

Tuberculosis is an infection caused by the airborne bacteria Mycobacterium tuberculosis. It usually affects the lungs, but almost any organ can be affected.
Tuberculosis (TB) is spread mainly when people breathe air contaminated by a person who has an active TB infection.
Cough is the most common symptom, but people may also have a fever and night sweats, lose weight, feel generally unwell, and, if TB affects other organs, have various other symptoms.
The diagnosis usually involves a tuberculin skin test or a blood test, a chest x-ray, and examination and culture of a sputum sample (saliva and mucus coughed up from the lungs and throat).
People are typically treated with several antibiotics to reduce the risk of drug resistance.
Early diagnosis, treatment, and isolation of people with an active infection until they start to get better help prevent TB from spreading.
(See also Tuberculosis in Newborns.)

TB is caused by bacteria called Mycobacterium tuberculosis. Other related bacteria (called mycobacteria), such as Mycobacterium bovis, Mycobacterium microti, and Mycobacterium africanum, occasionally cause a similar disease. These 3 bacteria and Mycobacterium tuberculosis together are called the Mycobacterium tuberculosis complex.
Other species of mycobacteria, such as Mycobacterium avium, also cause diseases in people. They can cause skin infections, wound or foreign body infections, or leprosy. These other species do not cause TB.
TB usually affects the lungs, but it can affect almost any organ in the body and also the blood, bones, connective tissues, or skin.
Tuberculosis worldwide
TB has been a serious public health problem for a long time. In the 1800s, the disease caused about 25% of all deaths in Europe. Once antibiotics became available in the late 1940s, the battle against TB seemed to be won. However, because of factors such as inadequate public health resources, issues with access to health care, immune system weakness (which can be caused by advanced HIV infection [also called AIDS], other diseases, or medications that suppress the immune system), the development of drug resistance, and extreme poverty, TB continues to be a deadly disease in many parts of the world. In 2024, TB was fatal in an estimated 1.23 million people, most of them in low- and middle-income countries.
In 2024, there were 10.7 million new cases of TB worldwide. Most new cases occurred in Southeast Asia, Africa, the Western Pacific, and the Eastern Mediterranean. Few new cases occurred in the Americas and Europe.
New infections can occur in all types of people, widely ranging by region, age, race, sex, and socioeconomic status. In 2024, most infected people were men.
About one-fourth of all people in the world are thought to be infected. Most have a dormant TB infection (called latent TB infection), which does not cause symptoms and is not contagious. Only a small percentage of latent infections progress to active TB. At any one time, about 11 million people worldwide have active, contagious TB.
In areas of the world where both HIV infection and TB are common, people who have HIV infection have a greatly increased risk of dying of TB. In 2024, TB was fatal in about 150,000 people with HIV infection.
Did You Know...
|
Tuberculosis in the United States
In the United States in 2023, 9,633 new cases of TB were reported.
The risk of being infected is increased among people who live in high-risk facilities, such as shelters for people experiencing homelessness, long-term care facilities, or prisons. In 2023, people with diabetes mellitus or who currently or formerly smoked or vaped tobacco were also at increased risk of infection.
People from racial and ethnic minority groups are disproportionately affected in the United States. For example, in 2023, when compared with TB rates in White people, the number of cases was 7 times higher in Black people, about 4 times higher in Asian people, and about 5 times higher in Hispanic or Latino people. Men were infected more often than women.
In 2022, TB was the reported as the underlying cause of 565 deaths.
How Tuberculosis Develops
With most infectious diseases (such as strep throat or pneumonia), people become sick right after the microorganism enters their body and are noticeably ill within 1 or 2 weeks. TB does not follow this pattern.
TB occurs in 3 stages:
Primary infection
Latent infection
Active disease
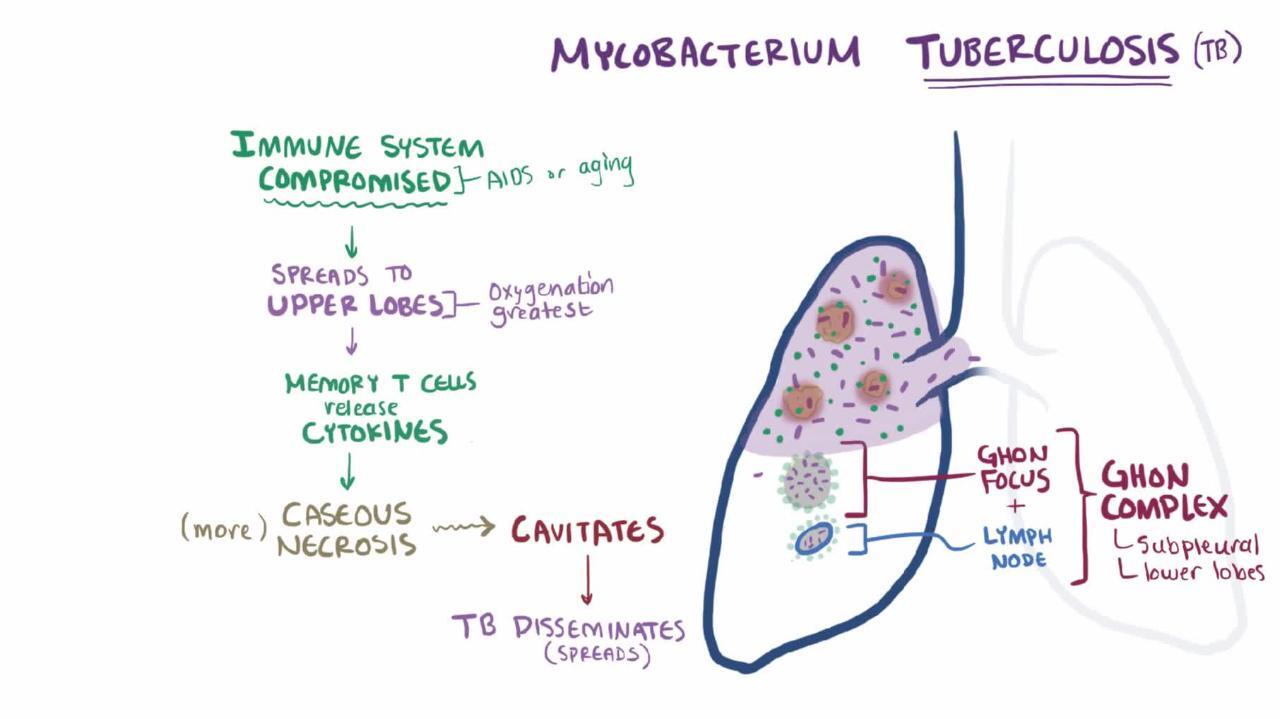
Except for very young children and people with a weakened immune system, few people become sick immediately after tuberculosis bacteria enter their body (this initial stage is called primary infection). In most cases, tuberculosis bacteria that enter the lungs are immediately killed by the body’s immune defenses. Bacteria that survive are engulfed by white blood cells called macrophages. The engulfed bacteria can remain alive inside these macrophages in a dormant state for many years (this stage is called latent infection). In most cases, these surviving bacteria never cause any further problems, but in a small percentage of infected people, they eventually start to multiply and cause active TB disease. At this stage, infected people actually become sick and are contagious.

Primary TB infection
In the first few weeks of the infection, some bacteria may travel from the lungs to nearby lymph nodes. These lymph nodes are located just outside the lungs. In most people, the infection goes no further, and the bacteria become dormant (inactive) and do not cause any symptoms.
However, infection in people with a weakened immune system (for example, children under age 5) may result in pneumonia and/or TB that affects other parts of the body (extrapulmonary TB). Also, in young children, the affected lymph nodes may become large enough to compress the bronchial tubes as they enter the lungs and cause symptoms (such as difficulty breathing and wheezing).
Usually, the infection is not contagious during primary infection.
Latent TB infection
During latent infection, bacteria can remain alive but in a dormant state inside macrophages for many years. The body walls off the bacteria inside a collection of cells, which form tiny scars in the lungs. The dormant bacteria do not multiply or cause symptoms. In most cases, these bacteria remain dormant and never cause any further problems.
The infection is not contagious during latent infection.
Active TB disease
In a small percentage of infected people, the dormant tuberculosis bacteria eventually start to multiply and cause active disease. This change from a dormant state is called reactivation. At this stage, infected people actually become sick and can spread the infection.
In many people who develop active disease, dormant bacteria reactivate within the first 2 years after the primary infection, but they may not reactivate for a very long time, even decades.
Reactivation occurs most often in the lungs and is more likely to occur in people who have a weakened immune system, especially people with HIV infection.
Other risk factors that make reactivation of TB infection more likely include the following:
Use of medications that suppress the immune system (such as steroids [sometimes called corticosteroids or glucocorticoids] and other medications such as adalimumab, etanercept, and infliximab)Use of medications that suppress the immune system (such as steroids [sometimes called corticosteroids or glucocorticoids] and other medications such as adalimumab, etanercept, and infliximab)
Age over 65
Substantial weight loss
Tobacco smoking
Blood cancers
Surgery to remove part or all of the stomach
TB is much more dangerous in people who have a weakened immune system. For such people, TB can be life threatening.
Transmission of infection
Mycobacterium tuberculosis can live only in people (not in animals). These bacteria are not normally transmitted by animals, insects, soil, or other nonliving objects. People are infected with TB usually by breathing air contaminated by a person who has active TB. Touching someone who has the disease does not spread it because Mycobacterium tuberculosis bacteria are spread almost exclusively through the air.
Did You Know...
|
People with active TB in their lungs or voice box (larynx) can contaminate the air with bacteria when they cough, sneeze, or even speak or sing. These bacteria can stay in the air for several hours. If another person breathes them in, that person may become infected. Thus, people who have close contact with a person who has active TB, such as family members or health care professionals who treat the infected person, are at increased risk of getting the infection. However, once people begin effective treatment, the risk of spreading the infection quickly decreases, usually after about 2 weeks.
People who have latent infection or TB that is not in their lungs or larynx do not expel bacteria into the air and cannot spread the infection.
Although Mycobacterium tuberculosis lives only in people, there are related mycobacteria that affect animals. Mycobacterium bovis is one of these related mycobacteria. It most commonly infects cattle and occasionally causes infection in people who consume unpasteurized milk or milk products (such as soft cheeses) from infected cows. In countries where cattle are tested for TB and milk is pasteurized, infection with Mycobacterium bovis is rare. However, cheese made from unpasteurized milk from infected cattle is sometimes brought into countries by travelers from other countries where infected cattle are a problem, and this sometimes results in infection in the people who eat it. If people inhale Mycobacterium bovis when it is present in the air, they can spread the bacteria to others when they cough or sneeze. People who work in slaughterhouses also may spread the infection if they breathe in bacteria from infected animal tissues.
Progression and spread of infection
The likelihood of TB progressing from latent infection to active disease varies greatly. Progression to active disease is far more likely and much faster in people with HIV infection and other risk factors. In contrast, people who have latent TB but who have a healthy immune system have about a 5 to 15% chance of developing active disease during their lifetime.
In people with a fully functioning immune system, active TB is usually limited to the lungs (pulmonary TB).
Extrapulmonary tuberculosis (TB outside the lungs) usually results from pulmonary TB that has spread from the lungs through the blood to affect other parts of the body. As in the lungs, the infection may not cause disease, but the bacteria may remain dormant in a very small scar. Dormant bacteria in these scars can reactivate later in life, leading to symptoms related to the organs involved.
Miliary tuberculosis develops if a large number of the bacteria travel through the bloodstream and spread throughout the body. This type of TB may be life threatening.
Symptoms and Complications of TB
Primary infection
Primary infection rarely causes symptoms, but when symptoms occur, they typically include fatigue and low-grade fever (around 100.4° F [38° C]). The thin, two-layered membrane that covers the lungs can become inflamed and causes chest pain.
Latent infection
People with latent infection do not have symptoms.
Active pulmonary tuberculosis
Some people with active pulmonary TB have no symptoms, except for not feeling well, fatigue, loss of appetite, and weight loss. These symptoms develop gradually over several weeks.
Cough is the most common symptom of active pulmonary TB. Because the disease develops slowly, infected people at first may blame the cough on smoking, a recent episode of flu, the common cold, or asthma. The cough may produce a small amount of green or yellow sputum, usually when people awaken in the morning. Rarely, the sputum may become streaked with blood.
People may awaken in the night and be drenched in sweat, with or without fever. Sometimes there is so much sweat that people have to change nightclothes or even the bed sheets.
People who develop shortness of breath and chest pain may have air (pneumothorax) or fluid (pleural effusion) in the space between their lungs and chest wall. Eventually, many people with untreated TB develop shortness of breath as the infection spreads in the lungs.
Extrapulmonary tuberculosis
TB can also affect the bones, brain, abdominal cavity, heart, skin, joints (especially weight-bearing joints, such as the hips and knees), liver, intestines, reproductive organs, blood, and lymph nodes. TB in these areas can be difficult to diagnose.
Symptoms of extrapulmonary TB are vague, usually fatigue, poor appetite, intermittent fevers, sweats, and possibly weight loss.
Sometimes the infection causes pain, discomfort, a collection of pus (abscess), or other symptoms, depending on the area involved:
Heart: In tuberculous pericarditis, the pericardium (the two-layered membrane around the heart) thickens and sometimes leaks fluid into the space between the pericardium and the heart. These effects limit the heart’s ability to pump and cause fever, chest pain, enlarged neck veins, and difficulty breathing. In parts of the world where TB is common, tuberculous pericarditis is a common cause of heart failure.
Lymph nodes: In a new TB infection, the bacteria may travel from the lungs to the lymph nodes that drain the lungs. If the body’s natural defenses can control the infection, it goes no further, and the bacteria become dormant. However, very young children have weaker defenses. In them, the lymph nodes that drain the lungs may become large enough to compress the bronchial tubes, causing a brassy cough and possibly a collapsed lung. Occasionally, bacteria spread from these lymph vessels to lymph nodes in the neck. An infection in lymph nodes in the neck may break through the skin and discharge pus. Sometimes bacteria travel in the bloodstream to lymph nodes in other parts of the body.
Brain: TB that infects the tissues covering the brain (tuberculous meningitis) is life threatening. In the United States, tuberculous meningitis most commonly occurs among older adults and people with a weakened immune system. In areas where TB is common among children, tuberculous meningitis usually occurs in newborns and children through 5 years of age. Symptoms include fever, constant headache, neck stiffness, nausea, confusion, and drowsiness that can lead to coma. TB may also infect the brain itself, forming a mass called a tuberculoma. A tuberculoma may cause symptoms such as headaches, seizures, or muscle weakness. Tuberculomas are also more common among and more destructive in people with advanced HIV infection.
Intestine: Intestinal TB occurs mainly in countries in which TB in cattle is a problem. It is acquired by eating or drinking unpasteurized dairy products contaminated with Mycobacterium bovis. This infection can cause pain, diarrhea, blockage of the intestine, and passage of bright red blood from the anus. Tissues in the abdomen may swell. This swelling may be mistaken for cancer or appendicitis.
Kidneys and bladder: Infection of the kidneys may cause fever, back or flank pain, and pus in the urine. Infection commonly spreads to the bladder, making people have to urinate more frequently and making urination painful.
Genitals: TB can also spread to the genitals. In men, genital TB causes the scrotum to enlarge. In women, it causes chronic pelvic pain and sterility and increases the risk of a pregnancy in an abnormal location (ectopic pregnancy).
Skin: TB may spread from another site, such as the lymph nodes or bones, to the skin (called cutaneous TB). It may cause painless, firm lumps to form. Eventually, these lumps enlarge and form open sores. Channels may form between the infected area within the body and the skin, and pus may drain through them.


When tuberculosis spreads to the skin, it may cause painless, firm lumps to form under the skin, as seen in this photo (top arrow). These lumps eventually enlarge and form open sores (bottom arrow). Also, channels may form from the infected area inside the body to the skin's surface.
© Springer Science+Business Media
Tuberculosis: A Disease of Many Organs
Site of Infection | Symptoms or Complications |
|---|---|
Abdominal cavity | Fatigue, swelling, slight tenderness, and appendicitis-like pain |
Bladder | Painful urination and blood in urine |
Bones (mainly in children) | Swelling and minimal pain |
Tissues covering the brain and spinal cord (meninges) | Fever, headache, nausea, drowsiness, confusion, a stiff neck, and, if untreated, coma |
Pericardium (the two-layered membrane around the heart) | Fever, chest pain, enlarged neck veins, shortness of breath |
Joints | Arthritis-like symptoms |
Kidneys | Kidney damage with fever, back pain, and white blood cells (pus) and blood in the urine |
Lymph nodes | Swollen lymph nodes, which may become inflamed and tender and drain pus |
Reproductive organs in men | Lump in the scrotum |
Reproductive organs in women | Chronic pelvic pain and sterility or a mislocated (ectopic) pregnancy |
Spine | Worsening or constant back pain, collapsed vertebrae, and leg paralysis |
Spotlight On Aging: Tuberculosis
If latent tuberculosis (TB) reactivates in older adults, it may cause few symptoms. Thus, doctors may not suspect it for weeks or months. In older adults, the presence of other disorders also makes it hard to diagnose reactivated TB. Older adults who live in a nursing home are at risk of being infected with TB. The pneumonia that results may not be recognized as TB. Thus, it may not be appropriately treated and may spread to other people. In the United States, miliary TB most often affects older adults. Miliary TB is a potentially life-threatening type of TB that occurs when a large number of the bacteria travel through the bloodstream and spread throughout the body. TB that infects the tissues covering the brain (called tuberculous meningitis) is also more common among older adults. This life-threatening infection causes fever, constant headache, neck stiffness, nausea, confusion, and drowsiness that can lead to coma. If older adults have long-standing latent TB, doctors weigh the risk and benefits of using antituberculosis antibiotics to prevent active TB from developing. The risk that these medications may cause harmful side effects may be greater than the risk of developing TB. In such cases, doctors often consult a TB expert before they decide whether to use antibiotics. |
Diagnosis of TB
Chest x-ray
Sputum sample tests: Nucleic acid amplification test (NAAT) and microscopic examination and culture of a sputum sample
Screening tests: Tuberculin skin test or blood tests for TB
Sometimes the first indication of TB is a positive screening test. Screening tests for TB are done routinely for people who are at risk of TB.
Doctors may suspect TB based on symptoms such as fever, a cough lasting more than 3 weeks, night sweats, weight loss, a cough the brings up blood, chest pain, and difficulty breathing.
When doctors suspect TB, the first tests done are:
Chest x-ray
NAATs to check for the genetic material (DNA) of Mycobacterium tuberculosis in sputum samples and to provide results quickly (usually with a few hours)
Microscopic examination and culture of a sputum sample
If the diagnosis is still unclear, the following may be done:
Tuberculin skin test
Interferon-gamma release assay (a blood test for TB)
If TB is diagnosed, blood tests to check for HIV infection (a risk factor for TB) and hepatitis B and hepatitis C may be done.
Chest x-ray for tuberculosis
In people with TB, a chest x-ray is typically abnormal. However, the abnormal findings in TB often resemble those in other disorders, so the diagnosis may depend on the results of the tuberculin skin test or other more specific tests for TB.
Sputum tests for tuberculosis
At least 3 sputum samples are collected. They are examined under a microscope to look for tuberculosis bacteria and are used to grow the bacteria in a culture. Microscopic examination provides results much faster than a culture but is less accurate. However, traditional cultures do not provide results for many weeks because tuberculosis bacteria grow slowly. For this reason, treatment of people who may have TB is often begun while doctors wait for results of sputum examination and culture. Newer culture methods that have much more rapid turnaround times (1 week or even less) are becoming increasingly more available and used worldwide.

NAATs are tests that increase the amount of the bacteria's genetic material and can confirm the presence of Mycobacterium tuberculosis in 24 to 48 hours. Newer NAATs can produce results in 2 hours. A sample of sputum is often used, but samples of other tissues such as a lymph node can be used if needed.
Genetic tests (also called drug-susceptibility tests) can also rapidly tell whether tuberculosis bacteria are resistant to some of the usual medications used to treat TB and thus can help doctors choose effective treatment. These tests detect mutations in the bacteria's genes that enable them to resist treatment with certain medications (see Next-generation sequencing technologies).
Skin test for tuberculosis
A tuberculin skin test (also called a Mantoux test) using purified protein derivative (PPD) is done by injecting a small amount of protein derived from tuberculosis bacteria between the layers of the skin, usually on the forearm. A pale bump appears immediately, then goes away in a few hours. This bump means only that the test was done correctly. About 2 or 3 days later, the injection site is checked. Swelling that feels firm to the touch and is larger than a certain size indicates a positive result. Redness around the site without swelling is not positive. A similar test called the Mycobacterium tuberculosis antigen-based skin test (TBST) may be done. This test is done the same way as the tuberculin skin test but is used to detect different proteins that are secreted by tuberculosis bacteria.
Some people who are very ill or who have a weakened immune system (such as those with HIV infection) may not respond to the skin test even if they are infected with TB.
Although a tuberculin skin test is one of the most useful tests for diagnosing TB, it indicates only that a person was infected by Mycobacterium tuberculosis or related bacteria or received a TB vaccine at some point. It does not indicate whether the infection is definitely TB or that the infection is currently active.
That is, results may indicate TB when it is not present (false-positive results) because people have a closely related infection (which is usually harmless) or have been recently vaccinated against TB.
Results may also indicate no TB when it is present (false-negative). But usually, results are false-negative only in people who:
Have a fever
Are very ill
Are older
Have a disorder that weakens the immune system, such as HIV infection
Are taking medications that suppresses the immune system, such as steroids (sometimes called corticosteroids or glucocorticoids)
Blood test for tuberculosis
The interferon-gamma release assay (IGRA) is a blood test that can detect TB. For this test, a sample of blood is mixed with synthetic proteins similar to those produced by the tuberculosis bacteria. If people are infected with tuberculosis bacteria, their white blood cells produce certain substances (interferons) in response to the synthetic proteins. The blood is then checked for the presence of interferons to determine whether TB infection is present.
This test, unlike tuberculin skin testing, does not cause a false-positive test result in people who have been vaccinated against TB.
Other tests
A sample of sputum is usually adequate, but occasionally a doctor needs to obtain a sample of lung fluid or tissue to make the diagnosis. An instrument called a bronchoscope is inserted through the mouth or nostril and into the airways. It is used to inspect the bronchial tubes and to obtain a sample of lung fluid or tissue. This procedure is most often done when other disorders, such as lung cancer, are suspected.
When symptoms suggest tuberculous meningitis, a doctor may need to do a spinal tap (lumbar puncture) to obtain a sample of spinal fluid for analysis. Because tuberculosis bacteria are hard to find in spinal fluid and because cultures usually take weeks, the polymerase chain reaction (PCR) technique may be used on the sample. It produces many copies of a gene, making identification of the bacteria’s DNA easier. Although test results are available quickly, doctors usually begin antibiotic therapy if they have any suspicion of tuberculous meningitis. Early treatment can prevent death and minimize brain damage.
Treatment of TB
Isolation
Antibiotics
Sometimes surgery or steroids
Most infected people do not need to be hospitalized for treatment. People are hospitalized if they:
Are seriously ill with TB
Have another serious disorder (such as cancer, malnutrition, or HIV infection)
Need to have diagnostic procedures
Do not have an appropriate place to go to (for example, if they are experiencing homelessness)
Have a substance use disorder
Need to be isolated, such as people who live in a group situation where they would regularly encounter previously unexposed people (such as a nursing home)
Isolation
People with pulmonary TB being treated in a hospital are kept in isolation in a room that is specially designed to minimize the risk of spreading infections through the air. The door is kept closed as much as possible, and the air in the room is changed 6 to 12 times every hour. People who are kept in isolation do not need to wear a surgical face mask if they can successfully cover their coughs. However, people who enter the room must wear a respirator (a specially fitted filter device, not a simple surgical mask).
People can move from isolation into a general hospital room or, sometimes, can return home when they have clearly responded to treatment. Typically, people have responded to treatment when all of the following occur:
Their sputum samples have been consistently negative (no tuberculosis bacteria seen) for a period of time (typically 3 negative samples over 2 days, including at least 1 negative early-morning sample).
They no longer have a fever.
They have regained their appetite and sense of well-being.
Antibiotics
A number of antibiotics are effective against TB. But because tuberculosis bacteria are very slow-growing, antibiotics must be taken for 4 to 6 months or longer. Treatment must be continued long after people feel completely well. Otherwise, TB tends to recur because it was not fully eliminated. Also, the tuberculosis bacteria may become resistant to the antibiotics.
Most people find it difficult to remember to take their medications every day for such a long time. Other people, for various reasons, stop treatment as soon as they feel better. Because of these problems, many experts recommend that people with tuberculosis receive their medications from a health care professional who watches them take the pills. This approach is called directly observed therapy (DOT). Because DOT ensures that people take every dose, the medications can sometimes be given just 2 or 3 times per week after the first 2 weeks. DOT is often done in person, but video DOT is an alternative method. With video DOT, people are observed taking their medications via a device that has video options, such as a smart phone, tablet, or computer.
Four antibiotics that work in different ways are always given because treatment with only one antibiotic can leave behind a few bacteria that are resistant to that antibiotic. With most other bacteria, a few bacteria would not be enough to cause a relapse, but if TB is treated with only one antibiotic, the tuberculosis bacteria soon become resistant to that antibiotic.
First-line medications are:
IsoniazidIsoniazid
RifampinRifampin
Pyrazinamide Pyrazinamide
EthambutolEthambutol
These 4 antibiotics are typically used together and are used first (called first-line medications). All of these antibiotics have side effects, but most people with TB are cured with these antibiotics and do not have any serious side effects.
There are many different combinations and dose schedules for these medications. Isoniazid, rifampin, and pyrazinamide may be contained in the same capsule, reducing the number of pills people have to take each day and reducing the chance of developing drug resistance. Unlike other antibiotics, those used to treat TB are usually taken at the same time, 1 time a day or 1 to 3 times a week.There are many different combinations and dose schedules for these medications. Isoniazid, rifampin, and pyrazinamide may be contained in the same capsule, reducing the number of pills people have to take each day and reducing the chance of developing drug resistance. Unlike other antibiotics, those used to treat TB are usually taken at the same time, 1 time a day or 1 to 3 times a week.
Second-line medications are usually used when the bacteria causing TB have become resistant to the first-line medications or when people cannot tolerate the first-line medications. Second-line medications include aminoglycosides (such as streptomycin, kanamycin, and amikacin), capreomycin (which is closely related to aminoglycosides), and (such as streptomycin, kanamycin, and amikacin), capreomycin (which is closely related to aminoglycosides), andfluoroquinolones (such as levofloxacin and moxifloxacin).(such as levofloxacin and moxifloxacin).
Other, newer medications are being developed to help treat TB that has become resistant to the usual medications. These medications include bedaquiline, delamanid, pretomanid, and sutezolid.Other, newer medications are being developed to help treat TB that has become resistant to the usual medications. These medications include bedaquiline, delamanid, pretomanid, and sutezolid.
Some Medications Used to Treat Tuberculosis
Medication | Route | Some Side Effects |
|---|---|---|
First-line medications* | ||
IsoniazidIsoniazid | By mouth | Liver injury (hepatitis) in 1 person in 1,000, resulting in fatigue, loss of appetite, nausea, vomiting, and jaundice Sometimes numbness in the limbs (peripheral neuropathy) |
Rifampin (and the related medications rifabutin and rifapentine)Rifampin (and the related medications rifabutin and rifapentine) | By mouth | Liver injury, particularly when rifampin is combined with isoniazid (but the side effects go away when people stop the medications) Reddish orange discoloration of urine, tears, and sweat Rarely a low white blood cell or platelet count |
PyrazinamidePyrazinamide | By mouth | Liver injury (hepatitis), digestive upset, and sometimes gout |
EthambutolEthambutol | By mouth | Sometimes blurred vision and decreased color perception (because the medication affects the optic nerve) |
MoxifloxacinMoxifloxacin | By mouth | Inflammation or rupture of tendons Nervousness, tremors, and seizures Antibiotic-associated diarrhea and colon inflammation (colitis) |
Second-line medications† | ||
Aminoglycosides, such as streptomycin, amikacin, and kanamycinAminoglycosides, such as streptomycin, amikacin, and kanamycin | By injection into a muscle or vein | Kidney injury, dizziness, hearing loss (due to damage to nerves of the inner ear), rash, and fever |
Fluoroquinolones, such as levofloxacinFluoroquinolones, such as levofloxacin | By mouth | Inflammation or rupture of tendons Nervousness, tremors, and seizures Antibiotic-associated diarrhea and colon inflammation (colitis) |
CapreomycinCapreomycin | By injection into a muscle or vein | Side effects similar to those of aminoglycosides (but capreomycin is often tolerated better if treatment is needed for a long time) |
* First-line medications are usually the first choice for treatment. | ||
† Second-line medications are usually used when the bacteria causing tuberculosis have become resistant to first-line medications or when people cannot tolerate the first-line medications. | ||
Did You Know...
|
Drug resistance
Tuberculosis bacteria can easily develop resistance to antibiotics, particularly when people do not take the antibiotics regularly or for as long as they are supposed to.
Bacteria that resist treatment with antibiotics are causing more and more cases of TB (called drug-resistant TB).
Drug resistance is a serious concern because drug-resistant TB must be treated for a very long time. People typically must take 4 or 5 medications for 18 to 24 months. Medications used to treat drug-resistant TB are often less effective, more toxic, and more expensive. A newer, shorter regimen of 4 medications is available, and the medications are taken for 6 months.
Tuberculosis bacteria that are resistant to antibiotics are classified based on the antibiotics they are resistant to:
Multidrug-resistant tuberculosis (MDR-TB): Resistant to both isoniazid and rifampin
Pre-extensively drug-resistant tuberculosis (pre-XDR-TB): Resistant to rifampin (may be resistant to isoniazid too), to more than 1 fluoroquinolone, and to either bedaquiline or linezolid or bothtoo), to more than 1 fluoroquinolone, and to either bedaquiline or linezolid or both
Extensively drug-resistant tuberculosis (XDR-TB): Resistant to isoniazid, rifampin, more than 1 fluoroquinolone, and bedaquiline or linezolid or both
The newer TB medications bedaquiline, delamanid, and pretomanid and the fluoroquinolone moxifloxacin are active against resistant strains of tuberculosis bacteria and may help control the epidemic of drug resistance.
Other treatments
Surgery to remove a portion of the lung is sometimes needed to treat people with the following:
Very drug-resistant infections
A cough that continuously brings up blood
Blocked airways
Pus that has accumulated (to drain it)
When tuberculous pericarditis causes significant restriction of the heart’s motion, the pericardium may need to be removed surgically. A tuberculoma (a mass that develops because of TB) in the brain or lung may also need to be surgically removed.
Doctors sometimes give steroids (such as dexamethasone) when TB causes a significant amount of inflammation, particularly in people with meningitis, pericarditis, or lung inflammation.Doctors sometimes give steroids (such as dexamethasone) when TB causes a significant amount of inflammation, particularly in people with meningitis, pericarditis, or lung inflammation.
Screening for and Treatment of Latent TB Infection
Certain tests are done routinely for people who are at risk of TB. The tests include the tuberculin skin test (TST) and the interferon-gamma release assay (IGRA) blood test.
People at risk of TB include those who:
Live or work with people who have active TB (screening is done yearly)
Are experiencing homelessness and reside in a shelter, or reside in a correctional facility
Were born in, currently live in, or have traveled for more than 1 month to areas where TB is common
Have signs of a past TB infection on a chest x-ray done for another reason
Have a weakened immune system (for example, because of HIV infection) or take a medication that may weaken the immune system and reactivate latent TB if present (for example, steroids and cancer chemotherapy)
Have certain disorders, such as diabetes, kidney disease, or head or neck cancer
Are over age 70
Have a substance use disorder
If the TST or IGRA results are positive, people are evaluated by a doctor, and a chest x-ray is taken. If the chest x-ray is normal and people have no symptoms suggesting TB, they probably have latent TB. People with latent TB are treated with antibiotics (see Treating TB early). If the chest x-ray is abnormal, people have symptoms of TB, or both, they are evaluated for active tuberculosis (see Diagnosis of Tuberculosis).
Prevention of TB
Prevention of TB has 3 aspects:
Stopping the spread of infection
Treating infection as early as possible before it becomes active disease
Sometimes vaccination
Stopping the spread of tuberculosis
Because tuberculosis bacteria are airborne, good ventilation with fresh air lowers the concentration of bacteria and limits their spread. Also, germicidal ultraviolet lamps can be used to kill airborne tuberculosis bacteria in buildings where people at risk are gathered, such as shelters for people experiencing homelessness, jails, and hospital and emergency department waiting areas. If health care workers handle samples of infected tissue or fluid or interact with people who may be infected, they wear specially fitted masks called respirators, which filter the air, to help protect them.
No precautions are needed if people do not have symptoms even if they do have a positive skin or blood test for TB.
Most people with active TB do not need to be hospitalized. However, to help prevent spread of the disease, they should do the following:
Stay at home
Avoid visitors (they do not have to avoid family members who have already been exposed)
Cover their cough with a tissue or cough into their elbow
People should follow these precautions until they are responding to the antibiotics. After 5 days of treatment with the correct antibiotics, people are less likely to spread the disease. However, if they live or work with people who are at high risk (such as young children or people with advanced HIV infection), repeated analyses of sputum samples may be needed to determine when the danger of spreading the infection has passed. Also, people who continue to cough during treatment, do not take their antibiotics as instructed, or have highly drug-resistant TB may need to follow these precautions longer so that they do not spread the disease.
Directly observed therapy (DOT) can also help prevent the spread of infection. Making sure that infected people take the prescribed antibiotics as instructed increases the chance that the bacteria will be eradicated.
Public health personnel try to determine who might have been infected by a person with TB and recommend that these people be tested for TB.
Treating tuberculosis early
Because TB is spread only by people with active disease, treatment of latent disease and early recognition and treatment of active disease are among the best ways to stop it from spreading.
Most people who have a positive tuberculin skin or blood test are treated even if they are not yet ill.
The antibiotic isoniazid is very effective at stopping the infection before it becomes active disease. It is given daily for 9 months. For some people, rifampin may be prescribed daily for 4 months. In some countries, isoniazid and rifapentine are taken together once a week for 3 months as directly observed therapy, primarily for latent TB.The antibiotic isoniazid is very effective at stopping the infection before it becomes active disease. It is given daily for 9 months. For some people, rifampin may be prescribed daily for 4 months. In some countries, isoniazid and rifapentine are taken together once a week for 3 months as directly observed therapy, primarily for latent TB.
Preventive therapy definitely benefits younger people who have a positive tuberculin skin test. It also is likely to help older adults with a positive tuberculin skin test if they are at high risk of TB—for example, if the any of the following apply:
Their skin or blood test changed from negative to positive within the past 2 years.
They have been recently exposed to tuberculosis bacteria.
They have a weakened immune system.
For older adults with long-standing latent infection, the risk of toxicity from the antibiotics may be greater than the risk of developing TB. In such cases, doctors often consult an expert in the subject before they decide whether to use preventive therapy.
If people have a positive skin or blood test, the risk of developing active infection is high:
If they have HIV infection
If they take steroids or other medications that suppress their immune system (including some anti-inflammatory medications such as infliximab, etanercept, and tofacitinib)If they take steroids or other medications that suppress their immune system (including some anti-inflammatory medications such as infliximab, etanercept, and tofacitinib)
Such people usually need treatment for latent TB infection.
Vaccination for tuberculosis
In areas of the world where TB is common, a vaccine called bacille Calmette-Guérin (BCG) is used to do the following:
Reduce development of serious complications, such as meningitis
Help prevent infection in people who are at high risk of becoming infected with Mycobacterium tuberculosis, especially children
Doctors usually do not recommend the BCG vaccine for people living in the United States. However, the vaccine may have a role in protecting health care workers and others (particularly children) exposed to TB that is resistant to 2 or more antibiotics.
People who received BCG vaccine at birth may have a positive reaction to the tuberculin skin test years later, even if they are not infected with tuberculosis bacteria. The effect of BCG vaccination on skin test results is usually smaller than that of TB, and it lessens with time. Nonetheless, people vaccinated at birth often incorrectly attribute a positive skin test later in life to the BCG vaccine. In most countries, TB is stigmatized, and many people are reluctant to believe they have latent infection, which is much less active disease. Usually, if children who have been vaccinated have a positive tuberculin skin test, doctors presume it is due to TB and treat it accordingly. Untreated latent infection can have serious complications, especially in children.
However, if possible, people who have received the BCG vaccine should be tested for TB using an interferon-gamma release assay (IGRA) because the IGRA does not cause a false-positive test result in people who have received the BCG vaccine. This test can also determine whether a positive reaction to a skin test is due to infection with Mycobacterium tuberculosis.





