



Varices are dilated veins in the distal esophagus or proximal stomach caused by elevated pressure in the portal venous system, typically from cirrhosis. They may bleed massively but cause no other symptoms. Diagnosis is by upper endoscopy. Treatment is primarily with endoscopic banding and IV octreotide. Sometimes a transjugular intrahepatic portosystemic shunting procedure is needed.
Portal hypertension results from a number of conditions, predominantly liver cirrhosis. If portal pressure remains higher than inferior vena caval pressure for a significant period, venous collaterals develop. The most dangerous collaterals occur in the distal esophagus and gastric fundus, causing engorged, serpentine submucosal vessels known as varices. These varices partially decompress portal hypertension but can rupture, causing massive gastrointestinal (GI) bleeding. The trigger for variceal rupture is unknown, but bleeding almost never occurs unless the portosystemic pressure gradient is > 12 mm Hg (normal < 5 mmHg). Coagulopathies caused by liver disease may worsen bleeding.


Varices are dilated, submucosal esophageal veins caused by portal hypertension, most commonly in the setting of cirrhosis.
Pearls & Pitfalls
|
Symptoms and Signs of Varices
Patients typically present with sudden, painless, upper GI bleeding, often massive. Hematemesis may be present if the bleeding is severe. Signs of shock may be present. Bleeding is usually from the distal esophagus, less often from the gastric fundus. Bleeding from gastric varices also may be acute but is more often subacute or chronic.
Bleeding into the GI tract may precipitate portosystemic encephalopathy in patients with impaired hepatic function.
Diagnosis of Varices
Endoscopy
Evaluation for coagulopathy
Both esophageal and gastric varices are best diagnosed by endoscopy, which may also identify varices at high risk of bleeding (eg, those with red markings) (1). Endoscopy is also critical to exclude other causes of acute bleeding (eg, peptic ulcer), even in patients known to have varices; perhaps as many as one-third of patients with known cirrhosis who have upper GI bleeding have a nonvariceal source (2).
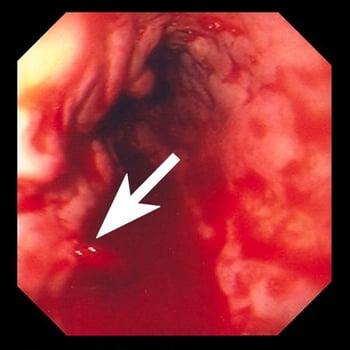
Hemorrhage from a ruptured varix (arrow).
Because varices are typically associated with significant hepatic disease, evaluation for possible coagulopathy is important. Laboratory tests include complete blood count (CBC) with platelets, prothrombin time (PT), partial thromboplastin time (PTT), and liver tests. Bleeding patients should have type and cross-match for multiple (typically ≥ 6) units of packed red blood cells.
Pearls & Pitfalls
|
Diagnosis references
1. Hwang JH, Shergill AK, Acosta RD, et al; American Society for Gastrointestinal Endoscopy. The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc. 2014 Aug;80(2):221-7. doi: 10.1016/j.gie.2013.07.023
2. Zullo A, Soncini M, Bucci C, Marmo R; Gruppo Italiano per lo Studio dell'Emorragia Digestiva (GISED) (Appendix). Clinical outcomes in cirrhotics with variceal or nonvariceal gastrointestinal bleeding: A prospective, multicenter cohort study. J Gastroenterol Hepatol. 2021 Nov;36(11):3219-3223. doi: 10.1111/jgh.15601
Treatment of Varices
Airway management and fluid resuscitation, including blood transfusion if needed
Endoscopic banding (sclerotherapy second choice)
IV octreotide
Sometimes antibiotics
Possibly a transjugular intrahepatic portosystemic shunting (TIPS) procedure
Airway management and fluid resuscitation, including transfusion if needed, are performed to manage hypovolemia and hemorrhagic shock. Patients with coagulation abnormalities (eg, significantly elevated international normalized ratio [INR]) can be treated with 1 to 2 units of fresh frozen plasma, but this should be given cautiously because giving large volumes of fluid to patients who are not hypovolemic may actually promote bleeding from varices and is associated with higher mortality (1).
Patients with known cirrhosis with GI bleeding are at risk of bacterial infection and should receive antibiotic prophylaxis with norfloxacin or ceftriaxone.
If a patient taking a nonselective beta-blocker (eg, propanolol) for primary prophylaxis for variceal bleeding has active hemorrhage and hypotension, the beta-blocker should be discontinued.
Because varices are diagnosed only during endoscopy, the primary treatment is endoscopic. Endoscopic banding of varices is preferred over injection sclerotherapy. At the same time, IV octreotide (a synthetic analog of somatostatin, which may also be used) should be given with an initial bolus followed by an infusion for 3 to 5 days after endoscopy (2). Octreotide increases splanchnic vascular resistance by inhibiting the release of splanchnic vasodilator hormones (eg, glucagon, vasoactive intestinal peptide). Octreotide is preferred over previously used agents such as vasopressin and terlipressin, because it has fewer adverse effects (3).
Tranexamic acid administration in some patients with cirrhosis may increase the success rate of endoscopic banding, and may decrease the rate of rebleeding (4).
If bleeding continues or recurs despite these measures, emergency techniques to shunt blood from the portal system to the vena cava can lower portal pressure and diminish bleeding. A TIPS procedure is the emergency intervention of choice (5). TIPS is an invasive radiologic procedure in which a guidewire is passed from the vena cava through the liver parenchyma into the portal circulation. The resultant passage is dilated by a balloon catheter, and a metallic stent is inserted, creating a bypass between the portal and hepatic venous circulations. Stent size is crucial. If the stent is too large, portal-systemic encephalopathy results because of diversion of too much portal blood flow from the liver. If the stent is too small, it is more likely to occlude.
Mechanical compression of bleeding varices with a Sengstaken-Blakemore tube or one of its variants causes considerable morbidity and should not be used as primary management. However, such a tube may provide life-saving tamponade pending decompression with a TIPS or surgical procedure. The tube is a flexible nasogastric tube with one gastric balloon and one esophageal balloon. After insertion, the gastric balloon is inflated with a fixed volume of air, and traction is applied to the tube to pull the balloon snugly against the gastroesophageal junction. This balloon is often sufficient to control bleeding, but, if not, the esophageal balloon is inflated to a pressure of 25 mm Hg. The procedure is quite uncomfortable and may result in esophageal perforation and aspiration; thus, endotracheal intubation and IV sedation are often recommended.
Expandable metal esophageal stents have been used successfully to tamponade bleeding.
Liver transplantation can also decompress the portal system but is a practical option only for patients already on a transplant list.
Long-term medical therapy of portal hypertension (with beta-blockers and nitrates) is discussed elsewhere. Treatment of portosystemic encephalopathy may be needed.
Splenectomy is performed to treat gastric variceal bleeding due to splenic vein thrombosis (sometimes a sequela of pancreatitis).

Treatment references
1. Mohanty A, Kapuria D, Canakis A, et al. Fresh frozen plasma transfusion in acute variceal haemorrhage: Results from a multicentre cohort study. Liver Int. 41(8):1901–1908, 2021. doi: 10.1111/liv.14936
2. Boregowda U, Umapathy C, Halim N, et al. Update on the management of gastrointestinal varices. World J Gastrointest Pharmacol Ther. 10(1):1–21, 2019. doi: 10.4292/wjgpt.v10.i1.1
3. Hwang JH, Shergill AK, Acosta RD, et al; American Society for Gastrointestinal Endoscopy. The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc. 2014 Aug;80(2):221-7. doi: 10.1016/j.gie.2013.07.023
4. Kumar M, Venishetty S, Jindal A, Bihari C, Maiwall R, Vijayaraghavan R, Saggere Muralikrishna S, Arora V, Kumar G, Sarin SK. Tranexamic acid in upper gastrointestinal bleed in patients with cirrhosis: A randomized controlled trial. Hepatology. 2024 Aug 1;80(2):376-388. doi: 10.1097/HEP.0000000000000817
5. Kaplan DE, Ripoll C, Thiele M, Fortune BE, Simonetto DA, Garcia-Tsao G, Bosch J. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology. 2024 May 1;79(5):1180-1211. doi: 10.1097/HEP.0000000000000647
Prognosis for Varices
In approximately 40% of patients, variceal bleeding stops spontaneously.
Mortality is 15 to 25% at 6 weeks; mortality at 5 years ranges from 20 to 80% depending on complications that reflect the severity of underlying liver disease (1). Bleeding is often fatal in patients with severe hepatocellular impairment (eg, advanced cirrhosis), whereas patients with good hepatic reserve usually recover.
Surviving patients are at high risk of further variceal bleeding. Ongoing endoscopy or pharmacotherapy (ie, endoscopic banding or nonselective beta-blockers) significantly lowers this risk, with reported rebleeding rates ranging from 5 to 60% depending on treatment strategy (2, 3). However, the overall effect on long-term mortality seems to be marginal, probably because of the underlying hepatic disease.
Prognosis references
1. Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017 Jan;65(1):310-335. doi: 10.1002/hep.28906. Epub 2016 Dec 1. Erratum in: Hepatology. 2017 Jul;66(1):304. doi: 10.1002/hep.29169
2. Kaplan DE, Ripoll C, Thiele M, Fortune BE, Simonetto DA, Garcia-Tsao G, Bosch J. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology. 2024 May 1;79(5):1180-1211. doi: 10.1097/HEP.0000000000000647
3. Branch-Elliman W, Perumalswami P, Factor SH, Sled SM, Flamm SL. Rates of recurrent variceal bleeding are low with modern esophageal banding strategies: a retrospective cohort study. Scand J Gastroenterol. 2015;50(9):1059-67. doi: 10.3109/00365521.2015.1027263
Key Points
Varices are the main but not the only cause of GI bleeding in patients with cirrhosis.
The severity of the underlying liver disease is a major determinant of mortality of a bleeding episode.
Endoscopy is performed for diagnosis and treatment; banding or sclerotherapy can be used.
Recurrence rate of variceal bleeding is 5 to 40% depending on treatment.
Drug Information for the Topic





