

Hypothyroidism is decreased production of thyroid hormone.
Hypothyroidism in children can occur when the thyroid gland is missing, is underdeveloped, or has developed in the wrong place or when another disorder causes the thyroid gland to become inflamed.
Symptoms depend on the child's age but include delayed growth and development.
The diagnosis is based on newborn screening tests, blood tests, and imaging tests.
Treatment includes giving thyroid hormone replacement.
(See also Hypothyroidism in adults.)

The thyroid gland is an endocrine gland located in the neck. Endocrine glands secrete hormones into the bloodstream. Hormones are chemical messengers that affect the activity of another part of the body.
Locating the Thyroid Gland

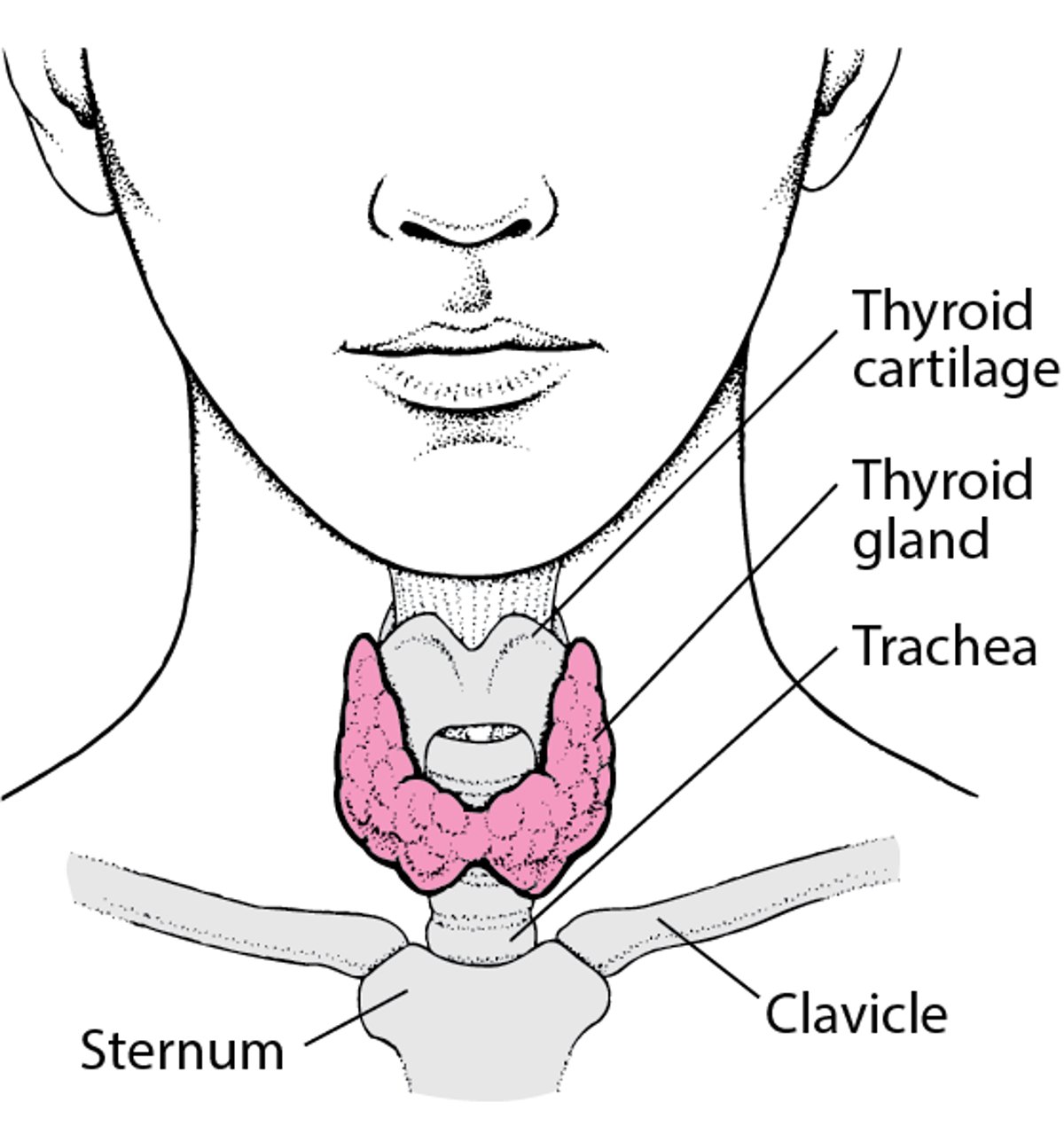
The thyroid gland secretes thyroid hormone. Thyroid hormone controls the speed of the body's metabolism, including how fast the heart beats and how the body regulates temperature. If the thyroid gland does not produce enough thyroid hormone, these functions slow down.
Hypothyroidism can occur in a developing fetus or newborn or during childhood or adolescence.
There are two types of hypothyroidism in children:
Congenital hypothyroidism: Present at birth
Acquired hypothyroidism: Develops after birth
Congenital hypothyroidism
Congenital hypothyroidism is present at birth.
Congenital hypothyroidism occurs when the thyroid gland does not develop or function normally before birth. This type of hypothyroidism occurs in about 1 in 2,000 to 4,000 live births. Most cases occur spontaneously, but about 10 to 20% are inherited.
More than half of cases of congenital hypothyroidism occur because the thyroid gland is missing, underdeveloped, or developed in the wrong place. Less often, the gland has developed normally but does not produce normal amounts of thyroid hormone.
In some countries, congenital hypothyroidism occurs when the mother does not get enough iodine in her diet while pregnant (iodine deficiency), and a woman's body needs more iodine when she is pregnant. Iodine deficiency is rare in areas of the world where iodine is added to table salt but is more common in areas where people do not get enough iodine in their diet.
Rarely, certain antibodies of the mother or medications that cause enlargement of the thyroid gland or medications that decrease the thyroid gland's production of thyroid hormones taken by the mother cross the placenta and temporarily cause congenital hypothyroidism.
In another rare cause, the pituitary gland is abnormally formed and fails to stimulate the thyroid gland to produce thyroid hormones. This is called central hypothyroidism. This pattern of thyroid abnormality also can develop in children who take certain medications (such as antiseizure medications and medications that help the body recognize and attack cancer cells) or who have certain illnesses. For those who have an illness, thyroid function becomes normal once the illness goes away.
Children who have Down syndrome are at increased risk of congenital hypothyroidism.
Acquired hypothyroidism
Acquired hypothyroidism occurs after birth.
In the United States, acquired hypothyroidism is most commonly caused by Hashimoto thyroiditis (autoimmune thyroiditis). In Hashimoto thyroiditis, the body's immune system attacks the cells of the thyroid gland, causing chronic inflammation and decreased production of thyroid hormones. About 50% of affected children have a family history of autoimmune thyroid disease. Hashimoto thyroiditis occurs most commonly during adolescence, but it can also occur in younger children, typically after the first few years of life. Children who have Down syndrome or Turner syndrome are at increased risk of Hashimoto thyroiditis. Children who have other genetic conditions (such as DiGeorge syndrome or Prader-Willi syndrome) are at increased risk of acquired hypothyroidism that is not autoimmune.
Worldwide, the most common cause of hypothyroidism is iodine deficiency, but this cause is rare in the United States. However, pregnant women in the United States can develop mild iodine deficiency because their bodies need more iodine when they are pregnant. Children whose diet is restricted because they have multiple food allergies or who are fed through a tube inserted into a vein (parenteral nutrition) may not eat enough of the proper foods and thus develop iodine deficiency.
Other less common causes of acquired hypothyroidism include radiation therapy to the head and neck for certain cancers and the use of certain medications (for example, lithium or amiodarone). Hypothyroidism also occurs as a result of Other less common causes of acquired hypothyroidism include radiation therapy to the head and neck for certain cancers and the use of certain medications (for example, lithium or amiodarone). Hypothyroidism also occurs as a result oftreatment for hyperthyroidism or for thyroid cancer.
Symptoms of Hypothyroidism in Infants and Children
Symptoms of hypothyroidism differ depending on the age of the child.
Newborns and infants
At first, newborns who have hypothyroidism that is caused by a problem with their thyroid gland usually have few if any symptoms because some thyroid hormone from the mother crosses the placenta. Once newborns no longer receive thyroid hormone from their mother, symptoms develop slowly and the disorder is detected only when they undergo newborn screening tests.
If the underlying cause of hypothyroidism is not identified and hypothyroidism remains undiagnosed or untreated, brain development slows moderately to severely. The newborn may become sluggish (lethargic) and have a poor appetite, yellowing of the skin (jaundice), low muscle tone, low heart rate, constipation, large fontanelles, hearing loss, a slightly open mouth with an enlarged tongue, a hoarse cry, and a bulging of the abdominal contents at the bellybutton (called an umbilical hernia). If the newborn has an enlarged thyroid gland (congenital goiter), the gland may press against the windpipe and interfere with breathing.
Eventually, infants may develop dry, cool, mottled skin, coarse facial features (such as a flat, broad nasal bridge and a puffy face), and a slightly open mouth with an enlarged tongue.
Rarely, delayed diagnosis and treatment of severe hypothyroidism lead to intellectual disability and short stature.
If iodine deficiency occurs very early during pregnancy, newborns may have severe growth failure, abnormal facial features, intellectual disability, and stiff muscles that are difficult to move and control (called spasticity).
Older children and adolescents
Some symptoms in older children and adolescents are similar to symptoms of hypothyroidism in adults (such as weight gain; fatigue; constipation; coarse, dry hair; and coarse, dry, and thick skin).
Symptoms that appear only in children include slowed growth, a delay in the development of the skeleton, and delayed puberty.
Diagnosis of Hypothyroidism in Infants and Children
Newborn screening test
Blood tests
Imaging tests
Because infants with hypothyroidism at birth often do not have any symptoms and because early treatment can prevent intellectual disability, doctors do routine screening tests of all newborns in the hospital after birth to evaluate thyroid function. If the screening is positive, tests to determine levels of thyroid hormones in the blood (thyroid function tests) are done to confirm the diagnosis of hypothyroidism. If confirmed, newborns must be treated quickly to prevent developmental delays.
Once congenital hypothyroidism is diagnosed, doctors may do imaging tests such as radionuclide scanning or ultrasonography to determine the size and location of the thyroid gland.
Thyroid function tests are also done in older children and adolescents who doctors think may have hypothyroidism. Biotin is a common over-the-counter supplement that can interfere with thyroid function tests by causing false readings of certain hormones. Use of biotin should be stopped for at least 2 days before tests are done. Ultrasonography may also be done in older children and adolescents if the thyroid gland feels asymmetric or the doctor feels a growth (nodule) on the thyroid gland.
Doctors do magnetic resonance imaging (MRI) of the brain and pituitary gland in children who have central hypothyroidism to rule out problems in the brain.
Treatment of Hypothyroidism in Infants and Children
Replacement of thyroid hormone
Children who have congenital or acquired hypothyroidism are usually given the synthetic thyroid hormone levothyroxine. Children who have congenital or acquired hypothyroidism are usually given the synthetic thyroid hormone levothyroxine.Levothyroxine usually is given to children in tablet form. For infants, tablets can be crushed, mixed with a small amount (1 to 2 milliliters) of water, breast milk, or non–soy-based formula, and given by mouth by syringe. It should not be given simultaneously with soy formula or with iron or calcium supplements because these substances can decrease the amount of levothyroxine that is absorbed. Liquid formulations are available commercially for children of any age, but there is limited experience with the use of these formulations in the treatment of congenital hypothyroidism. usually is given to children in tablet form. For infants, tablets can be crushed, mixed with a small amount (1 to 2 milliliters) of water, breast milk, or non–soy-based formula, and given by mouth by syringe. It should not be given simultaneously with soy formula or with iron or calcium supplements because these substances can decrease the amount of levothyroxine that is absorbed. Liquid formulations are available commercially for children of any age, but there is limited experience with the use of these formulations in the treatment of congenital hypothyroidism.
Most children who have congenital hypothyroidism usually need to take thyroid hormone replacement for life. However, some children who have congenital hypothyroidism, usually those who have not required a dose increase after infancy, may be able to stop treatment after they are about 3 years of age.
Doctors continue to monitor children by doing blood tests at regular intervals depending on their age. Children are monitored more frequently during the first few years of life.
Treatment of hypothyroidism is directed by a doctor who specializes in treating children with problems of the endocrine system (called a pediatric endocrinologist).
Prognosis for Hypothyroidism in Infants and Children
Most newborns who are treated have normal movement control and intellectual development.
Even when treated promptly, severe congenital hypothyroidism may still cause subtle developmental problems and hearing loss. Hearing loss may be so mild that it is not detected during the routine newborn screening, but it may still interfere with language learning. To detect subtle hearing loss, infants are tested again when they are older.
Most children with hypothyroidism who properly take their medications achieve normal growth and development.





