

Alopecia is defined as loss of hair from the body. Hair loss is often a cause of great concern to the patient for cosmetic and psychological reasons, but it can also be an important sign of systemic disease.
(See also Alopecia Areata.)
Pathophysiology of Alopecia
Growth cycle
Hair grows in cycles. Each cycle consists of phases:
Anagen: A long (2- to 6-year) growing phase
Catagen: A brief (3-week) transitional apoptotic phase
Telogen: A short (2- to 3-month) resting phase
At the end of the resting phase, the hair falls out (exogen). Normally, about 50 to 100 scalp hairs reach the end of resting phase each day and fall out. When a new hair starts growing in the follicle, the cycle begins again.
Disorders of the growth cycle include
Anagen effluvium—a disruption of the growing phase causing abnormal loss of anagen hairs
Telogen effluvium—significantly more than 100 hairs/day going into resting phase
Classification
Alopecia can be classified as focal or diffuse and by the presence or absence of scarring.
Scarring alopecia is the result of active destruction of the hair follicle. The follicle is irreparably damaged and replaced by fibrotic tissue. Several hair disorders show a biphasic pattern in which nonscarring alopecia occurs early in the course of the disease, and then scarring alopecia and permanent hair loss occurs as the disease progresses. Scarring alopecias can be subdivided further into primary forms, where the target of inflammation is the follicle itself, and secondary forms, where the follicle is destroyed as a result of nonspecific inflammation (see table ).
Nonscarring alopecia results from processes that reduce or slow hair growth without irreparably damaging the hair follicle. Disorders that primarily affect the hair shaft (trichodystrophies) also are considered nonscarring alopecia.
Some Causes of Alopecia
Alopecia Disorder | Causes or Descriptions |
|---|---|
Nonscarring diffuse hair loss | |
Anagen effluvium (caused by agents that impair or disrupt the anagen cycle) | Chemotherapeutic agents Poisoning (eg, thallium, arsenic, other metals) Radiation (also causes scarring focal hair loss) |
Androgenetic alopecia (male-pattern or female-pattern hair loss) | Androgens (eg, dihydrotestosterone) Familial Pathologic hyperandrogenism (virilization in females—see Hirsutism) |
Congenital disorders | Congenital atrichia with papules Ectodermal dysplasia |
Primary hair shaft abnormalities | Easy hair breakage (trichorrhexis nodosa) Genetic disorders Loose anagen hair syndrome Overuse of hair dryers (bubble hair) |
Telogen effluvium (increased number of hairs entering resting phase) | Medications (eg, antimitotic chemotherapeutic agents, anticoagulants, retinoids, oral contraceptives, angiotensin-converting enzyme inhibitors, beta-blockers, lithium, antithyroid medications, antiseizure medications, vitamin A excess)Medications (eg, antimitotic chemotherapeutic agents, anticoagulants, retinoids, oral contraceptives, angiotensin-converting enzyme inhibitors, beta-blockers, lithium, antithyroid medications, antiseizure medications, vitamin A excess) Endocrine problems (eg, hyperthyroidism, hypothyroidism) Nutritional deficiencies (eg, zinc, biotin, or possibly iron deficiency) Physiologic or psychological stress (eg, surgery, systemic or febrile illness, pregnancy) |
Diffuse loss of scalp hair (less common form of alopecia areata) Alopecia totalis (complete scalp hair loss) Alopecia universalis (complete scalp and body hair loss) | |
Commonly causes diffuse hair loss | |
Nonscarring focal hair loss | |
Patchy loss of scalp hair (most common form of alopecia areata) Ophiasis (band pattern hair loss along periphery of temporal and occipital scalp) Sisaipho (central hair loss, sparing hair at the margin of the scalp) | |
Other | Hair loss due to compulsive hair pulling, twisting, or teasing (trichotillomania) Postoperative (pressure-induced) alopecia Primary hair shaft abnormalities (can also cause nonscarring diffuse alopecia) Secondary syphilis Temporal triangular alopecia |
Microsporum audouinii Microsporum canis Trichophyton schoenleinii Trichophyton tonsurans | |
Traction alopecia* | Traction due to braids, rollers, or ponytails (occurs primarily at frontal and temporal hairlines) |
Scarring hair loss (focal or diffuse) | |
Acne keloidalis nuchae | Folliculitis on the occipital scalp that results in scarring alopecia |
Central centrifugal cicatricial alopecia | Progressive scarring alopecia on the crown or vertex of the scalp Most common cause of alopecia in Black patients, typically occurring in women of African descent |
Chronic cutaneous (discoid) lupus | Discoid lupus lesions of the scalp |
Dissecting cellulitis of the scalp | Boggy inflammatory nodules that coalesce with sinus tract formation Part of the follicular occlusion tetrad† |
Lichen planopilaris and frontal fibrosing alopecia | Typically perifollicular erythema and follicular hyperkeratosis Frontal fibrosing alopecia, a variant of lichen planopilaris, characterized by hair loss and scarring in the frontal region of the scalp |
Secondary scarring alopecias | Burns Morphea (localized scleroderma) Progressive systemic sclerosis (scleroderma) Radiation therapy (also causes nonscarring diffuse hair loss) Superinfected kerion (due to severe primary syphilis or severe tinea capitis) Trauma |
* Tinea capitis and traction alopecia can cause scarring if the follicle is sufficiently damaged. | |
† The follicular occlusion tetrad consists of acne conglobata, hidradenitis suppurativa, dissecting cellulitis of the scalp, and pilonidal sinus—disorders that have follicular occlusion in apocrine gland–bearing skin in common. | |
Etiology of Alopecia
The alopecias comprise a large group of disorders with multiple and varying etiologies (see table ).
The most common cause of alopecia is
Androgenetic alopecia (male-pattern or female-pattern hair loss)
Androgenetic alopecia is an androgen-dependent hereditary disorder in which dihydrotestosterone plays a major role. The prevalence of this form of alopecia increases with age, and it can affect over 70% of men (male-pattern hair loss) and 57% of all women (female-pattern hair loss) over the age of 80 (1, 2). However, prevalence rates vary among different populations.

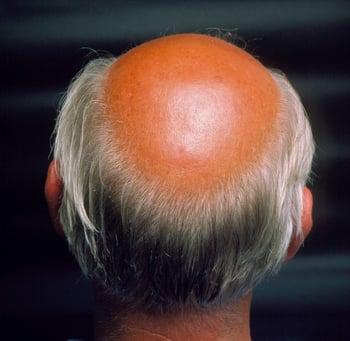
This image shows androgenetic alopecia (male-pattern baldness).
Other common causes of hair loss are
Medications (including chemotherapeutic agents)
Infection (eg, tinea capitis, kerion)
Systemic disorders (eg, disorders that cause high fever, endocrine disorders)
Trauma
Traumatic causes include trichotillomania, traction alopecia, burns, radiation, and pressure-induced (eg, postoperative) hair loss.
Less common causes are
Primary hair shaft abnormalities
Autoimmune diseases
Lichen planopilaris/frontal fibrosing alopecia
Rare dermatologic conditions (eg, dissecting cellulitis of the scalp)
Etiology references
1. Adil A, Godwin M: The effectiveness of treatments for androgenetic alopecia: A systematic review and meta-analysis. J Am Acad Dermatol 77(1):136–141.e5, 2017. doi: 10.1016/j.jaad.2017.02.054
2. Gan DC, Sinclair RD: Prevalence of male and female pattern hair loss in Maryborough. J Investig Dermatol Symp Proc 10(3):184-189, 2005. doi: 10.1111/j.1087-0024.2005.10102.x
Evaluation of Alopecia
History
History of present illness should cover the onset and duration of hair loss, whether hair shedding is increased, and whether hair loss is generalized or localized. Associated symptoms such as pruritus and scaling should be noted. Patients should be asked about typical hair care practices, including use of braids, rollers, and hair dryers, and whether they routinely pull or twist their hair.
Review of systems should include recent exposures to noxious stimuli (eg, medications, illicit drugs, toxins, radiation) and stressors (eg, surgery, chronic illness, fever, psychological stressors). Symptoms of possible causes (eg, fatigue and hot or cold intolerance [hypothyroidism/hyperthyroidism] and, in women, hirsutism, deepening of the voice, and increased libido [virilization]) should be sought. Other features, including dramatic weight loss, dietary practices (including various restrictive diets), and obsessive-compulsive behavior, should be noted. In women, a hormonal/gynecologic/obstetric history should be obtained.
Past medical history should note known possible causes of hair loss, including endocrine and skin disorders. Current and recent medication use should be reviewed for offending agents (see table ). A family history of hair loss should be recorded.
Physical examination
Examination of the scalp should note the distribution of hair loss, the presence and characteristics of any skin lesions, and whether there is scarring. Part widths should be measured. Abnormalities of the hair shafts should be noted.
A full skin examination should be done to evaluate hair loss elsewhere on the body (eg, eyebrows, eyelashes, arms, legs), rashes that may be associated with certain types of alopecia (eg, discoid lupus lesions, signs of secondary syphilis or of other bacterial or fungal infections), and signs of virilization in women (eg, hirsutism, acne, deepening voice, clitoromegaly). Signs of potential underlying systemic disorders should be sought, and a thyroid examination should be done.
Red flags
The following findings are of particular concern:
Virilization in women
Signs of systemic illness or constellations of nonspecific findings possibly indicating poisoning
Interpretation of findings
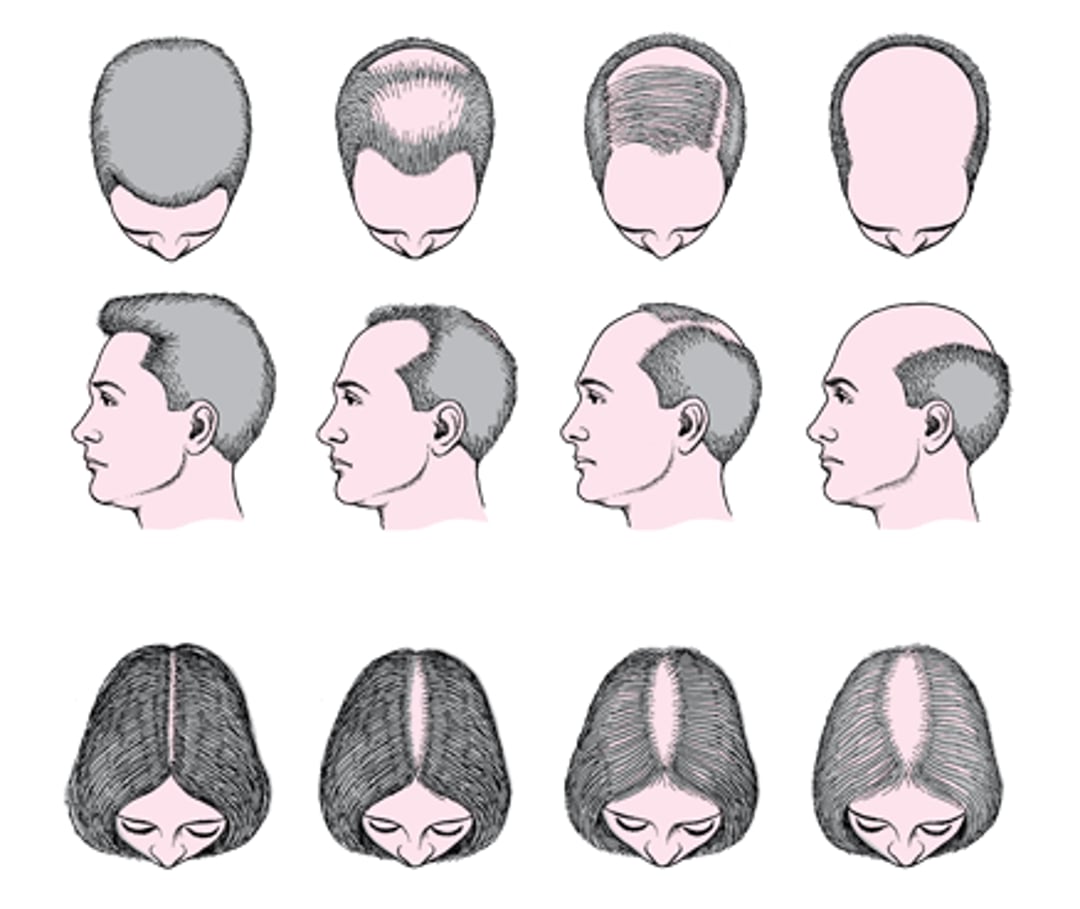
Hair loss that begins at the temples and/or crown (vertex) and spreads to diffuse thinning or nearly complete hair loss is typical of male-pattern hair loss. Hair thinning on the crown manifesting as widening of the central part is typical of female-pattern hair loss (see figure ). In women, this is characterized by a central part width that is wider on the crown of the scalp than it is on the occipital scalp.
Male- and Female-Pattern Hair Loss (Androgenetic Alopecia)

Hair loss that occurs 2 to 4 weeks after chemotherapy or radiation therapy (anagen effluvium) can typically be ascribed to those causes. Hair loss that occurs 3 to 4 months after a major stressor (pregnancy, major febrile illness, surgery, medication change, or severe psychological stressor) suggests a diagnosis of telogen effluvium.
Other findings help suggest alternative diagnoses (see table ).
Interpreting Physical Findings in Alopecia
Finding | Possible Causes |
|---|---|
Asymmetric, bizarre, irregular hair loss pattern | |
Circular, discrete patches of loss; short, broken hairs; exclamation point hairs at periphery of patches | |
Patchy hair loss that appears moth-eaten | |
Pruritus, erythema, and scaling | Chronic cutaneous lupus, lichen planopilaris Tinea capitis (particularly if adenopathy is present) |
Pustules | Scarring dermatologic or infectious process (eg, dissecting cellulitis of the scalp, acne keloidalis nuchae) |
Scalp and body hair loss | Alopecia universalis |
Unruly or unusually wooly hair | Primary hair shaft abnormality |
Virilization (see Hirsutism) | Adrenal disorder or tumor Anabolic steroid use (sometimes surreptitious) |


Anagen effluvium is a physiologic disruption of the anagen (growing) phase. It typically occurs several weeks after chemotherapy or radiation therapy. This photo shows an abrupt loss of hairs in the anagen phase along with sparse broken anagen hairs.
Anagen effluvium is a physiologic disruption of the anagen (growing) phase. It typically occurs several weeks after che
© Springer Science+Business Media


This photo shows typical acneiform lesions and deep keloidal scarring alopecia in a young male with acne keloidalis nuchae.
This photo shows typical acneiform lesions and deep keloidal scarring alopecia in a young male with acne keloidalis nuc
© Springer Science+Business Media


In this photo, the hair pulling is limited to the range of the person's right hand.
In this photo, the hair pulling is limited to the range of the person's right hand.
© Springer Science+Business Media
Anagen effluvium is a physiologic disruption of the anagen (growing) phase. It typically occurs several weeks after chemotherapy or radiation therapy. This photo shows an abrupt loss of hairs in the anagen phase along with sparse broken anagen hairs.
Anagen effluvium is a physiologic disruption of the anagen (growing) phase. It typically occurs several weeks after che
© Springer Science+Business Media
This photo shows typical acneiform lesions and deep keloidal scarring alopecia in a young male with acne keloidalis nuchae.
This photo shows typical acneiform lesions and deep keloidal scarring alopecia in a young male with acne keloidalis nuc
© Springer Science+Business Media
In this photo, the hair pulling is limited to the range of the person's right hand.
In this photo, the hair pulling is limited to the range of the person's right hand.
© Springer Science+Business Media
Other than hair loss, scalp symptoms (eg, itching, burning, tingling) are often absent and, when present, are not specific to any cause.
Signs of hair loss in patterns other than those described above are nondiagnostic and may require microscopic hair examination or scalp biopsy for definitive diagnosis.
Testing
Evaluation for causative disorders (eg, endocrinologic, autoimmune, toxic) should be done based on clinical suspicion.
Male-pattern hair loss usually requires no testing. When it occurs in young men with no family history, the physician should question the patient about use of anabolic steroids and other drugs. In addition to questions regarding prescription medication and illicit drug use, women with significant hair loss and abnormal menses, acne, hirsutism, or other evidence of virilization should have levels of appropriate hormones (eg, testosterone and dehydroepiandrosterone sulfate [DHEAS]) measured (see Hirsutism). Other laboratory testing in women with suspected androgenetic alopecia can include iron, ferritin, vitamin D, and thyroid function testing if indicated by history.
The pull test helps evaluate diffuse scalp hair loss. Gentle traction is exerted on a bunch of hairs (about 40) on at least 3 different areas of the scalp, and the number of extracted hairs is then counted. Normally, < 3 telogen-phase hairs should come out with each pull. If > 4 to 6 hairs come out with each pull, the pull test is positive and is suggestive of telogen effluvium.
Scalp biopsy is indicated when alopecia persists and diagnosis is in doubt. A 4-mm punch biopsy sectioned horizontally is preferred. Biopsy differentiates scarring from nonscarring forms. In cases of suspected cicatricial alopecia, specimens should be taken from areas of active inflammation, typically at the border of a bald patch. Noncicatricial alopecia should be sampled where hair is most sparse, typically in the center of the lesion. Fungal and bacterial cultures may be useful.
Daily hair counts can be done by the patient to quantify hair loss when the pull test is negative. Hairs lost during the first morning combing or during washing are collected in clear plastic bags daily for 14 days. The number of hairs in each bag is then recorded. Scalp hair counts of > 100/day are abnormal except after shampooing, when hair counts of up to 250 may be normal. Hairs may be brought in by the patient for microscopic examination.
Treatment of Alopecia
Medications (including hormonal modulators)
Laser light therapy
Surgery
Androgenetic alopecia
MinoxidilMinoxidil works by mechanisms that are not completely understood to shorten the telogen phase, lengthen the anagen phase, and promote growth in hair follicle diameter and length. Topical minoxidil (2% for women, 2% or 5% for men) 1 mL twice a day applied to the scalp is most effective for vertex alopecia in male-pattern or female-pattern hair loss. The 5% preparation is more efficacious than the 2% solution but causes more pruritus and irritation (works by mechanisms that are not completely understood to shorten the telogen phase, lengthen the anagen phase, and promote growth in hair follicle diameter and length. Topical minoxidil (2% for women, 2% or 5% for men) 1 mL twice a day applied to the scalp is most effective for vertex alopecia in male-pattern or female-pattern hair loss. The 5% preparation is more efficacious than the 2% solution but causes more pruritus and irritation (1). However, usually only a subset of patients experience significant hair growth, adherence is often a limiting factor, and minoxidil is generally not effective or indicated for other causes of hair loss except possibly ). However, usually only a subset of patients experience significant hair growth, adherence is often a limiting factor, and minoxidil is generally not effective or indicated for other causes of hair loss except possiblyalopecia areata and telogen effluvium. Hair regrowth can take 8 to 12 months. Treatment is continued indefinitely because, once treatment is stopped, hair loss resumes. The most frequent adverse effects are mild scalp irritation, allergic contact dermatitis, and increased facial hair. Low-dose oral minoxidil in doses ranging from 0.25 to 5 mg once/day is sometimes used off-label, but facial hypertrichosis and rarely cardiovascular adverse events can occur (, and increased facial hair. Low-dose oral minoxidil in doses ranging from 0.25 to 5 mg once/day is sometimes used off-label, but facial hypertrichosis and rarely cardiovascular adverse events can occur (2, 3).
FinasterideFinasteride inhibits the 5-alpha-reductase enzyme, blocking conversion of testosterone to dihydrotestosterone, and is useful for male-pattern hair loss. Finasteride 1 mg orally once/day can stop hair loss and can stimulate hair growth. Efficacy is usually evident within 6 to 8 months of treatment. Adverse effects include decreased libido; erectile and ejaculatory dysfunction, which may persist even after cessation of treatment (see to dihydrotestosterone, and is useful for male-pattern hair loss. Finasteride 1 mg orally once/day can stop hair loss and can stimulate hair growth. Efficacy is usually evident within 6 to 8 months of treatment. Adverse effects include decreased libido; erectile and ejaculatory dysfunction, which may persist even after cessation of treatment (seeMale Sexual Dysfunction); hypersensitivity reactions; gynecomastia; myopathy; and rarely symptoms of depression and suicidal ideation (4). There may be a decrease in prostate-specific antigen (PSA) levels in older men, which should be taken into account when this test is used for cancer screening. Common practice is to continue treatment for as long as positive results persist. Once treatment is stopped, hair loss returns to previous levels. Finasteride is sometimes used off-label in women of non-childbearing potential; it is contraindicated in pregnant women because it has teratogenic effects in animals.levels in older men, which should be taken into account when this test is used for cancer screening. Common practice is to continue treatment for as long as positive results persist. Once treatment is stopped, hair loss returns to previous levels. Finasteride is sometimes used off-label in women of non-childbearing potential; it is contraindicated in pregnant women because it has teratogenic effects in animals.
Dutasteride,Dutasteride, a medication used to treat benign prostatic hyperplasia, is a stronger inhibitor of 5-alpha-reductase than finasteride and is sometimes used off-label to treat androgenetic alopecia (, is a stronger inhibitor of 5-alpha-reductase than finasteride and is sometimes used off-label to treat androgenetic alopecia (3).
Hormonal modulators such as spironolactone may be useful for female-pattern hair loss (such as spironolactone may be useful for female-pattern hair loss (5–7).
Low-level laser light therapy is an alternate or additional treatment for androgenetic alopecia that has been shown to promote hair growth (8). Physician-dispensed and over-the-counter devices are available.
Autologous platelet-rich plasma injected into the scalp is thought to contain growth factors that promote hair follicle growth and maintenance (9).
Surgical options include follicle transplant, scalp flaps, and alopecia reduction. Few procedures have been subjected to scientific scrutiny, but patients who are self-conscious about their hair loss may consider them (7).
Hair loss due to other causes
Underlying disorders are treated.
Treatment for alopecia areata includes topical, intralesional, or, in severe cases, systemic corticosteroids, topical minoxidil, topical anthralin, topical immunotherapy (diphenylcyclopropenone or squaric acid dibutylester), baricitinib, ritlecitinib, and methotrexate.Treatment for alopecia areata includes topical, intralesional, or, in severe cases, systemic corticosteroids, topical minoxidil, topical anthralin, topical immunotherapy (diphenylcyclopropenone or squaric acid dibutylester), baricitinib, ritlecitinib, and methotrexate.
Treatment for traction alopecia is elimination of physical traction or stress to the scalp.
Treatment for tinea capitis is oral antifungals.
Trichotillomania is difficult to treat, but behavior modification, clomipramine, or a is difficult to treat, but behavior modification, clomipramine, or aselective serotonin reuptake inhibitor (SSRI—eg, fluoxetine, fluvoxamine, paroxetine, sertraline, citalopram) may be of benefit.(SSRI—eg, fluoxetine, fluvoxamine, paroxetine, sertraline, citalopram) may be of benefit.
Scarring alopecia as in central centrifugal cicatricial alopecia or dissecting cellulitis of the scalp is best treated with an oral tetracycline plus a potent topical or intralesional corticosteroid. Severe or chronic acne keloidalis nuchae can be treated similarly; if mild, topical retinoids, topical antibiotics, and/or topical benzoyl peroxide may suffice.Scarring alopecia as in central centrifugal cicatricial alopecia or dissecting cellulitis of the scalp is best treated with an oral tetracycline plus a potent topical or intralesional corticosteroid. Severe or chronic acne keloidalis nuchae can be treated similarly; if mild, topical retinoids, topical antibiotics, and/or topical benzoyl peroxide may suffice.
Lichen planopilaris, frontal fibrosing alopecia (a variant of lichen planopilaris), and chronic cutaneous lupus lesions may be treated with medications such as oral antimalarials, topical or intralesional corticosteroids, topical calcineurin inhibitors such as tacrolimus or pimecrolimus, topical or oral Janus kinase inhibitors (Lichen planopilaris, frontal fibrosing alopecia (a variant of lichen planopilaris), and chronic cutaneous lupus lesions may be treated with medications such as oral antimalarials, topical or intralesional corticosteroids, topical calcineurin inhibitors such as tacrolimus or pimecrolimus, topical or oral Janus kinase inhibitors (10, 11) or oral immunosuppressants (10, 12). Finasteride and dutasteride (). Finasteride and dutasteride (10, 13, 14) can be prescribed to treat frontal fibrosing alopecia while retinoids, dapsone, thalidomide, lenalidomide, anifrolumab, and rituximab can be prescribed for chronic, refractory cutaneous lupus lesions () can be prescribed to treat frontal fibrosing alopecia while retinoids, dapsone, thalidomide, lenalidomide, anifrolumab, and rituximab can be prescribed for chronic, refractory cutaneous lupus lesions (15).
Hair loss due to chemotherapy (anagen effluvium) is temporary and is best treated with a wig; when hair regrows, it may be different in color and texture from the original hair. Hair loss due to telogen effluvium is usually temporary as well and abates after the precipitating agent is eliminated.
Treatment references
1. Olsen EA, Dunlap FE, Funicella T, et al: A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. : A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men.J Am Acad Dermatol 47(3):377-385, 2002. doi: 10.1067/mjd.2002.124088
2. Randolph M, Tosti A: Oral minoxidil treatment for hair loss: A review of efficacy and safety. : Oral minoxidil treatment for hair loss: A review of efficacy and safety.J Am Acad Dermatol 84(3):737–746, 2021. doi: 10.1016/j.jaad.2020.06.1009
3. Gupta AK, Venkataraman M, Talukder M, Bamimore MA: Relative efficacy of minoxidil and the 5-α reductase inhibitors in androgenetic alopecia treatment of male patients: A network meta-analysis. : Relative efficacy of minoxidil and the 5-α reductase inhibitors in androgenetic alopecia treatment of male patients: A network meta-analysis.JAMA Dermatol 158(3):266–274, 2022. doi: 10.1001/jamadermatol.2021.5743
4. Nguyen D-D, Marchese M, Cone EB, et al: Investigation of suicidality and psychological adverse events in patients treated with finasteride. : Investigation of suicidality and psychological adverse events in patients treated with finasteride.JAMA Dermatol 157(1):35-42, 2021. doi:10.1001/jamadermatol.2020.3385
5. Sinclair R, Wewerinke M, Jolley D: Treatment of female pattern hair loss with oral antiandrogens. Br J Dermatol 152(3):466-73, 2005. doi: 10.1111/j.1365-2133.2005.06218.x
6. Famenini S, Slaught C, Duan L, et al: Demographics of women with female pattern hair loss and the effectiveness of spironolactone therapy. : Demographics of women with female pattern hair loss and the effectiveness of spironolactone therapy.J Am Acad Dermatol 73(4):705-6, 201570. doi: 10.1016/j.jaad.2015.06.063
7. Adil A, Godwin M. The effectiveness of treatments for androgenetic alopecia: A systematic review and meta-analysis. J Am Acad Dermatol 77(1):136-141.e5, 2017. doi: 10.1016/j.jaad.2017.02.054
8. Jimenez JJ, Wikramanayake TC, Bergfeld W, et al: Efficacy and safety of a low-level laser device in the treatment of male and female pattern hair loss: A multicenter, randomized, sham device-controlled, double-blind study. Am J Clin Dermatol 15(2):115-27, 2014. doi: 10.1007/s40257-013-0060-6
9. Hesseler MJ, Shyam N: Platelet-rich plasma and its utilities in alopecia: A systematic review. Dermatol Surg 46(1):93–102, 2020. doi: 10.1097/DSS.0000000000001965
10. Ezemma O, Devjani S, Kelley KJ, et al: Treatment modalities for lymphocytic and neutrophilic scarring alopecia. J Am Acad Dermatol 89(2S):S33-S35, 2023. doi: 10.1016/j.jaad.2023.04.023
11. Abduelmula A, Sood S, Mufti A, et al: Management of cutaneous lupus erythematosus with Janus kinase inhibitor therapy: An evidence-based review. J Am Acad Dermatol 89(1):130-131. doi: 10.1016/j.jaad.2022.12.037
12. Fechine COC, Valente NYS, Romiti R: Lichen planopilaris and frontal fibrosing alopecia: Review and update of diagnostic and therapeutic features. An Bras Dermatol 97(3):348-357, 2022. doi: 10.1016/j.abd.2021.08.008
13. Ho A, Shapiro J: Medical therapy for frontal fibrosing alopecia: A review and clinical approach. J Am Acad Dermatol 81(2):568-580, 2019. doi: 10.1016/j.jaad.2019.03.079
14. Pindado-Ortega C, Saceda-Corralo D, Moreno-Arrones, et al: Effectiveness of dutasteride in a large series of patients with frontal fibrosing alopecia in real clinical practice. : Effectiveness of dutasteride in a large series of patients with frontal fibrosing alopecia in real clinical practice.J Am Acad Dermatol 84(5):1285-1294, 2021. doi: 10.1016/j.jaad.2020.09.093
15. Verdelli A, Corrà A, Mariotti EB, et al: An update on the management of refractory cutaneous lupus erythematosus. Front Med (Lausanne) 9:941003, 2022. doi: 10.3389/fmed.2022.941003
Key Points
Androgenetic alopecia (male-pattern and female-pattern hair loss) is the most common type of hair loss.
Concomitant virilization in women should prompt a thorough evaluation for an underlying disorder.
Microscopic hair examination or scalp biopsy may be required for definitive diagnosis.
Treatments include topical minoxidil or oral finasteride for male-pattern hair loss; topical minoxidil, or spironolactone for female-pattern hair loss; and sometimes scalp injections with platelet-rich plasma, low level laser light therapy, follicle transplant, or other surgical procedures. Treatments include topical minoxidil or oral finasteride for male-pattern hair loss; topical minoxidil, or spironolactone for female-pattern hair loss; and sometimes scalp injections with platelet-rich plasma, low level laser light therapy, follicle transplant, or other surgical procedures.
Drug Information for the Topic





