

The vertical mattress suture accomplishes, in a single suture, both dermal and subdermal approximation using a wide-deep (“far-far”) loop, followed by epidermal approximation and eversion using a narrow-shallow (“near-near”) loop. The major advantage of this suture is its capacity for alignment and eversion of wound edges.
(See also figures Vertical Mattress Suture, Lacerations, and How To Insert Simple Interrupted Sutures.)
The mattress sutures (both vertical and horizontal) are commonly used to close wounds under tension. Suture loops placed through the skin lateral to the wound (rather than over the wound) transfer tension away from the wound edges to the looped lateral skin. Additionally, having the sutures cross under (rather than over) the laceration, can help achieve eversion of the edges when the suture is tightened.
Indications for Vertical Mattress Sutures
Wounds with edges that are difficult to align or evert. These can include wounds that tend to invert, such as those of concave skin of the groin or posterior neck or loose skin over the dorsum of the elbow or hand.
Wounds under moderate (but not marked) tension (instead of a layered closure)
Contraindications for Vertical Mattress Sutures
Absolute contraindications
Laceration of the face, palm, or sole, where a blind deep suture is contraindicated
Relative contraindications
Wounds under marked tension
Wounds that may be contaminated or relatively old and would be at higher risk of infection if closed by sutures, such as small bites to hands or feet, puncture wounds, or high-velocity missile wounds.
Wounds involving deep structures (eg, nerves, blood vessels, ducts, joints, tendons, bones) may require specialized techniques or consultation by a surgical specialist, as should those covering large areas or involving the face or hands.
Complications of Vertical Mattress Sutures
Infection
Scarring, due to unrelieved tension on the laceration
Cross-hatching (train tracks) due to pressure on the skin surface caused by the wide-deep loop
Cutting of skin by sutures, particularly by the narrow-shallow loop, particularly if this loop is placed prior to the wide-deep loop
Ischemia and necrosis, which occur more often than with simple interrupted or continuous sutures
Equipment for Vertical Mattress Sutures
Wound hygiene and closure are not required to be performed under sterile conditions (4, 5). Instruments that touch the wound (eg, forceps, needles, suture) must be sterile. Clean single-use nonsterile gloves as well as clean but not sterile water may be used in immunocompetent patients.
Clean procedure, barrier protection
Appropriate personal protective equipment (eg, face mask, safety glasses or a face shield, head cap, gown, gloves)
Sterile drapes, towels (for wound debridement and suturing)
Needle driver, toothed forceps, suture material (typically, a nonabsorbable monofilament suture is used; for detailed discussion of the various types and sizes of suture material, see Lacerations)
Antiseptic solution (eg, chlorhexidine, povidone-iodine), sterile gauze squaresAntiseptic solution (eg, chlorhexidine, povidone-iodine), sterile gauze squares
Sometimes splinting or other materials (for aftercare, to restrict motion or skin tension that may pull on the sutures)
Materials used to dress the wound
Positioning for Vertical Mattress Sutures
Position the patient comfortably reclined or supine.
Adjust the stretcher height so that you will be comfortable either sitting or standing at the bedside.
In general, position yourself so that the laceration is roughly parallel to the front of your body.
The laceration should be well lit, preferably with an overhead procedure light.
Step-by-Step Description of Vertical Mattress Sutures
(For step-by-step descriptions of wound preparation, anesthesia, and dressing, see How To Cleanse, Irrigate, Debride, and Dress Wounds; for instructions on how to handle the instruments, work with needles, and tie a surgeon's knot using instruments, see How To Repair a Laceration With Simple Interrupted Sutures.)
Cleanse, anesthetize, irrigate, and debride the wound as necessary.
Place a sterile fenestrated drape over the wound. Place additional drapes nearby as needed to provide a large-enough sterile work area.
In general, place the first suture in the middle of the wound. Place all subsequent sutures in the middle of each open section, until there are no gaps.
Vertical mattress suture
The first pass of the needle (wide-deep bite) is placed farther from the wound edges (eg, > 1 cm) and deeper than the bite of a simple interrupted suture.
Push the needle through both wound edges if this can be done with little resistance. If resistance is significant, or if you are placing a suture across a relatively wide space (as may occur with the first few sutures), pull the needle out through the center of the laceration after it passes through the first wound edge; then reattach it to the needle driver and continue the suture with a second bite, passing it into the opposite side of the wound.
Reverse the direction of the needle in the needle driver.
The second pass (narrow-shallow bite) is placed closer to the wound edge and begins on the same side of the laceration as the exit site of the first pass. Use forceps as needed to maintain edge eversion. In this pass, unlike with simple interrupted sutures, the width of the bite need not be greater at the deepest part of the wound than at the surface.
Tie the suture closed.
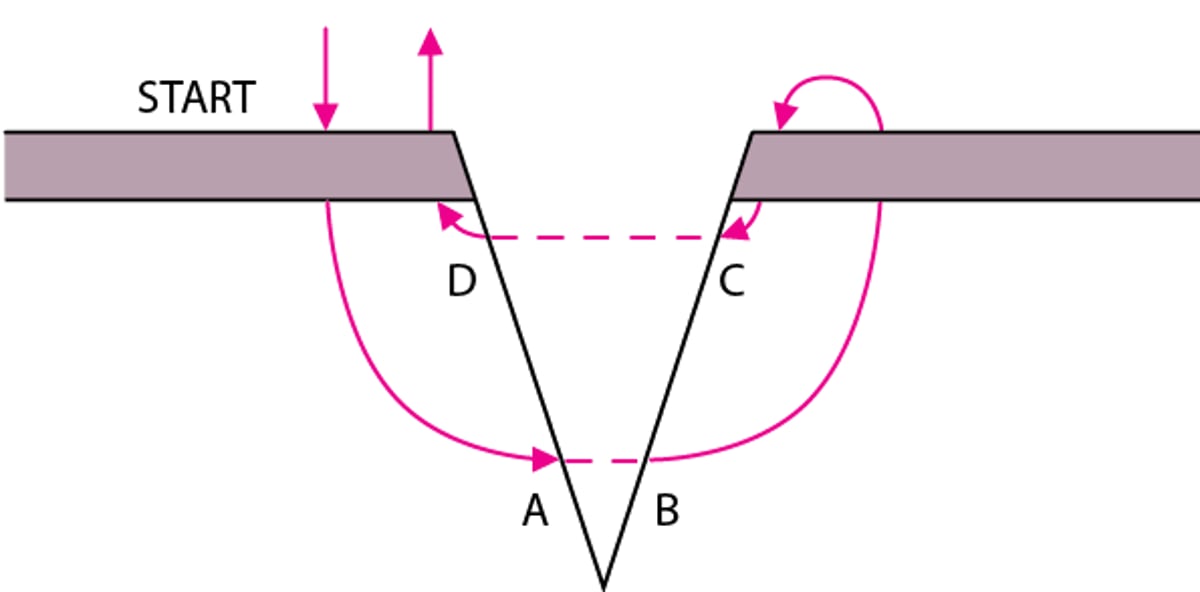
Vertical Mattress Suture
The first pass of the needle is the same as a large simple suture, but instead of tying off, another smaller bite is taken back across the wound to end on the starting side. Both ends are pulled up to closely align (approximate) the wound edges. Points A and B must be at the same depth, as must points C and D; this placement results in correct vertical alignment. |

Aftercare for Vertical Mattress Sutures
Dress the wound (see Lacerations and How To Cleanse, Irrigate, Debride, and Dress Wounds).
Splint joints if movement will cause wound tension (eg, an elbow splint for a dorsal elbow laceration).
Instruct the patient to keep the dressing dry and in place and to return in 2 days for a wound check.
Instruct the patient to return if signs of infection develop (eg, increased pain, swelling, erythema, fever, proximally spreading red streaks [infectious lymphangiitis]).
Instruct the patient when to return for suture removal, which is generally based on the wound site: 3 to 5 days for the face, 6 to 10 days for the scalp and trunk, 10 to 14 days for the arms and legs, and 14 days for wounds overlying joints. Early suture removal risks wound dehiscence; however, to decrease scarring and cross-hatching of facial sutures, half of the suture line (ie, every other suture) may be removed on day 3 and the remainder removed on day 5.
Warnings and Common Errors for Vertical Mattress Sutures
During pre-procedure preparation of the wound, diligently inspect the wound to avoid the frequent error of failing to note associated injuries of nearby tissues, foreign bodies, or body cavity penetrations
Avoid overly tight sutures and use cautery sparingly because both can cause tissue ischemia.
Tips and Tricks for Vertical Mattress Sutures
Some operators prefer to make the narrow-shallow loop first, which saves time by facilitating placement of the wide-deep loop. However, traditional placement of the wide-deep loop first facilitates a more precise placement of the narrow-shallow loop (achieving more even edge alignment) and also prevents tearing of the skin that may occur when pulling up on the narrow loop to start the wide bite.





