



Diabetic nephropathy is glomerular sclerosis and fibrosis caused by the metabolic and hemodynamic changes of diabetes mellitus. It manifests as slowly progressive albuminuria with worsening hypertension and chronic kidney disease. Diagnosis is based on history, physical examination, urinalysis, and urine albumin/creatinine ratio. Treatment is strict glucose control, angiotensin inhibition (using angiotensin-converting enzyme [ACE] inhibitors or angiotensin II receptor blockers [ARBs]), and control of blood pressure and lipids.
(See also Complications of Diabetes Mellitus: Diabetic nephropathy.)
Diabetic nephropathy is the most common cause of nephrotic syndrome in adults. Diabetic nephropathy is also the most common cause of kidney failure worldwide, accounting for up to half of new cases in the United States. The lifetime prevalence of kidney failure is approximately 40% among patients with diabetes mellitus (1, 2). Kidney failure associated with diabetes is particularly common in certain ethnic groups; in the United States kidney failure is common among Black, Hispanic, and Native American people (3). Other risk factors include the following:
Duration and degree of hyperglycemia
Certain polymorphisms affecting the renin-angiotensin-aldosterone axis
Family history of diabetic nephropathy
Genetic variables (decreased number of glomeruli)
Because type 2 diabetes is often present for several years before being recognized, nephropathy may be present at the time of diagnosis; 25% of patients with type 2 will have microalbuminuria 10 years after diagnosis (4). Kidney failure may take 10-20 years after to develop; for example, one study reports a mean duration from diagnosis of type 2 diabetes to kidney failure of 14 years (5).
General references
1. de Boer IH, Khunti K, Sadusky T, et al. Diabetes management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2022;102(5):974-989. doi:10.1016/j.kint.2022.08.012
2. Burrows NR, Koyama A, Pavkov ME. Reported Cases of End-Stage Kidney Disease - United States, 2000-2019. MMWR Morb Mortal Wkly Rep 2022;71(11):412-415. Published 2022 Mar 18. doi:10.15585/mmwr.mm7111a3
3. United States Renal Data System. 2024 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2024.
4. Adler AI, Stevens RJ, Manley SE, et al. Development and progression of nephropathy in type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int 2003;63(1):225-232. doi:10.1046/j.1523-1755.2003.00712.x
5. Ng YP, Ahmed R, Ooi GS, Lau CY, Balasubramanian GP, Yap CH. The rate of progression of type 2 diabetes mellitus to end stage renal disease - A single centred retrospective study from Malaysia. Diabetes Metab Syndr 2018;12(6):1025-1030. doi:10.1016/j.dsx.2018.06.018
Pathophysiology of Diabetic Nephropathy
Pathogenesis begins with small vessel disease. Pathophysiology is complex, involving glycosylation of proteins, hormonally influenced cytokine release (eg, transforming growth factor-beta), deposition of mesangial matrix, and alteration of glomerular hemodynamics. Hyperfiltration, an early functional abnormality, is only a relative predictor for the development of kidney failure.
Hyperglycemia causes glycosylation of glomerular proteins, which may be responsible for mesangial cell proliferation and matrix expansion and vascular endothelial damage. The glomerular basement membrane classically becomes thickened.
Lesions of diffuse or nodular intercapillary glomerulosclerosis are distinctive; areas of nodular glomerulosclerosis may be referred to as Kimmelstiel-Wilson lesions. There is marked hyalinosis of afferent and efferent arterioles as well as arteriosclerosis; interstitial fibrosis and tubular atrophy may be present. Mesangial matrix expansion appears to correlate with progression to kidney failure (1).

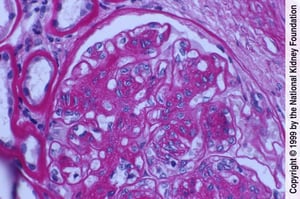
Mesangial cell proliferation and matrix expansion with endothelial damage are manifest here as thickened glomerular basement membranes without evident immune complex deposits (periodic acid-Schiff stain, ×400).
Mesangial cell proliferation and matrix expansion with endothelial damage are manifest here as thickened glomerular bas
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
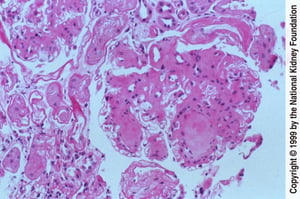
Formation of acellular nodules within mesangial matrix is a distinctive feature of diabetic nephropathy (periodic acid-Schiff stain, ×200).
Formation of acellular nodules within mesangial matrix is a distinctive feature of diabetic nephropathy (periodic acid-
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
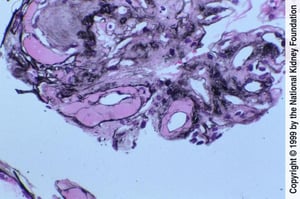
Hyalinosis of both afferent and efferent arterioles.
Hyalinosis of both afferent and efferent arterioles.
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Mesangial cell proliferation and matrix expansion with endothelial damage are manifest here as thickened glomerular basement membranes without evident immune complex deposits (periodic acid-Schiff stain, ×400).
Mesangial cell proliferation and matrix expansion with endothelial damage are manifest here as thickened glomerular bas
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Formation of acellular nodules within mesangial matrix is a distinctive feature of diabetic nephropathy (periodic acid-Schiff stain, ×200).
Formation of acellular nodules within mesangial matrix is a distinctive feature of diabetic nephropathy (periodic acid-
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Hyalinosis of both afferent and efferent arterioles.
Hyalinosis of both afferent and efferent arterioles.
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Diabetic nephropathy begins as glomerular hyperfiltration (increased glomerular filtration rate [GFR]); GFR normalizes with early kidney injury and mild hypertension, which worsens over time. Microalbuminuria, urinary excretion of albumin in a range of 30 to 300 mg (0.03 to 0.3 g) albumin/day, then occurs. Urinary albumin in these concentrations is called microalbuminuria because detection of proteinuria by dipstick on routine urinalysis usually requires >300 mg (0.3 g)albumin/day. Microalbuminuria progresses to macroalbuminuria (proteinuria > 300 mg/day [0.3 g/day] at a variable course), usually over years. Nephrotic syndrome (proteinuria ≥ 3 g/day) precedes kidney failure by several years but this timing is highly variable.
Other urinary tract abnormalities commonly occurring with diabetic nephropathy that may accelerate the decline of kidney function include papillary necrosis, type IV renal tubular acidosis, and urinary tract infections. In diabetic nephropathy, the kidneys are usually of normal size or larger (> 10 to 12 cm in length).
Pathophysiology reference
1. Mottl AK, Gasim A, Schober FP, et al. Segmental Sclerosis and Extracapillary Hypercellularity Predict Diabetic ESRD. J Am Soc Nephrol 2018;29(2):694-703. doi:10.1681/ASN.2017020192
Symptoms and Signs of Diabetic Nephropathy
Diabetic nephropathy is asymptomatic in early stages. Sustained microalbuminuria is the earliest warning sign. Hypertension and some measure of dependent edema eventually develop in most untreated patients.
In later stages, patients may develop symptoms and signs of uremia (eg, nausea, vomiting, anorexia) earlier (ie, with higher glomerular filtration rate [GFR]) than do patients without diabetic nephropathy, possibly because the combination of end-organ damage due to diabetes (eg, neuropathy) and kidney failure worsens symptoms.
Diagnosis of Diabetic Nephropathy
Yearly screening of all patients with diabetes with random urine albumin/creatinine ratio
Urinalysis for signs of other renal disorders (eg, hematuria, red blood cell [RBC] casts)
The diagnosis is suspected in patients with diabetes who have proteinuria, particularly if they have diabetic retinopathy (indicating small vessel disease) or risk factors for diabetic nephropathy. Other renal disorders should be considered if there are any of the following:
Heavy proteinuria with only a brief history of diabetes
Absence of diabetic retinopathy
Rapid onset of heavy proteinuria
Gross hematuria
RBC casts
Rapid decline in glomerular filtration rate (GFR)
Small kidney size
Urinary protein
Patients are tested for proteinuria by routine urinalysis; if proteinuria is present, testing for microalbuminuria is unnecessary because the patient already has macroalbuminuria suggestive of diabetic kidney disease. In patients without proteinuria on urinalysis, an albumin/creatinine ratio should be calculated from a mid-morning urine specimen. A ratio ≥ 30 mg/g (≥ 34 mg/mmol) indicates microalbuminuria if it is present on at least 2 of 3 specimens within 3 to 6 months and if it cannot be explained by infection or exercise.
Microalbuminuria be measured from a 24-hour urine collection, but this approach is less convenient, and many patients have difficulty accurately collecting a specimen. The random urine albumin/creatinine ratio can overestimate 24-hour collection of microalbuminuria in older and underweight individuals due to reduced creatinine production from reduced muscle mass (1). Inaccurate results can also occur in very muscular patients or if vigorous exercise precedes urine collection.
For most patients with diabetes who have proteinuria, the diagnosis is clinical. Renal biopsy can confirm the diagnosis but is rarely necessary.

Screening
Patients with type 1 diabetes without known kidney disease should be screened for proteinuria and, if proteinuria is absent on routine urinalysis, for microalbuminuria, beginning 5 years after diagnosis and at least annually thereafter (2).
Patients with type 2 diabetes should be screened at the time of diagnosis and annually thereafter (2).
Diagnosis references
1. Carter CE, Gansevoort RT, Scheven L, et al. Influence of urine creatinine on the relationship between the albumin-to-creatinine ratio and cardiovascular events. Clin J Am Soc Nephrol 2012;7(4):595-603. doi:10.2215/CJN.09300911
2. de Boer IH, Khunti K, Sadusky T, et al. Diabetes management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2022;102(5):974-989. doi:10.1016/j.kint.2022.08.012
Treatment of Diabetic Nephropathy
Maintenance of glycosylated Hb (HbA1C) ≤ 7.0
Aggressive blood pressure (BP) control, beginning with angiotensin inhibition
Treatment of dyslipidemia
Blood glucose control
Primary treatment is strict glucose control to maintain HbA1C ≤ 7.0; maintenance of euglycemia reduces microalbuminuria but may not retard disease progression once diabetic nephropathy is well-established.
Blood pressure control
Glucose control must also be accompanied by strict control of BP to < 130/80 mm Hg, although some experts recommend BP < 140/90 mm Hg. Some suggest BP should be 110 to 120/65 to 80 mm Hg, particularly in patients with protein excretion of > 1 g/day; however, others claim that BP values < 120/85 mm Hg are associated with increased cardiovascular mortality and heart failure.
Angiotensin inhibition is first-line therapy. Thus, angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs) are the antihypertensives of choice; they reduce BP and proteinuria and slow the progression of diabetic nephropathy. ACE inhibitors are usually tried first, in part because they are less expensive, but ARBs can be used instead if ACE inhibitors cause persistent cough. Treatment should be started when microalbuminuria is detected regardless of whether hypertension is present; some experts recommend medications be used even before signs of kidney disease appear.
Diuretics are required by most patients in addition to angiotensin inhibition to reach target BP levels. Dose should be decreased if symptoms of orthostatic hypotension develop or serum creatinine increases by more than 30%.
Nondihydropyridine calcium channel blockers (diltiazem and verapamil) are also antiproteinuric and renoprotective and can be used if proteinuria does not meaningfully decrease when target BP is reached or as alternatives for patients with hyperkalemia or other contraindications to ACE inhibitors or ARBs.
In contrast, dihydropyridine calcium channel blockers (eg, nifedipine, felodipine, amlodipine) do not reduce proteinuria, although they are useful adjuncts for BP control and may be cardioprotective in combination with ACE inhibitors. ACE inhibitors and nondihydropyridine calcium channel blockers have greater antiproteinuric and renoprotective effects when used together, and their antiproteinuric effect is enhanced by sodium restriction. Nondihydropyridine calcium channel blockers should be used with caution in patients taking beta-blockers because of the potential to worsen bradycardia.
Dyslipidemia
Dyslipidemia should also be treated.
Statins should be used as first-line therapy for dyslipidemia treatment in patients with diabetic nephropathy because they reduce cardiovascular mortality and urinary protein.
Other treatments
Dietary protein restriction yields mixed results. The American Diabetes Association and National Kidney Foundation recommend a target of 0.8 to 1.2 g protein/kg/day for patients with diabetes and overt nephropathy, but restriction below 0.8 g protein/kg/day is not recommended (1).
Sodium-glucose cotransporter-2 (SGLT 2) inhibitors should also be given to patients with type 2 diabetes, but not those with type 1 diabetes or those with an eGFR of < 20 mL/minute. Inhibition of the sodium glucose transporter has been shown to reduce the progression of kidney disease (2, 3, 4).
Vitamin D supplementation, typically with cholecalciferol (vitamin D3).
Sodium bicarbonate, given to maintain a serum bicarbonate concentration > 22 mEq/L (22 mmol/L), may slow disease progression in patients with chronic kidney disease and metabolic acidosis.
Treatments for edema can include the following:
Dietary sodium restriction (eg, < 2 g/day)
Fluid restriction
Loop diuretics, as needed, with careful titration to avoid hypovolemia
Kidney transplantation
Kidney transplantation with or without simultaneous or subsequent pancreas transplantation is an option for patients with kidney failure. The 5-year survival rate for patients with type 2 diabetes receiving a kidney transplant is almost 77%, compared with 88% for patients who do not have diabetes. Kidney allograft survival rates are > 97% among living donor transplant recipients and 77% among deceased donor transplant recipients at 5 years (5, 6).
Treatment references
1. de Boer IH, Khunti K, Sadusky T, et al. Diabetes management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2022;102(5):974-989. doi:10.1016/j.kint.2022.08.012
2. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al: Dapagliflozin in patients with chronic kidney disease. N Engl J Med 383(15):1436-1446, 2020. doi: 10.1056/NEJMoa202481
3. Perkovic V, Jardine MJ, Neal B, et al: Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 13;380(24):2295-2306, 2019. doi: 10.1056/NEJMoa1811744
4. Zinman B, Wanner C, Lachin JM, et al: Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 373(22):2117-2128, 2015. doi: 10.1056/NEJMoa1504720
5. United States Renal Data System. 2024 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2024.
6. Harding JL, Pavkov M, Wang Z, et al: Long-term mortality among kidney transplant recipients with and without diabetes: A nationwide cohort study in the USA. BMJ Open Diabetes Res Care 9(1):e001962, 2021. doi: 10.1136/bmjdrc-2020-001962
Prognosis for Diabetic Nephropathy
Prognosis is good for patients who are meticulously treated and monitored. Such care is often difficult in practice, however, and most patients slowly lose kidney function; even prehypertension (BP 120 to 139/80 to 89 mm Hg) or stage 1 hypertension (BP 140 to 159/90 to 99 mm Hg) may accelerate injury. Systemic atherosclerotic disease (stroke, myocardial infarction, peripheral artery disease) predicts an increase in mortality.
Key Points
Diabetic nephropathy is very common, asymptomatic until late, and should be screened for in all patients with diabetes.
Periodically screen all patients with diabetes with urinalysis and, if proteinuria is absent, albumin/creatinine ratio calculated from a mid-morning urine specimen.
Treat blood pressure aggressively, usually beginning with angiotensin inhibition.
Treat increased albuminuria with angiotensin inhibition.
Control glucose to maintain HbA1C at ≤ 7.0.
Treat dyslipidemia with a statin.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
American Diabetes Association Professional Practice Committee. Summary of Revisions: Standards of Care in Diabetes-2025. Diabetes Care 2025;48(1 Suppl 1):S6-S13. doi:10.2337/dc25-SREV
Drug Information for the Topic





