

The autonomic nervous system regulates physiologic processes. Regulation occurs without conscious control, ie, autonomously. The 2 major divisions are the
Sympathetic system
Parasympathetic system
Disorders of the autonomic nervous system cause autonomic insufficiency or failure and can affect any system of the body.
Anatomy of the Autonomic Nervous System
The autonomic nervous system receives input from parts of the central nervous system (CNS) that process and integrate stimuli from the body and external environment. These parts include the hypothalamus, nucleus of the solitary tract, reticular formation, amygdala, hippocampus, and olfactory cortex.
The sympathetic and parasympathetic systems each consist of 2 sets of nerve bodies:
Preganglionic: This set is located in the CNS, with connections to another set of nerves in ganglia outside the CNS.
Postganglionic: This set has efferent fibers that go from the ganglia to effector organs (see figure ).
The Autonomic Nervous System

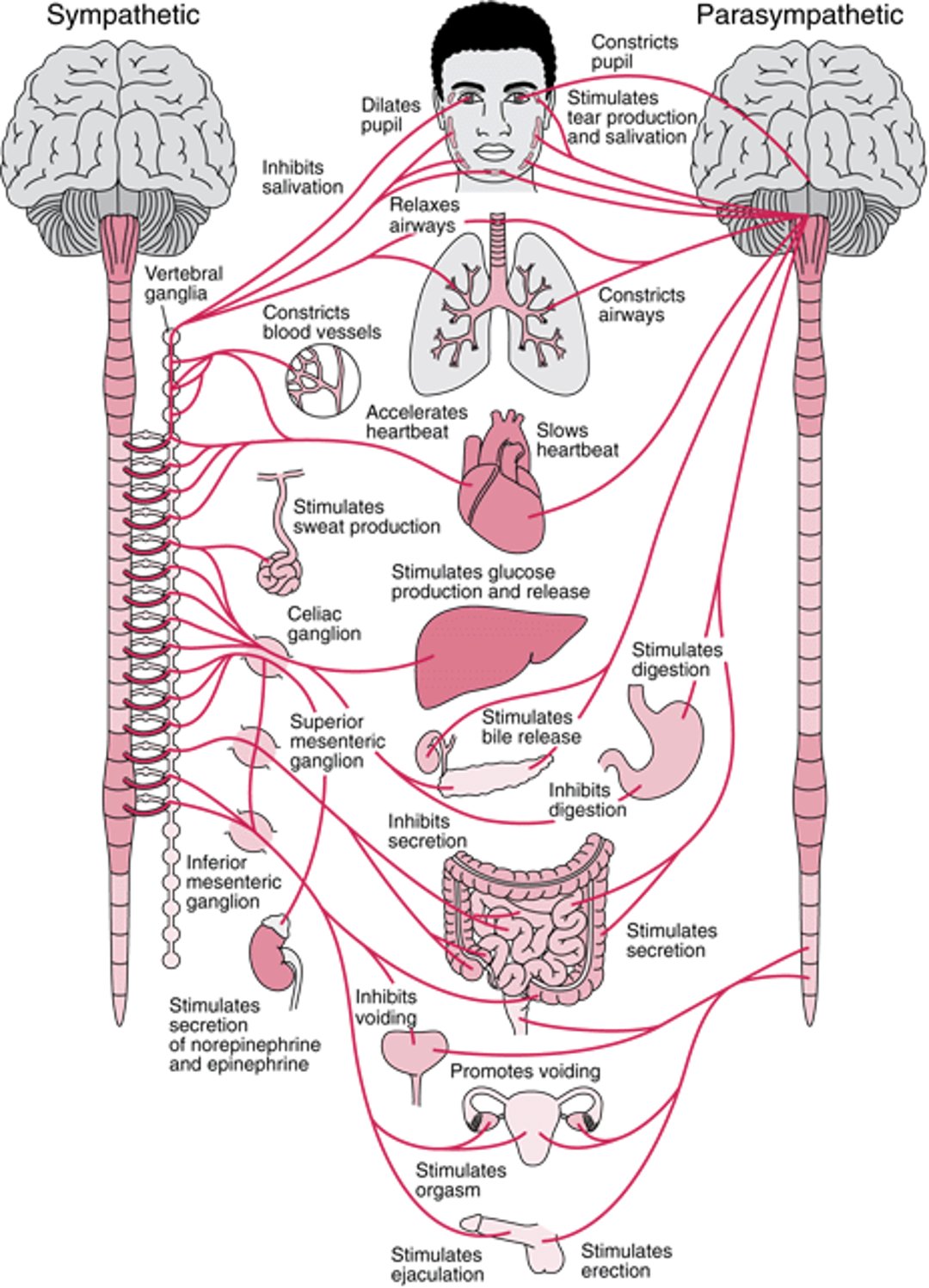
Sympathetic system
The preganglionic cell bodies of the sympathetic system are located in the intermediolateral horn of the spinal cord between T1 and L2 or L3.
The sympathetic ganglia are adjacent to the spine and consist of the vertebral (sympathetic chain) and prevertebral ganglia, including the superior cervical, celiac, superior mesenteric, inferior mesenteric, and aorticorenal ganglia.
Long fibers run from these ganglia to effector organs, including the following:
Smooth muscle of blood vessels, viscera, lungs, scalp (piloerector muscles), and pupils
Heart
Glands (sweat, salivary, and digestive)
Parasympathetic system
The preganglionic cell bodies of the parasympathetic system are located in the brain stem and sacral portion of the spinal cord. Preganglionic fibers exit the brain stem with the 3rd, 7th, 9th, and 10th (vagus) cranial nerves and exit the spinal cord at S2 and S3; the vagus nerve contains about 75% of all parasympathetic fibers.
Parasympathetic ganglia (eg, ciliary, sphenopalatine, otic, pelvic, and vagal ganglia) are located within the effector organs, and postganglionic fibers are only 1 or 2 mm long. Thus, the parasympathetic system can produce specific, localized responses in effector organs, including:
Blood vessels of the head, neck, and thoracoabdominal viscera
Lacrimal and salivary glands
Smooth muscle of glands and viscera (eg, liver, spleen, colon, kidneys, bladder, genitals)
Muscles of the pupil
Physiology of the Autonomic Nervous System
The autonomic nervous system is involved in control of blood pressure (BP), heart rate, body temperature, weight, digestion, metabolism, fluid and electrolyte balance, sweating, urination, defecation, sexual response, and other processes. Many organs are controlled primarily by either the sympathetic or parasympathetic system, although they may receive input from both; occasionally, functions are reciprocal (eg, sympathetic input increases heart rate; parasympathetic decreases it).
The sympathetic nervous system is catabolic; it activates fight-or-flight responses.
The parasympathetic nervous system is anabolic; it conserves and restores (see table ).
Divisions of the Autonomic Nervous System
Division | Some Effects |
|---|---|
Sympathetic | Increases the following:
Causes palms to sweat Decreases functions not necessary for immediate survival (eg, digestion) Controls ejaculation |
Parasympathetic | Stimulates gastrointestinal secretions and motility (including bowel evacuation) Slows heart rate Reduces blood pressure Controls erection |
The 2 major neurotransmitters in the autonomic nervous system are:
Acetylcholine: Fibers that secrete acetylcholine (cholinergic fibers) include all preganglionic fibers, all postganglionic parasympathetic fibers, and some postganglionic sympathetic fibers (those that innervate piloerectors and sweat glands).
Norepinephrine: Fibers that secrete norepinephrine (adrenergic fibers) include most postganglionic sympathetic fibers. Sweat glands on the palms and soles also respond to adrenergic stimulation to some degree.
There are different subtypes of adrenergic receptors and cholinergic receptors, which vary by location.
Etiology of Autonomic Insufficiency
Disorders causing autonomic insufficiency or failure can originate in the peripheral or central nervous system and may be primary or secondary to other disorders.
The most common causes of autonomic insufficiency are:
Other causes include:
Autoimmune autonomic ganglionopathy
Disorders of the neuromuscular junction (eg, botulism, Lambert-Eaton syndrome)
Certain viral infections, including COVID-19
Injury to nerves in the neck, including injury due to surgery
Certain medications
Autonomic insufficiency that occurs with COVID-19 typically develops after recovery from the respiratory and other acute systemic symptoms of COVID (1). One manifestation is postural orthostatic tachycardia syndrome (POTS), which is characterized by abnormal autonomic responses when upright. The mechanism is unknown.
Etiology reference
1. Jamal SM, Landers DB, Hollenberg SM, et al. Prospective Evaluation of Autonomic Dysfunction in Post-Acute Sequela of COVID-19. J Am Coll Cardiol 2022;79(23):2325-2330. doi:10.1016/j.jacc.2022.03.357
Evaluation of Autonomic Insufficiency
History
Symptoms suggesting autonomic insufficiency include:
Orthostatic intolerance (development of autonomic symptoms such as lightheadedness that is relieved by sitting down) due to orthostatic hypotension or postural orthostatic tachycardia (POTS)
Heat intolerance
Loss of bladder and bowel control
Sexual dysfunction, including male erectile dysfunction
Other possible symptoms include dry eyes and dry mouth, but they are less specific.
Physical examination
Important parts of the examination include the following:
Postural blood pressure (BP) and heart rate: In a normally hydrated patient, a sustained (eg, > 1 minute) decrease of at least 20 mm Hg in systolic BP or a decrease of at least 10 mm Hg in diastolic BP with standing indicates orthostatic hypotension. Heart rate change with respiration and standing should be noted; absence of physiologic sinus arrhythmia and failure of heart rate to increase with standing indicate autonomic insufficiency. In contrast, patients with postural orthostatic tachycardia syndrome typically have postural tachycardia with a rise in heart rate greater than 30 beats per minute (or 40 beats per minute in children) without hypotension.
Eye examination: Miosis and mild ptosis (Horner syndrome) suggest a sympathetic lesion. A dilated, unreactive pupil (Adie pupil) suggests a parasympathetic lesion.
Genitourinary (GU) and rectal reflexes: Abnormal GU and rectal reflexes may indicate autonomic nervous system deficits. Testing includes the cremasteric reflex (normally, stroking the upper inner thigh results in retraction of the testes), anal wink reflex (normally, stroking perianal skin results in contraction of the anal sphincter), and bulbocavernosus reflex (normally, squeezing the glans penis or clitoris results in contraction of the anal sphincter). In practice, the GU and rectal reflexes are rarely tested.
Laboratory testing
If patients have symptoms and signs suggesting autonomic impairment, sudomotor, cardiovagal, and adrenergic testing is usually done to help determine severity and distribution of the impairment (1).
Sudomotor testing includes the following:
Quantitative sudomotor axon-reflex test: This test evaluates the integrity of postganglionic fibers. The fibers are activated by iontophoresis using acetylcholine. Standard sites on the leg and arm are tested, and the volume of sweat is then measured. The test can detect decreased or absent sweat production.
Thermoregulatory sweat test: This test evaluates both preganglionic and postganglionic pathways. After an indicator powder is applied to the skin, patients enter a closed compartment that is heated to cause maximal sweating. Sweating causes the powder to change color, so that areas of anhidrosis and hypohidrosis are apparent and can be calculated as a percentage of body surface area.
Cardiovagal testing evaluates heart rate response (via ECG rhythm strip) to deep breathing and to the Valsalva maneuver (forced expiration against a closed glottis). If the autonomic nervous system is intact, heart rate varies with these maneuvers; normal responses to deep breathing and the Valsalva ratio vary by age. The Valsalva ratio is the maximum heart rate during the Valsalva maneuver divided by the heart rate 30 seconds after the maneuver. The lower limit for normal is 1.0.
Adrenergic testing evaluates response of beat-to-beat BP to the following:
Head-up tilt (tilt table testing): Blood shifts to dependent parts, causing reflex responses in BP and heart rate. This test helps differentiate orthostatic hypotension from postural orthostatic tachycardia syndrome.
Valsalva maneuver: This maneuver increases intrathoracic pressure and reduces venous return, causing changes in BP and heart rate that reflect vagal and adrenergic baroreflex function.
Plasma norepinephrine levels can be measured with patients supine and then after they stand for > 5 minutes. Normally, levels increase after standing. If patients have autonomic impairment, levels may not increase with standing and may be low in the supine position, particularly in postganglionic disorders (eg, autonomic neuropathy, pure autonomic failure).
Reference
1. Cheshire WP, Freeman R, Gibbons CH, et al. Electrodiagnostic assessment of the autonomic nervous system: A consensus statement endorsed by the American Autonomic Society, American Academy of Neurology, and the International Federation of Clinical Neurophysiology [published correction appears in Clin Neurophysiol 2021 May;132(5):1194. doi: 10.1016/j.clinph.2021.02.006]. Clin Neurophysiol 2021;132(2):666-682. doi:10.1016/j.clinph.2020.11.024





