



Paragonimiasis is infection with the lung fluke Paragonimus westermani and related species. Humans are infected by eating raw, pickled, or undercooked freshwater crustaceans. Most infections are asymptomatic, but pulmonary symptoms may occur, including chronic cough, chest pain, dyspnea, and hemoptysis. Ectopic flukes can cause allergic skin reactions and central nervous system abnormalities, including seizures, aphasia, paresis, and visual disturbances. Diagnosis is by identifying eggs in sputum, feces, or pleural or peritoneal fluid. Serologic tests are also available. Praziquantel is the treatment of choice.
Flukes are parasitic flatworms that infect various parts of the body (eg, blood vessels, gastrointestinal tract, lungs, liver) depending on the species.
Although > 30 species of Paragonimus exist and 10 have been reported to infect humans, P. westermani is the most frequent cause of disease (1, 2).
The most important endemic areas are in Asia, principally Korea, Japan, Taiwan, the highlands of China, and the Philippines. Endemic foci with other Paragonimus species exist in West and Central Africa (P. africanus) and in parts of South and Central America (P. mexicanus). P. kellicotti has caused human infection in North America.
Pathophysiology of Paragonimiasis
Eggs passed in sputum or feces develop for 2 to 3 weeks in freshwater before miracidia (first larval stage) hatch. The miracidia invade snails; there, they develop, multiply, and eventually emerge as cercariae (free-swimming larvae). Cercariae penetrate freshwater crabs or crayfish and encyst to form metacercariae. Humans become infected by eating raw, salted, pickled, smoked, or undercooked crustaceans, thus inadvertently ingesting metacercariae. Metacercariae then excyst in the human gastrointestinal tract, penetrate the intestinal wall, and move into the peritoneal cavity, then through the diaphragm into the pleural cavity; they enter lung tissue, become encapsulated, and develop into hermaphroditic adult worms, which produce eggs. Adult worms grow to about 7.5 to 12 mm by 4 to 6 mm. From the lungs, eggs exit the body in sputum that is coughed up and spit out or swallowed and passed in feces.
Worms may also reach the brain, liver, lymph nodes, skin, and spinal cord and develop there. However, in these organs, the life cycle cannot be completed because the eggs have no way to exit the body. Adult flukes may persist for 20 to 25 years.

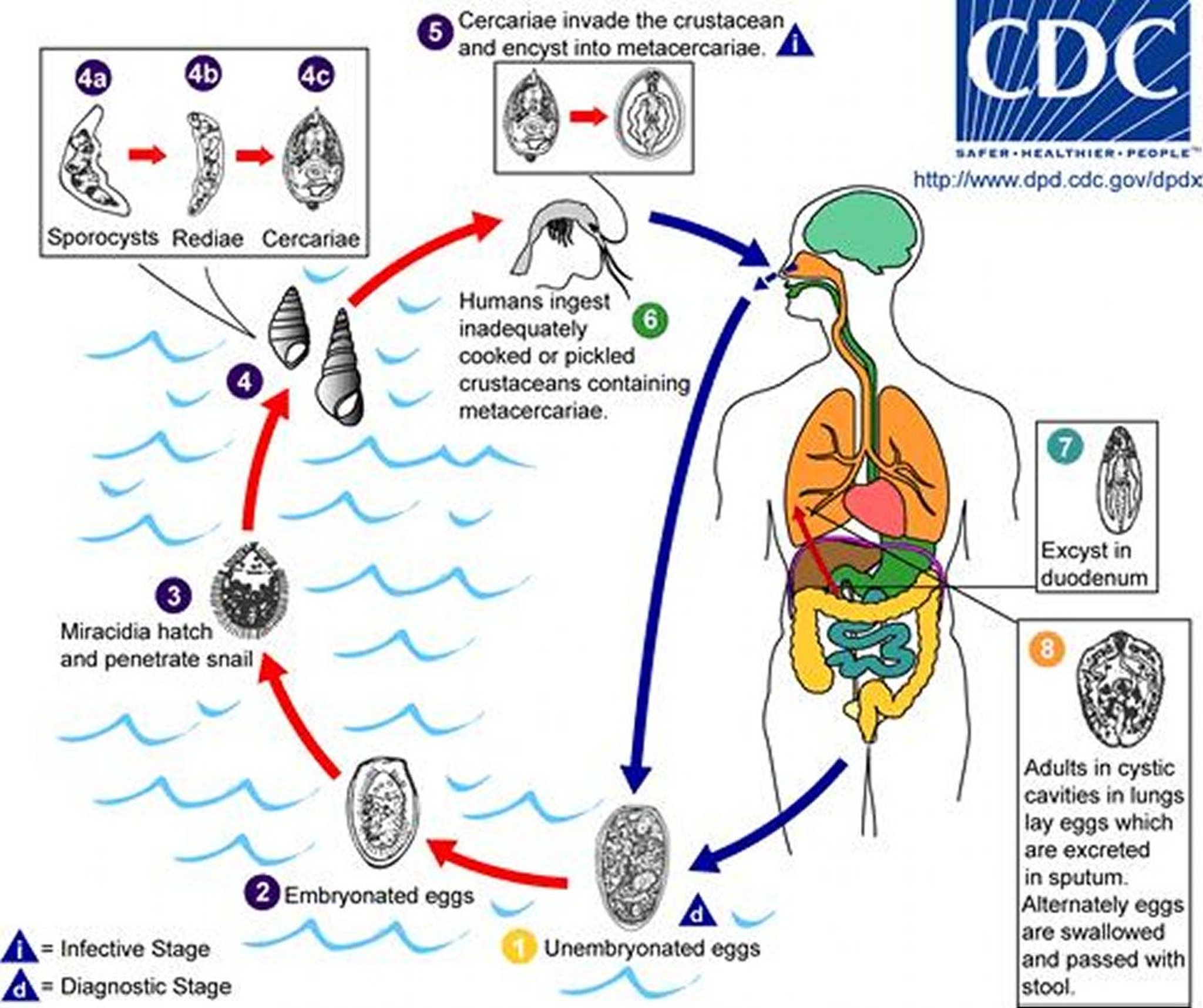
1. In the human host, unembryonated eggs pass out of the body in sputum, or they are swallowed and passed with feces.
2. In the external environment, eggs become embryonated, and miracidia hatch.
3. Miracidia seek a snail (first intermediate host), and penetrate its soft tissues.
4. Inside the snail, miracidia develop into sporocysts, then rediae, and then many cercariae, which emerge from the snail.
5. Cercariae invade a crustacean such as a crab or crayfish (2nd intermediate host), where they encyst (form cystic structures) and become metacercariae (the infective stage for mammalian hosts).
6. Humans are infected with P. westermani by eating inadequately cooked or pickled freshwater crab or crayfish that contain metacercariae.
7. The metacercariae excyst (rupture out of existing cysts) in the duodenum.
8. They then penetrate the intestinal wall and move into the peritoneal cavity, then through the abdominal wall and diaphragm into the lungs; there, they become encapsulated and develop into adults, which produce eggs. The eggs exit the body in sputum that is coughed up and spit out or swallowed and passed in feces. The worms can also reach other organs and tissues, but in such sites, the life cycle cannot be completed because the eggs cannot exit the body.
Image from the Centers for Disease Control and Prevention Image Library.
Other hosts include pigs, dogs, and a variety of feline species.
Symptoms and Signs of Paragonimiasis
Most people with paragonimiasis are asymptomatic. During the acute phase of infection, characterized by invasion and migration of the flukes, diarrhea, abdominal pain, fever, cough, urticaria, hepatosplenomegaly, pulmonary abnormalities, and eosinophilia may develop.
During the chronic phase, the lungs are damaged most, but other organs may be involved. Manifestations of pulmonary infection develop slowly and include chronic cough, chest pain, expectoration of sputum, hemoptysis, and dyspnea; the clinical picture resembles and is often confused with tuberculosis or Löffler syndrome. Pleural effusions may be present.
Cerebral infections manifest as space-occupying lesions, often within a year after the onset of pulmonary disease. Seizures, aphasia, paresis, and visual disturbances occur.
Migratory allergic skin lesions similar to those of cutaneous larva migrans (painless subcutaneous swellings of varying sizes, or tender firm nodules, both containing immature flukes) are common in infections with P. skrjabini but also occur with other species.
Diagnosis of Paragonimiasis
Microscopic examination of sputum and feces
Serologic tests to detect antibodies
Sometimes imaging (chest radiographs and CT)
Diagnosis of paragonimiasis is based on identifying the characteristic large operculated eggs in sputum or feces. Occasionally, eggs may be found in pleural, bronchoalveolar lavage, or peritoneal fluid. Eggs may be difficult to identify in sputum or feces because they are released intermittently and in small numbers. Concentration techniques increase sensitivity.


P. westermani eggs range from 80 to 120 micrometers long by 45 to 70 micrometers wide. They are yellow-brown, ovoid or elongate, and have a thick shell. The eggs are often asymmetrical with one end slightly flattened. At the large end, the operculum is clearly visible. The abopercular end is thickened.
The eggs are unembryonated when passed in sputum or feces.
CDC/DPDx
Serologic tests to detect antibodies are useful in light infections and in the diagnosis of extrapulmonary paragonimiasis. Technical difficulties and potential cross-reactivity of the original complement fixation text has led to the development of enzyme immunoassays (EIA) as a replacement; however the complement fixation test may still be in use in some regions. In the United States, an immunoblot assay with P. westermani antigen is available from the CDC.
Radiographs provide ancillary information but are not diagnostic; chest radiographs and CT may show a diffuse infiltrate, nodules, annular ring shadow lesions, cavitations, linear opacities, lung abscesses, pleural effusion, and/or pneumothorax.
Treatment of Paragonimiasis
Praziquantel
Triclabendazole
Praziquantel orally 3 times a day for 2 days is the medication of choice for paragonimiasis. Praziquantel is also used to treat extrapulmonary infections, but multiple courses may be required.
For cerebral infections, a short course of glucocorticoids may be given with praziquantel to reduce the inflammatory response induced by dying flukes.
Triclabendazole is an acceptable treatment in areas where it is available; it is dosed orally once postprandially or, for severe infections, 2 doses given postprandially 12 hours apart.
Surgery may be needed to excise skin lesions or, rarely, brain cysts.
The best prevention is to avoid eating raw, salted, pickled, smoked, or undercooked crustaceans (eg, freshwater crabs and crayfish) from endemic waters.
References
1. Centers for Disease Control and Prevention: DPDx–Laboratory Identification of Parasites of Public Health Concern: Paragonimiasis. June 6, 2024. Accessed July 2, 2025.
2. World Health Organization: Neglected tropical diseases: Paragonimiasis. July 28, 2020. Accessed July 2, 2025.
Drug Information for the Topic





