



Sore throat is pain in the posterior pharynx that occurs with or without swallowing. Pain can be severe; many patients refuse oral intake.
Etiology of Sore Throat
Sore throat results from infection; the most common cause is
Tonsillopharyngitis
Less commonly, gastroesophageal reflux disease (GERD) and postnasal drip from allergic rhinitis or chronic rhinosinusitis may lead to a sore throat. Anaerobic infections are also less common, however, may cause Lemierre syndrome, which is a cause of acute sore throat, particularly those that are recurrent. Even more rarely, an abscess or epiglottitis is involved; although uncommon, these disorders are of particular concern because they may compromise the airway.
Some Infectious Causes and Features of Sore Throat
Cause | Common Features* | Diagnostic Approach |
|---|---|---|
Viral tonsillopharyngitis | Usually rhinorrhea and/or cough Pharyngeal and tonsillar erythema, sometimes with exudate Sometimes one or two enlarged cervical lymph nodes Sometimes no fever and/or only mild or moderate throat pain | History and physical examination alone |
Strep throat | Often severe throat pain and fever Rarely rhinorrhea or cough Marked pharyngeal and tonsillar erythema with exudate Usually tender cervical lymphadenopathy | Throat swab rapid antigen detection test (RADT) Throat culture |
Often high fever and constant fatigue without other upper respiratory infection symptoms Usually in adolescents or young adults Marked pharyngeal and tonsillar erythema with exudate, tonsillar enlargement Bilateral cervical lymphadenopathy and sometimes splenomegaly | Serology; heterophile antibody test Sometimes measurement of Epstein-Barr–specific antibodies | |
Abscess (eg, parapharyngeal)† | Severe throat pain, trismus, odynophagia, and sometimes drooling Characteristic "hot potato" voice Pharyngeal and tonsillar erythema Peritonsillar swelling with uvular deviation | Needle aspiration and culture Sometimes CT with contrast or another imaging test |
Sudden severe throat pain and odynophagia Usually occurs in children age 2 to 6 Often drooling, tachypnea, stridor Sometimes tripod position (sitting upright and leaning forward with neck tilted back and jaw thrust forward) Absence of pharyngeal and tonsillar erythema, exudates, and swelling | Flexible fiberoptic laryngoscopy done in the operating room Sometimes lateral neck radiographs | |
* Features include symptoms and the results of the physical examination. Features mentioned are typical but not always present. † These causes are rare. | ||
CT = computed tomography. | ||
Tonsillopharyngitis
Tonsillopharyngitis is predominantly a viral infection; a lesser number of cases are caused by bacteria.
The respiratory viruses (rhinovirus, adenovirus, the influenza virus, coronavirus, respiratory syncytial virus) are the most common viral causes, but occasionally Epstein-Barr virus (the cause of mononucleosis), herpes simplex, cytomegalovirus, HIV (as a primary infection), or coronavirus SARS-CoV-2 (the cause of COVID-19) is involved.


Hyperemia and tonsillar exudate in a patient diagnosed with sore throat. Sore throat, fever, and tender cervical adenitis were also present in this patient.
BIOPHOTO ASSOCIATES/SCIENCE PHOTO LIBRARY
The main bacterial cause of sore throat is group A beta-hemolytic streptococci (GABHS), mainly Streptococcus pyogenes species, which, although estimates vary, causes perhaps 10 to 25% of all sore throats in adults and slightly more in children. GABHS is a concern because serious poststreptococcal sequelae (eg, rheumatic fever, glomerulonephritis, abscess, pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections [PANDAS]) may occur.
Obligate anaerobic infection due to Fusobacterium species is also a common cause of recurrent sore throats.
Uncommon bacterial causes include gonorrhea, diphtheria, mycoplasma, and chlamydial infection.
Abscess


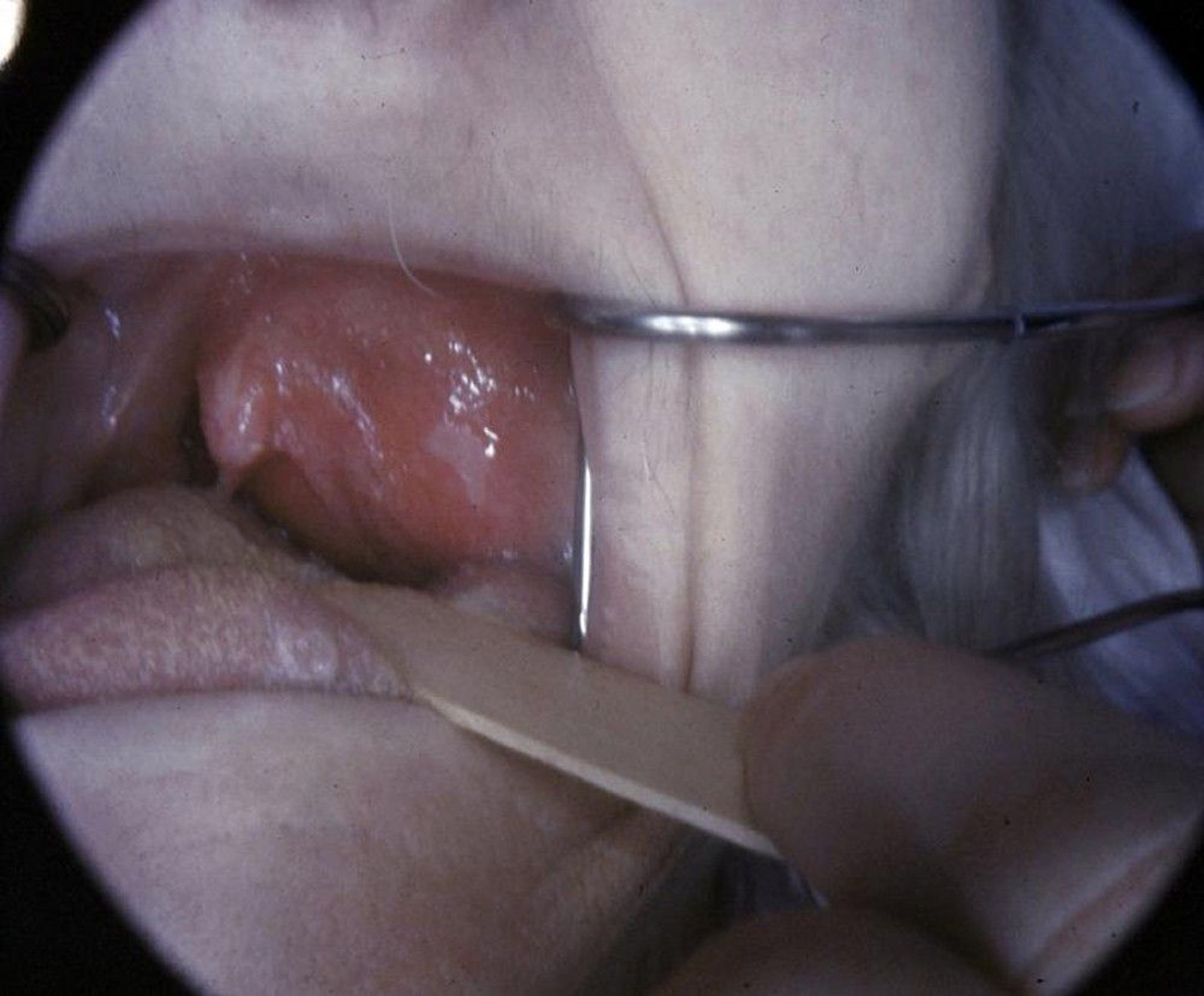
In this patient, the uvula is pushed away from the midline by the swollen tonsillar area, suggesting peritonsillar abscess or cellulitis. There are crypts on the swollen side.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY

This photo shows peritonsillar abscess with bulging and deviation of the uvula accompanying moderate trismus.
Image provided by Clarence T. Sasaki, MD.
An abscess in the pharyngeal area (peritonsillar, parapharyngeal, and, in children, retropharyngeal) is uncommon but causes significant throat pain. The usual causative organism is GABHS.
Epiglottitis
Epiglottitis, perhaps better termed supraglottitis, used to occur primarily in children and usually was caused by Haemophilus influenzae type B (HiB). Now, because of widespread childhood vaccination against HiB, supraglottitis/epiglottitis has almost been eradicated in children; more cases occur in adults. Causal organisms in children and adults include Streptococcus pneumoniae, Staphylococcus aureus, nontypeable H. influenzae, Haemophilus parainfluenzae, beta-hemolytic streptococci, Moraxella catarrhalis, and Klebsiella pneumoniae. HiB is still a cause in adults and unvaccinated children.
Evaluation of Sore Throat
History
History of present illness should note the duration and severity of sore throat.
Review of systems should seek important associated symptoms, such as fever, runny nose, cough, and difficulty swallowing, speaking, or breathing. The presence and duration of any preceding weakness and malaise (suggesting mononucleosis) are noted.
Past medical history should seek history of previous documented mononucleosis (recurrence is highly unlikely). Social history should include inquiring about close contact with people with documented GABHS infection, risk factors for gonorrhea transmission (eg, recent oral-genital sexual contact), and risk factors for HIV acquisition (eg, unprotected intercourse, multiple sexual partners, IV drug abuse).
Physical examination
General examination should note fever and signs of respiratory distress, such as tachypnea, dyspnea, stridor, and, in children, the tripod position (sitting upright, leaning forward with neck hyperextended and jaw thrust forward).
During direct pharyngeal examination, erythema, exudates, and any signs of swelling around the tonsils or retropharyngeal area should be noted. Whether the uvula is in the midline or appears pushed to one side should also be noted.
If supraglottitis or epiglottitis is suspected, especially in pediatric patients exhibiting stridor, it is crucial to perform a pharyngeal examination with caution, because the insertion of a tongue blade during the examination may provoke complete airway obstruction. Ideally, examination should be done in an operating room and with a flexible fiberoptic laryngoscope. Adults with no respiratory distress may be examined but also with care.
The neck is examined to check for enlarged, tender lymph nodes. The abdomen is palpated to check for splenomegaly, which may occur in patients with mononucleosis or HIV.
Red flags
The following findings in patients with a sore throat are of particular concern:
Stridor or other sign of respiratory distress
Drooling
Muffled, “hot potato” voice
Visible bulge in the pharynx
Interpretation of findings
Supraglottitis/epiglottitis and pharyngeal abscess pose a threat to the airway and must be differentiated from simple tonsillopharyngitis, which is uncomfortable but not acutely dangerous. Clinical findings help make this distinction.
With supraglottitis/epiglottitis, severe throat pain and dysphagia begin abruptly, usually with no preceding upper respiratory infection (URI) symptoms. Children often drool and exhibit signs of toxicity. Sometimes (more often in children), patients have respiratory manifestations, with tachypnea, dyspnea, stridor, and sitting in the tripod position. If examined, the pharynx almost always appears unremarkable.
Pharyngeal abscess and tonsillopharyngitis may cause pharyngeal erythema, exudate, or both. However, some findings are more likely to occur in one condition or the other:
Pharyngeal abscess: Muffled, “hot potato” voice (speaking as if a hot object is being held in the mouth) and visible focal swelling in the posterior pharyngeal area (often with deviation of the uvula)
Tonsillopharyngitis: Often URI symptoms (eg, runny nose, cough)
Although tonsillopharyngitis is easily recognized clinically, its cause is not. Manifestations of viral and GABHS infection overlap significantly, although URI symptoms are more common with a viral cause. In adults, the that increase suspicion of GABHS as a cause include
Tonsillar exudate
Tender lymphadenopathy
Fever or history of fever
Absence of cough
Adults with 1 or no criteria may reasonably be presumed to have viral illness. If ≥ 2 criteria are present, the likelihood of GABHS is high enough to warrant testing (1) but probably not high enough to warrant antibiotics, but this decision needs to be patient-specific (ie, threshold for testing and treatment may be lower in those at risk because of diabetes or immunocompromise). In children, testing is usually done and empirical treatment initiated to prevent serious poststreptococcal sequelae. Although this approach is reasonable, not all experts agree on when to test for GABHS and when antibiotic treatment is indicated.
Rarer causes of tonsillopharyngitis should be considered when the following are present:
Posterior cervical or generalized adenopathy, hepatosplenomegaly, and fatigue and malaise present for > 1 week: Infectious mononucleosis
No URI symptoms but possible recent oral-genital contact: Pharyngeal gonorrhea
A dirty-gray, thick, tough membrane on the posterior pharynx that bleeds if peeled away: Diphtheria (rare in the United States)
Risk factors for HIV infection: HIV infection
Testing
If supraglottitis/epiglottitis is considered possible after evaluation, specific testing is required. Patients who do not appear seriously ill and have no respiratory symptoms may have lateral neck radiographs to look for edematous epiglottis. However, these radiographs are subject to false-positive interpretation because patient positioning may be imperfect (not a perfectly lateral view) or it is taken during expiration. In addition, a child who appears seriously ill or has stridor or any other respiratory symptoms should not be transported to radiology. Such patients (and those with positive or equivocal radiographic findings) should usually have flexible fiberoptic laryngoscopy. (CAUTION: Examination of the pharynx and larynx may precipitate complete respiratory obstruction in children, and the pharynx and larynx should not be directly examined except in the operating room, where the most advanced airway intervention is available.)
Pearls & Pitfalls
|
Many abscesses are managed clinically, but if location and extent are unclear, immediate CT of the neck should be done.
In tonsillopharyngitis, throat culture is the most reliable way to differentiate viral infection from GABHS. To balance timeliness of diagnosis, cost, and accuracy, one strategy in children is to do a rapid strep screen (rapid antigen detection test) in the office and treat empirically if positive, and if negative, send a formal culture to a laboratory for testing. In adults, because other bacterial pathogens may be involved, throat culture for all bacterial pathogens is appropriate for those meeting clinical criteria described previously (tonsillar exudate, tender lymphadenomegaly, fever or history of fever, absence of cough).
Testing for mononucleosis, gonorrhea, or HIV infection is done only when clinically suspected.
Reference
1. Fine AM, Nizet V, Mandl KD: Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med 172 (11):847–852, 2012. doi:10.1001/archinternmed.2012.950
Treatment of Sore Throat
Specific conditions are treated. Patients with severe symptoms of tonsillopharyngitis may be started on a broad-spectrum antibiotic (eg, amoxicillin/clavulanate, dose based on age and indication) pending culture results.
Symptomatic treatments such as warm saltwater gargles and topical anesthetics (eg, benzocaine, lidocaine, dyclonine) may help temporarily relieve pain in tonsillopharyngitis, but patients should be instructed to avoid doses of topical anesthetics that result in toxicity. Patients in severe pain (even from tonsillopharyngitis) may require short-term use of opioids, preferably in liquid preparations.
Corticosteroids (eg, dexamethasone, 10 mg orally) are occasionally used to reduce inflammation and throat pain—for example, for tonsillopharyngitis that appears to pose a risk of airway obstruction (eg, due to mononucleosis) or very severe tonsillopharyngitis symptoms. Corticosteroids are effective in providing complete resolution of sore throat within 48 hours of initiation in the context of tonsillopharyngitis, particularly when used as an adjunct to antibiotics and analgesia, or even as a standalone treatment in certain cases (1).
Treatment reference
1. Sadeghirad B, Siemieniuk RAC, Brignardello-Petersen R, et al. Corticosteroids for treatment of sore throat: systematic review and meta-analysis of randomised trials. BMJ. 2017;358:j3887. Published 2017 Sep 20. doi:10.1136/bmj.j3887
Key Points
Most sore throats are caused by viral tonsillopharyngitis.
It is difficult to clinically distinguish viral from bacterial causes of tonsillopharyngitis.
Abscesses (parapharyngeal, retropharyngeal, peritonsillar) and epiglottitis are rare but serious causes.
Suspect epiglottitis if patients have a severe sore throat and a normal-appearing pharynx.
Drug Information for the Topic





