

Cholecystitis is inflammation of the gallbladder, usually resulting from a gallstone blocking the cystic duct.
Typically, people have abdominal pain, fever, and nausea.
Ultrasound can usually detect signs of gallbladder inflammation.
The gallbladder may need to be removed, usually with surgery using a viewing tube called a laparoscope.
The gallbladder is a small, pear-shaped sac located beneath the liver. It stores bile, a fluid that is produced by the liver and aids in digestion. When bile is needed, such as when people eat, the gallbladder contracts, pushing bile through the bile ducts into the small intestine. (See also Overview of Gallbladder and Bile Duct Disorders and figure .)
Cholecystitis is the most common problem resulting from gallbladder stones. It usually occurs when a stone blocks the cystic duct, which carries bile out from the gallbladder to the GI tract.
Cholecystitis is classified as acute or chronic.
Acute cholecystitis
Acute cholecystitis begins suddenly, resulting in severe, steady pain in the upper abdomen. At least 90% of people with acute cholecystitis have gallstones. The inflammation almost always begins without infection, although infection may develop later. Inflammation may cause the gallbladder to fill with fluid and its walls to thicken.
Rarely, a form of acute cholecystitis without gallstones (acalculous cholecystitis) occurs. However, the gallbladder may contain sludge (microscopic particles of materials similar to those in gallstones). Acalculous cholecystitis is more serious than other types of cholecystitis. It tends to occur after the following:
Major surgery
Critical illnesses such as serious injuries, severe burns, or a bloodstream infection (sepsis)
Intravenous feedings for a long time
Fasting for a long time
A deficiency in the immune system
Certain disorders involving blood vessel inflammation (vasculitis), such as systemic lupus erythematosus or polyarteritis nodosa
Acute acalculous cholecystitis can occur in young children after an infectious illness with a fever; usually the source of the illness is not known.
Chronic cholecystitis
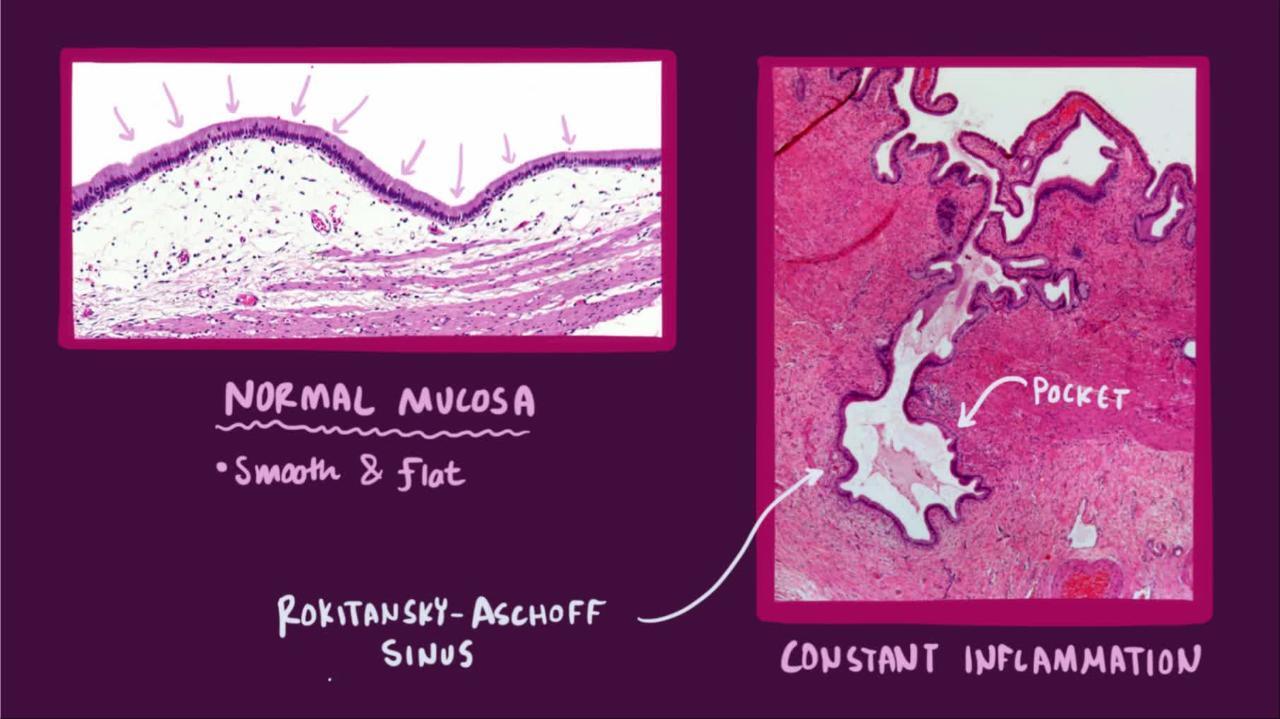
Chronic cholecystitis is gallbladder inflammation that has lasted a long time. It almost always results from gallstones and from prior attacks of acute cholecystitis. Chronic cholecystitis is characterized by repeated attacks of pain (biliary colic) that occur when gallstones periodically block the cystic duct.
In chronic cholecystitis, the gallbladder is damaged by repeated attacks of acute inflammation, usually due to gallstones, and may become thick-walled, scarred, and small. The gallstones may block the opening of the gallbladder into the cystic duct or block the cystic duct itself. The gallbladder usually also contains sludge. If scarring is extensive, calcium may be deposited in the walls of the gallbladder, causing them to harden (called porcelain gallbladder).

Symptoms of Cholecystitis
A gallbladder attack, whether in acute or chronic cholecystitis, begins as pain.
Acute cholecystitis
The pain of acute cholecystitis is similar to biliary colic (pain caused by gallstones) but is more severe and lasts longer. The pain peaks after 15 to 60 minutes and then remains constant, lasting 6 hours or longer. It usually occurs in the upper right part of the abdomen. The pain may become excruciating. Most people feel a sharp pain when a doctor presses on the upper right part of the abdomen. Breathing deeply may worsen the pain. The pain often extends to the lower part of the right shoulder blade or to the back. Nausea and vomiting are common.
Within a few hours, the abdominal muscles on the right side may become stiff. Fever is common and may be accompanied by chills.
In older adults, the first or only symptoms of cholecystitis may be vague. For example, older people may lose their appetite, feel tired or weak, or vomit. They may not develop a fever.
Typically, an attack subsides in 2 to 3 days and completely resolves in a week. If the acute episode persists, it may signal a serious complication. Increasingly severe pain, a high fever, and chills suggest pockets of pus (abscesses) in or a tear (perforation) in the gallbladder. Abscesses result from gangrene, which develops when tissue dies. A large stone may tear the gallbladder's wall and pass into the small intestine and block it. This blockage may cause abdominal pain and bloating.
If people develop jaundice or pass dark urine and light-colored stools, the common bile duct is probably blocked by a stone, causing a backup of bile in the liver (cholestasis).
Inflammation of the pancreas (pancreatitis) can develop. It is caused by a stone blocking the ampulla of Vater (where the common bile duct and the pancreatic duct join together).
Acalculous cholecystitis
Acalculous cholecystitis (cholecystitis without gallstones) typically causes sudden, excruciating pain in the upper abdomen in people with no previous symptoms or other evidence of a gallbladder disorder (see Biliary Pain Without Gallstones). The inflammation is often very severe and can lead to gangrene or rupture of the gallbladder.
People who develop acalculous cholecystitis tend to be very ill. For example, they may be in the intensive care unit for another reason and have many other symptoms. Also, because these people are so ill, they may not be able to communicate very clearly. For these reasons, acalculous cholecystitis may be overlooked at first.
The only symptoms may be a swollen (distended), tender abdomen or a fever with no known cause.
Chronic cholecystitis
People with chronic cholecystitis have recurring attacks of pain. The upper abdomen above the gallbladder is tender to the touch. In contrast to acute cholecystitis, fever rarely occurs in people with chronic cholecystitis. The pain is less severe than the pain of acute cholecystitis and does not last as long.
Diagnosis of Cholecystitis
Ultrasound and sometimes other imaging tests
Doctors diagnose cholecystitis based mainly on symptoms and results of imaging tests.
Ultrasound is the best way to detect gallstones in the gallbladder. Ultrasound can also detect fluid around the gallbladder or thickening of its wall, which are typical of acute cholecystitis. Often, when the ultrasound probe is moved across the upper abdomen above the gallbladder, people report tenderness.
Cholescintigraphy, another imaging test, is useful when acute cholecystitis is difficult to diagnose. For this test, a radioactive substance (radionuclide) is injected intravenously. A gamma camera detects the radioactivity given off, and a computer is used to produce an image. Thus, movement of the radionuclide from the liver through the biliary tract can be followed. Images of the liver, bile ducts, gallbladder, and upper part of the small intestine are taken. If the radionuclide does not fill the gallbladder, the cystic duct is probably blocked by a gallstone. Cholescintigraphy is also useful when doctors suspect acute acalculous cholecystitis.
CT or MRI scans may also help confirm the diagnosis when other tests are not conclusive.
Liver tests (blood tests) are done to evaluate how well the liver is functioning and whether it is damaged. However, these tests cannot confirm the diagnosis because results are often normal or only slightly high, unless the bile duct is blocked.
Other blood tests are also done. For example, the number (count) of white blood cells is measured. A high white blood cell count suggests inflammation, an abscess, gangrene, or a perforated gallbladder.
Computed tomography (CT) of the abdomen can detect some complications of cholecystitis, such as pancreatitis or a tear in the gallbladder.
Treatment of Cholecystitis
Intravenous fluids and antibiotics
Surgery to remove gallbladder (cholecystectomy)
Hospitalization
People with acute or chronic cholecystitis need to be hospitalized. They are not allowed to eat or drink and are given fluids and electrolytes intravenously. A doctor may pass a tube through the nose and into the stomach, so that suctioning can be used to keep the stomach empty and reduce fluid accumulating in the intestine if the intestine is blocked and to allow the gallbladder to rest.
Usually, people are given antibiotics intravenously (because infection is possible) and pain relievers.
Cholecystectomy
Surgical removal of the gallbladder (cholecystectomy) is usually done using a rigid tube called a laparoscope. After small incisions are made in the abdomen, the laparoscope and surgical instruments are inserted through the incisions. Doctors then use the instruments to remove the gallbladder. The laparoscope contains a tiny camera, which enables surgeons to see what they are doing inside the body.
The gallbladder is usually removed within 24 to 48 hours after symptoms start if:
Acute cholecystitis is confirmed and the risk of surgery is small.
People are older or have diabetes because in such people, cholecystitis is more likely to result in infections.
A complication such as an abscess, gangrene, or perforated gallbladder is suspected.
The gallstones caused pancreatitis
Surgery is being performed for acalculous cholecystitis
If necessary, surgery can be delayed for 6 weeks or more while the attack subsides. If people have a disorder that makes surgery too risky (such as a serious heart, lung, kidney, or liver disorder), surgery is delayed until appropriate treatment can control the disorder as well as possible.
If surgery needs to be delayed or avoided completely, the gallbladder may need to be drained to help treat and prevent spread of the infection. Drainage can be done by placing a tube through the abdominal wall into the gallbladder, allowing fluid to drain outside the body. Alternatively, a drainage tube can be placed from inside the body during endoscopy guided by endoscopic ultrasound (EUS). In EUS, an endoscope that contains a tiny ultrasound device at its tip is passed through the mouth into the stomach and the small intestine. The ultrasound images guide the doctor to place a drain between the gallbladder and the small intestine or between the gallbladder and the stomach.
In chronic cholecystitis, the gallbladder is sometimes removed after the current attack subsides, although a conservative (non-surgical) treatment approach can also be used.
Pain after surgery
Some people have new or recurring episodes of pain that feel like gallbladder attacks even though the gallbladder (and the stones) have been removed. Diarrhea can also develop. Doctors sometimes call this postcholecystectomy syndrome. The cause of this syndrome is not known, but in a few people, it may be malfunction of the sphincter of Oddi (a ring-shaped muscle between the common bile and pancreatic ducts and the small intestine). Malfunction of this muscle can slow the flow of bile and pancreatic secretions from the ducts and thus increase pressure in the ducts, causing pain. Pain may also result from small gallstones that remain in the ducts after the gallbladder is removed. More commonly, the cause is another, unrelated problem, such as irritable bowel syndrome or peptic ulcer disease that existed before the surgery.
Endoscopic retrograde cholangiopancreatography (ERCP) or cholescintigraphy (see Imaging Tests of the Liver and Gallbladder) may be necessary to determine whether the cause of pain is increased pressure in the bile ducts. For ERCP, a viewing tube (endoscope) is inserted through the mouth and into the intestine, and a device to measure pressure is inserted through the tube. If pressure is increased, surgical instruments are inserted through the tube and used to cut and thus widen the sphincter of Oddi. This procedure (called endoscopic sphincterotomy) can relieve symptoms when the pain is caused by malfunction of the sphincter.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
International Foundation for Gastrointestinal Disorders (IFFGD): A resource that helps people with gastrointestinal disorders manage their health.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): Comprehensive information on how the digestive system works and links to related topics, such as research and treatment options.





