

Neurogenic bladder is bladder dysfunction (flaccid or spastic) caused by neurologic damage. Symptoms can include overflow incontinence, frequency, urgency, urge incontinence, and retention. Risk of serious complications (eg, recurrent infection, vesicoureteral reflux, autonomic dysreflexia) is high. Diagnosis involves imaging and cystoscopy or urodynamic testing. Treatment involves catheterization or measures to trigger urination.
Any condition that impairs bladder and bladder outlet afferent and efferent signaling can cause neurogenic bladder. Causes may involve the central nervous system (eg, stroke, spinal injury, meningomyelocele, amyotrophic lateral sclerosis), peripheral nerves (eg, neuropathy caused by diabetes, alcohol use disorder, or vitamin B12 deficiency ; herniated discs; damage due to pelvic surgery), or both (eg, Parkinson disease, multiple sclerosis, syphilis). Bladder outlet obstruction (eg, due to benign prostatic hyperplasia, prostate cancer, fecal impaction, or urethral strictures) often coexists and may exacerbate symptoms. (See also Overview of Voiding.)
In flaccid (hypotonic) neurogenic bladder, the bladder volume is large, pressure is low, and contractions are absent. It may result from peripheral nerve damage or spinal cord damage at the S2 to S4 level. After acute cord damage, initial flaccidity may be followed by long-term flaccidity or spasticity, or bladder function may improve after days, weeks, or months.
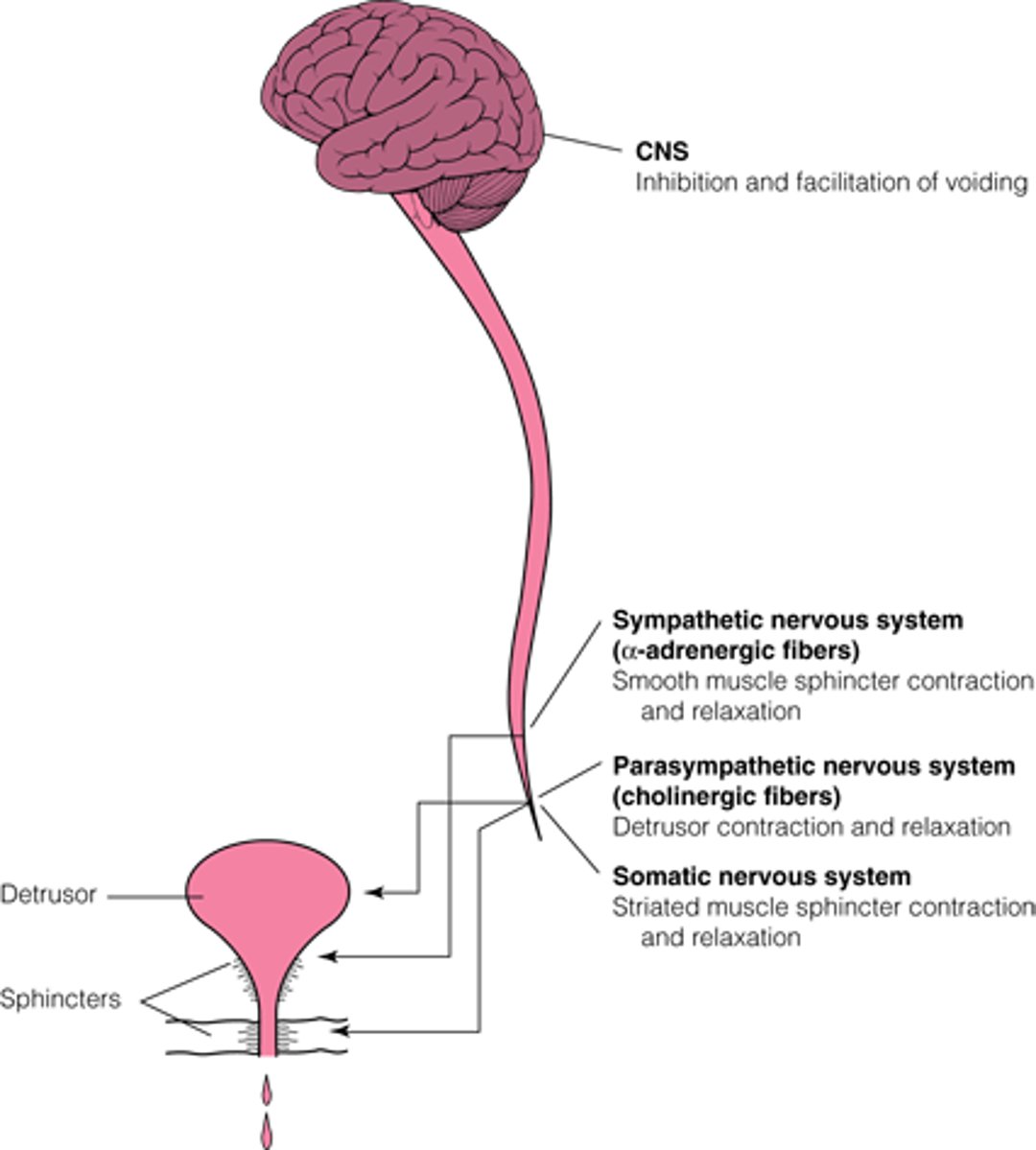
Normal Micturition: Coordinated Bladder Contraction and Urethral Sphincter Relaxation
The CNS inhibits voiding until the appropriate time and coordinates and facilitates input from the lower urinary tract to start and complete voiding. The sympathetic system contracts the smooth muscle sphincter. The parasympathetic nervous system contracts the bladder detrusor muscle through cholinergic fibers. The somatic nervous system contracts the striated muscle sphincter through cholinergic fibers from the pudendal nerve. (Adapted from DuBeau CE, Resnick NM with the Massachusetts Department of Health EDUCATE project collaborators: Urinary Incontinence in the Older Adult: An Annotated Speaker/Teacher Kit, 1993; used with permission of the authors.) |

In spastic bladder, the bladder volume is typically normal or small, and involuntary contractions occur. It usually results from brain damage or spinal cord damage above T12. Precise symptoms vary by site and severity of the lesion. Bladder contraction and external urinary sphincter relaxation are typically uncoordinated (detrusor-sphincter dyssynergia).
Mixed patterns (flaccid and spastic bladder) may be caused by many disorders, including syphilis, diabetes mellitus, brain or spinal cord tumors, stroke, ruptured intervertebral disc, and demyelinating or degenerative disorders (eg, multiple sclerosis, amyotrophic lateral sclerosis).
Symptoms and Signs of Neurogenic Bladder
Overflow incontinence is the primary symptom in patients with a flaccid bladder. Patients retain urine and have constant overflow dribbling. Men typically also have erectile dysfunction, and anorgasmia is common in women with spinal cord injury.
Patients with spastic bladder may have frequency, nocturia, and spastic paralysis with sensory deficits; most have intermittent bladder contractions causing urine leakage and, unless they lack sensation, urgency. In patients with detrusor-sphincter dyssynergia, sphincter spasm during voiding may prevent complete bladder emptying.
Common complications include recurrent urinary tract infections and urinary calculi. Hydronephrosis with vesicoureteral reflux may occur because the large urine volume puts pressure on the vesicoureteral junction, causing dysfunction with reflux and, in severe cases, nephropathy. Patients with high thoracic or cervical spinal cord lesions are at risk of autonomic dysreflexia (a life-threatening syndrome of malignant hypertension, bradycardia or tachycardia, headache, piloerection, and sweating due to unregulated sympathetic hyperactivity). Autonomic dysreflexia in such patients may be triggered by acute bladder distention (due to urinary retention) or bowel distention (due to constipation or fecal impaction).
Diagnosis of Neurogenic Bladder
Postvoid residual volume
Renal ultrasound
Serum creatinine
Usually cystography, cystoscopy, and cystometrography with urodynamic testing
Diagnosis is suspected based on clinical presentation. Usually, postvoid residual volume is measured, renal ultrasound is done to detect hydronephrosis, and serum creatinine is measured to assess kidney function.
In patients with hydronephrosis or nephropathy who are not severely debilitated, cystography, cystoscopy, and cystometrography with urodynamic testing are usually recommended and may guide further therapy. These studies may not be indicated in severely debilitated patients who are not able to self-catheterize or cannot recognize the need to urinate.
Cystography is used to evaluate bladder capacity and detect ureteral reflux.
Cystoscopy is used to evaluate duration and severity of retention (by detecting the degree of bladder trabeculations) and to check for bladder outlet obstruction.
Cystometrography can determine whether bladder volume and pressure are high or low; if done during the recovery phase of flaccid bladder after spinal cord injury, it can help evaluate detrusor functional capacity and predict rehabilitation prospects.
Urodynamic testing of voiding flow rates with sphincter electromyography can show whether bladder contraction and sphincter relaxation are coordinated.
Treatment of Neurogenic Bladder
Catheterization
Increased fluid intake
Medication
Surgery if conservative measures fail
Specific treatment involves catheterization or measures to trigger urination. Intermittent catheterization is preferred to continuous catheterization whenever possible. General treatment includes renal function monitoring, control of urinary tract infections (UTIs), high fluid intake to decrease risk of UTIs and urinary calculi (although this measure may exacerbate incontinence), early ambulation, frequent changes of position, and dietary calcium restriction to inhibit calculus formation.
The prognosis for preserving renal function is generally favorable with early and appropriate management.
Catheterization
For flaccid bladder, especially if the cause is an acute spinal cord injury, immediate continuous or intermittent catheterization is needed. Intermittent self-catheterization is preferable to indwelling urethral catheterization, which has a high risk of recurrent UTIs and, in men, a high risk of urethritis, periurethritis, prostatic abscesses, and urethral fistulas. Suprapubic catheterization may be used if patients cannot self-catheterize.

Medications and other therapies
For spastic bladder, treatment depends on the patient’s ability to retain urine. Patients who can retain normal volumes can use techniques to trigger voiding (eg, applying suprapubic pressure, scratching the thighs); anticholinergics may be effective. For patients who cannot retain normal volumes, treatment is the same as that for urge incontinence, including medications (see table ) and sacral nerve stimulation.
Surgery
Surgery is a last resort. It is usually indicated if patients have had, or are at risk of, severe acute or chronic sequelae (eg, renal deterioration, recurrent urinary infections, calculi) or if social circumstances, spasticity, or quadriplegia prevents use of continuous or intermittent bladder drainage. Sphincterotomy (for men) converts the bladder into an open draining conduit. Sacral (S3 and S4) rhizotomy converts a spastic into a flaccid bladder. Urinary diversion may involve an ileal conduit or ureterostomy.
An artificial, mechanically controlled urinary sphincter, surgically inserted, is an option for patients who have adequate bladder capacity, good bladder emptying, and upper extremity motor skills and who can comply with instructions for use of the device; if patients do not comply, life-threatening situations (eg, chronic kidney disease, urosepsis) can result.
Key Points
Damage to the neural pathways that control voiding can render the bladder too flaccid or spastic.
Flaccid bladder tends to cause overflow incontinence.
Spastic bladder tends to cause frequency, urge incontinence and, particularly with detrusor-sphincter dyssynergia, retention.
Measure postvoid residual volume, do renal ultrasound and serum creatinine measurement, and in many patients, do cystography, cystoscopy, and cystometrography with urodynamic testing.
Treatment for flaccid bladder includes increased fluid intake and intermittent self-catheterization.
Treatment for spastic bladder may include measures to trigger urination and/or measures used to treat urge incontinence (including medications).





