


Assisted reproductive techniques (ARTs) involve manipulation of sperm and ova or embryos in vitro with the goal of producing a pregnancy.
For assisted reproductive techniques, oocytes and sperm are collected from the intended parents or donors, and an embryo or the gametes are transferred to the woman's reproductive tract after culture in vitro.
ARTs may result in multifetal pregnancy, but risk is much less than that with controlled ovarian stimulation. If risk of genetic defects is high, the embryo can often be tested for defects before transfer and implantation (preimplantation genetic testing).
Еекстракорпоральне запліднення (ЕКЗ)
IVF can be used to treat infertility due to oligospermia, sperm antibodies, tubal dysfunction, or endometriosis as well as unexplained infertility.
The procedure typically involves the following:
Controlled ovarian stimulation: Clomiphene plus gonadotropins or gonadotropins alone can be used. A gonadotropin-releasing hormone (GnRH) agonist or antagonist is often given to prevent premature ovulation. After sufficient follicular growth, human chorionic gonadotropin (hCG) is given to trigger final follicular maturation and ovulation. Alternatively, a GnRH agonist can be used to trigger ovulation in women at high risk of ovarian hyperstimulation syndrome.
Oocyte retrieval: About 34 hours after hCG is given, oocytes are retrieved by direct needle puncture of the follicle, usually transvaginally with ultrasound guidance or less commonly laparoscopically. At some centers, natural cycle IVF (in which a single oocyte is retrieved) is offered as an alternative; pregnancy rates with this technique are lower than those with retrieval of multiple oocytes, but costs are lower and success rates are increasing.
Fertilization: The oocytes are inseminated in vitro. The semen sample is typically washed several times with tissue culture medium and is concentrated for motile sperm, which are then added to the medium containing the oocytes. At this point, intracytoplasmic sperm injection—injection of a single sperm into each oocyte—may be done, particularly if spermatogenesis is abnormal in the male partner.
Embryo culture: After sperm are added, the oocytes are cultured for about 2 to 5 days.
Embryo transfer: Only 1 or a few of the resulting embryos are transferred to the uterine cavity, minimizing the chance of a multifetal pregnancy, the greatest risk of IVF. The number of embryos transferred is determined by the woman’s age and likelihood of response to IVF. Some or all embryos (especially if women are at high risk of ovarian hyperstimulation syndrome) may be frozen in liquid nitrogen for transfer in a subsequent cycle. There is an increasing tendency to place only one embryo at each transfer and to freeze the remaining embryos for use in subsequent cycles if pregnancy does not result.
Birth defects may be slightly more common after IVF, but experts are uncertain whether the increased risk is due to IVF or to factors contributing to infertility; infertility itself increases risk of birth defects. Still, as of early 2018, the overwhelming majority of the > 7 million children born after IVF have no birth defects (1, 2). Worldwide, an estimated 200,000 babies are born after IVF every year.
Preimplantation genetic testing can be done using cells from the polar body of an oocyte or cells from an embryo (either a blastomere from a 3-day-old embryo or trophectoderm cells from a 5- or 6-day-old embryo). Testing may involve preimplantation genetic screening to rule out aneuploidy and/or preimplantation genetic diagnosis to check for specific serious hereditary disorders. If test results are delayed, the blastocyst can be frozen and transferred in a later cycle after the results are known.
Preliminary data for 2020 indicate that in the US, the cumulative chances of a live birth for each oocyte retrieval (counting all transfers of the patient's own embryos—both fresh and frozen-thawed) was 44.6% for women < 35 (6.6% were twins; 0.2% were triplets or more) and 9.7% for women aged 41 to 42 (3).
Use of donor oocytes is usually recommended for women > 42.
Перенесення гамет в маткову трубу (GIFT)
GIFT is an alternative to IVF but is rarely used because success rates for IVF have increased.
GIFT is used most often when women have one of the following:
Unexplained infertility
Normal tubal function plus endometriosis
Multiple oocytes and sperm are obtained as for IVF but are transferred—transvaginally with ultrasound guidance or laparoscopically—to the distal fallopian tubes, where fertilization occurs.
Live birth rates per cycle are about 25 to 35%.
Інтрацитоплазматична ін'єкція сперматозоїда (ICSI)
This technique is useful when
Other techniques are unsuccessful or are likely to be so.
A severe sperm disorder is present.
Oocytes are obtained as for IVF. A single sperm is injected into each oocyte to avoid fertilization by abnormal sperm. The embryo is then cultured and transferred as for IVF.
Intracytoplasmic sperm injection is involved in about two thirds of ART cycles in the US. There is no benefit to using intracytoplasmic sperm injection in couples with low oocyte yield or advanced maternal age. If a couple's infertility involves the woman, > 30 of these procedures must be done to make one additional pregnancy likely. Thus, the additional costs and risks of intracytoplasmic sperm injection must be considered when deciding whether to use it.

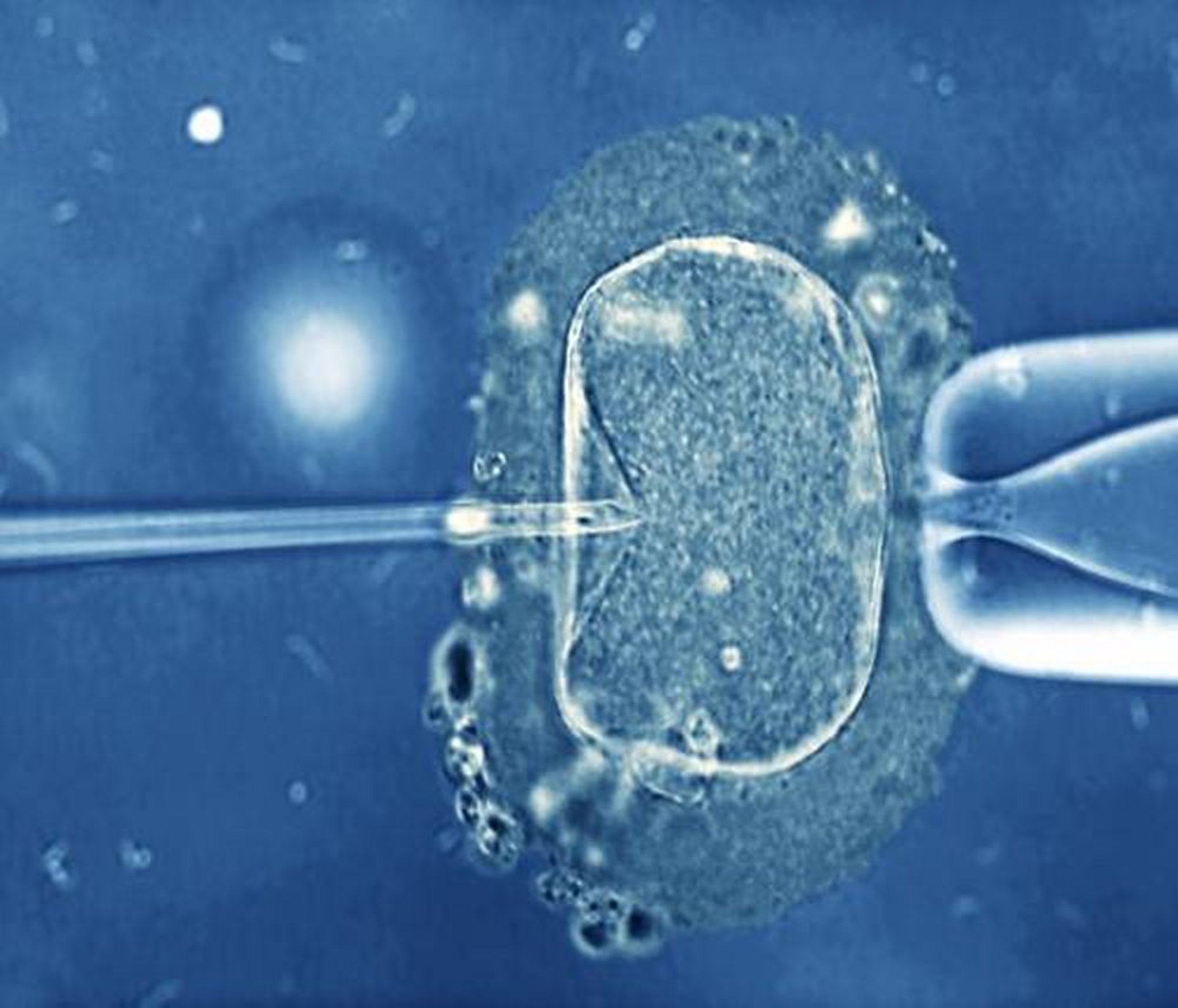
ZEPHYR/SCIENCE PHOTO LIBRARY
Risk of birth defects may be increased after intracytoplasmic sperm injection, possibly because of the following:
The procedure itself can damage the sperm, egg, or embryo.
Sperm from men who have mutations of the Y chromosome may be used. Most reported birth defects involve the male reproductive tract.
Інші техніки
Other techniques are sometimes used. They include the following:
A combination of IVF and GIFT
Zygote intrafallopian tube transfer (rarely used)
Use of donor oocytes or embryos
Transfer of frozen embryos to a gestational carrier
For postmenopausal women who are > 50 years and have an older male partner (usually defined as ≥ 45 years), use of IVF is controversial.
Довідкові матеріали загального характеру
1. Berntsen S, Söderström-Anttila V, Ulla-Britt Wennerholm U-B, et al: The health of children conceived by ART: 'the chicken or the egg?' Hum Reprod Update 25 (2):137–158, 2019. doi: 10.1093/humupd/dmz001
2. Zhao J, Yan Y, Huang X, Li Y: Do the children born after assisted reproductive technology have an increased risk of birth defects? A systematic review and meta-analysis. J Matern Fetal Neonatal Med 33 (2):322–333, 2020. doi: 10.1080/14767058.2018.1488168
3. Society for Assisted Reproductive Technology: Preliminary national summary report for 2020. Accessed 8/9/22.