prevention of Diphtheria
Prevention consists of:
Infection control measures (respiratory droplet isolation until the 14-day course of antibiotic treatment has concluded and 2 cultures at least 24 hours apart are negative)
Vaccination (primary and postexposure)
Antibiotics
Vaccination
See Diphtheria-Tetanus-Pertussis Vaccine (DTaP), Tetanus-Diphtheria-Pertussis (Tdap), and Tetanus-Diphtheria (Td booster) vaccines for more information.
The vaccine for diphtheria contains diphtheria toxoid; it is available only in combination with other vaccines.
Postexposure antibiotics
All close contacts should be examined; surveillance for evidence of disease is maintained for 7 days after the last known exposure. Contact tracing protocols may be obtained from the CDC Emergency Operations Center (1).
Nasopharyngeal and throat cultures for C. diphtheriae should be performed regardless of immunization status because the vaccine protects only against the effects of diphtheria toxin; it does not prevent infection with C. diphtheriae.
Close contacts, including household members and individuals in direct contact with the infected patient, should receive contact prophylaxis. Medical personnel exposed to a patient's respiratory secretions should also undergo prophylaxis.
Contact prophylaxis typically involves a single dose of penicillin G administered as follows:
600,000 units intramuscularly for patients younger than 6 years
1.2 million units intramuscularly for patients 6 years or older
Alternatively, oral erythromycin can be given at a dose of 500 mg 4 times a day for 7 to 10 days. Timely and complete antibiotic treatment is crucial for the individual patient, for preventing outbreaks, and for minimizing complications in the wider community.
If cultures remain positive, an additional 10-day course of erythromycin should be given; carriers should not be given antitoxin. After 3 days of treatment, carriers can safely resume work while continuing to take antibiotics. Cultures should be repeated; 24 hours after the completion of antimicrobial therapy, 2 consecutive culture sets of the nose and throat should be collected 24 hours apart. If results are positive, another course of antibiotics is given and cultures are performed again.
Prevention reference
1. Centers for Disease Control and Prevention: Office of Readiness and Response. Emergency Operations. February 21, 2024. Accessed July 15, 2025.
Key Points
Diphtheria is a contagious bacterial cutaneous or nasopharyngeal infection, producing a potent toxin that can damage the heart, nerves, and sometimes the kidneys.
Diphtheria is rare in countries with widespread vaccination but is endemic in many countries where vaccination is not widespread; rates are increasing slightly in some countries in which rates of vaccination and revaccination are declining.
Pharyngeal infection causes a characteristic pseudomembrane in the tonsillar area; it may initially appear as a white, glossy exudate but typically becomes dirty gray, tough, fibrinous, and adherent.
Treat with diphtheria antitoxin and penicillin or erythromycin; document cure by cultures after completion of treatment.
Vaccinate patients after recovery, and vaccinate close contacts who have not completed a primary series or who have gone > 5 years since their last booster.
Do nasopharyngeal and throat cultures of close contacts regardless of their immunization status.
Give antibiotics to close contacts; duration of treatment depends on culture results.
Drug Information for the Topic





