

Squamous cell carcinoma is a malignant tumor of epidermal keratinocytes that invades the dermis; this cancer usually occurs in sun-exposed areas. Local destruction may be extensive, and metastases occur in advanced stages. Diagnosis is by biopsy. Treatment depends on the tumor’s characteristics and may involve curettage and electrodesiccation, surgical excision, cryosurgery, or, occasionally, radiation therapy.
(See also Overview of Skin Cancer.)
Squamous cell carcinoma is a keratinocyte skin cancer and the second most common type of skin cancer after basal cell carcinoma, with 1.8 million cases annually in the United States (1). It may develop in normal tissue, in a preexisting actinic keratosis, in a patch of oral leukoplakia, or in a burn scar. Squamous cell carcinoma is more common in men (1), and risks increase dramatically with age (2) (particularly in patients older than 75).
The pathophysiology of squamous cell carcinoma is similar to that of the pathophysiology of basal cell carcinoma and involves the interplay between combinations of environmental and genetic factors (3). People with lightly pigmented skin are much more susceptible to squamous cell carcinoma than people with darkly pigmented skin, as are people with chronic immunosuppression. Some key differentiating factors include stronger associations with cumulative UV damage (4) and mutations in key tumor suppressor genes such as TP53 in squamous cell carcinoma (compared to the Hedgehog pathway in basal cell carcinoma) (5). Less commonly, other signaling pathways may also be implicated (eg, EGFR, RAS, Fyn, p16, NOTCH1, NOTCH2, PI3K) (6). Squamous cell carcinomas are also more aggressive and likely to metastasize than basal cell carcinomas, which are instead characterized by local invasion but low likelihood of metastatic spread. Squamous cell carcinoma is also more likely to develop on skin damaged by chronic irritation or injury.
References
1. The Skin Cancer Foundation. Skin Cancer Facts & Statistics: Nonmelanoma skin cancer. Accessed November 5, 2025.
2. Wysong A. Squamous-Cell Carcinoma of the Skin. N Engl J Med. 2023 Jun 15;388(24):2262-2273. doi: 10.1056/NEJMra2206348. PMID: 37314707.
3. Skin Cancer Foundation. Squamous Cell Carcinoma Risk Factors. Accessed October 29, 2025.
4. Firnhaber JM. Basal Cell and Cutaneous Squamous Cell Carcinomas: Diagnosis and Treatment. Am Fam Physician. 2020 Sep 15;102(6):339-346. PMID: 32931212.
5. Piipponen M, Riihilä P, Nissinen L, Kähäri VM. The Role of p53 in Progression of Cutaneous Squamous Cell Carcinoma. Cancers (Basel). 2021;13(18):4507. Published 2021 Sep 7. doi:10.3390/cancers13184507
6. Boeckmann L, Martens MC, Emmert S. Molecular Biology of Basal and Squamous Cell Carcinomas. Adv Exp Med Biol. 2020;1268:171-191. doi: 10.1007/978-3-030-46227-7_9. PMID: 32918219.
Symptoms and Signs of Squamous Cell Carcinoma
The clinical appearance is highly variable, but any nonhealing lesion on a sun-exposed surface should raise clinical suspicion for a keratinocyte cancer. The tumor may begin as a red papule or plaque with a scaly or crusted surface and may become nodular or hyperkeratotic, sometimes with a warty surface. In some cases, the bulk of the lesion may lie below the level of the surrounding skin. Eventually, the tumor can ulcerate and invade the underlying tissue.
Lesions in the head, neck, hands, feet or anogenital regions are considered high-risk (ie, elevated risk of recurrence and metastasis) (1).

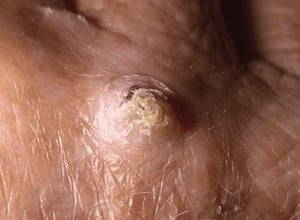
This photo shows a hyperkeratotic skin-colored nodule arising on a sun-exposed area consistent with cutaneous squamous cell carcinoma.
This photo shows a hyperkeratotic skin-colored nodule arising on a sun-exposed area consistent with cutaneous squamous
Photo provided by Thomas Habif, MD.


This erythematous, irregular plaque on an extremity was diagnosed as squamous cell carcinoma on biopsy.
This erythematous, irregular plaque on an extremity was diagnosed as squamous cell carcinoma on biopsy.
© Springer Science+Business Media


The appearance of squamous cell carcinoma is variable. These hyperpigmented, scaly lesions on the earlobe were diagnosed as squamous cell carcinoma on biopsy.
The appearance of squamous cell carcinoma is variable. These hyperpigmented, scaly lesions on the earlobe were diagnose
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


This squamous cell carcinoma on the lip is highly keratinized; not all squamous cell carcinomas of the lip are as highly keratinized.
This squamous cell carcinoma on the lip is highly keratinized; not all squamous cell carcinomas of the lip are as highl
Photo courtesy of Gregory L. Wells, MD.


This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to other parts of the body.
This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to o
DR M.A. ANSARY / SCIENCE PHOTO LIBRARY


This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to other parts of the body.
This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to o
DR M.A. ANSARY / SCIENCE PHOTO LIBRARY
This photo shows a hyperkeratotic skin-colored nodule arising on a sun-exposed area consistent with cutaneous squamous cell carcinoma.
This photo shows a hyperkeratotic skin-colored nodule arising on a sun-exposed area consistent with cutaneous squamous
Photo provided by Thomas Habif, MD.
This erythematous, irregular plaque on an extremity was diagnosed as squamous cell carcinoma on biopsy.
This erythematous, irregular plaque on an extremity was diagnosed as squamous cell carcinoma on biopsy.
© Springer Science+Business Media
The appearance of squamous cell carcinoma is variable. These hyperpigmented, scaly lesions on the earlobe were diagnosed as squamous cell carcinoma on biopsy.
The appearance of squamous cell carcinoma is variable. These hyperpigmented, scaly lesions on the earlobe were diagnose
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
This squamous cell carcinoma on the lip is highly keratinized; not all squamous cell carcinomas of the lip are as highly keratinized.
This squamous cell carcinoma on the lip is highly keratinized; not all squamous cell carcinomas of the lip are as highl
Photo courtesy of Gregory L. Wells, MD.
This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to other parts of the body.
This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to o
DR M.A. ANSARY / SCIENCE PHOTO LIBRARY
This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to other parts of the body.
This photo shows squamous cell carcinoma manifesting as a large, ulcer-like area that, in its later stages, spread to o
DR M.A. ANSARY / SCIENCE PHOTO LIBRARY
Symptoms and signs reference
1. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Squamous Cell Skin Cancer, version 1.2026. https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Accessed November 13, 2025.
Diagnosis of Squamous Cell Carcinoma
Biopsy
The diagnosis of squamous cell carcinoma consists of clinical evaluation of a suspicious skin lesion followed by confirmation with biopsy and histologic examination. Biopsy, which should extend into the dermis, is essential (1).
Due to the likelihood of metastatic spread, regional lymph node exams and imaging studies of the area of involvement may be required in some cases.
Differential diagnosis
The differential diagnosis varies based on the lesion's appearance.
Nonhealing ulcers should be differentiated from pyoderma gangrenosum and venous stasis ulcers.
Nodular and hyperkeratotic lesions should be differentiated from keratoacanthomas (probably squamous cell carcinomas themselves) and verruca vulgaris.
Scaling plaques should be differentiated from basal cell carcinoma, actinic keratosis, verruca vulgaris, seborrheic keratosis, psoriasis, and nummular dermatitis (discoid dermatitis).
Diagnosis reference
1. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Squamous Cell Skin Cancer, version 1.2026. https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Accessed November 13, 2025.
Treatment of Squamous Cell Carcinoma
Usually locally destructive techniques
The treatment of squamous cell carcinoma is similar to that for basal cell carcinoma and includes curettage and electrodesiccation, surgical excision, cryosurgery, topical chemotherapy (imiquimod or 5-fluorouracil) and photodynamic therapy, or, occasionally, radiation therapy (and includes curettage and electrodesiccation, surgical excision, cryosurgery, topical chemotherapy (imiquimod or 5-fluorouracil) and photodynamic therapy, or, occasionally, radiation therapy (1). Treatment and follow-up must be monitored closely because squamous cell carcinoma has a greater risk of metastasis compared with basal cell carcinoma.
Squamous cell carcinoma on the lip or other mucocutaneous junction should be excised; at times, cure is difficult.
Surgical excision relies on standard excision with 4 to 6 mm clear margins for low-risk lesions and progressive excision with wider surgical margins for high-risk lesions. Mohs micrographic surgery may also be performed and is preferred for high-risk lesions. Radiation therapy can be provided as an adjunct to surgery or for nonsurgical candidates (ie, patients with positive margins, recurrent disease, or extensive perineural invasion) (1). Recurrences and large tumors should be treated aggressively with Mohs micrographic surgery.
Metastatic disease is responsive to radiation therapy if metastases can be identified and are isolated. Widespread metastases do not respond well to conventional chemotherapeutic regimens. Cetuximab (an EGFR-blocking monoclonal antibody) has been moderately effective when co-administered with surgery or radiation (Metastatic disease is responsive to radiation therapy if metastases can be identified and are isolated. Widespread metastases do not respond well to conventional chemotherapeutic regimens. Cetuximab (an EGFR-blocking monoclonal antibody) has been moderately effective when co-administered with surgery or radiation (2). Programmed death receptor 1 (PD-1) inhibitors (eg, cemiplimab, pembrolizumab) are reserved for patients with inoperable, advanced, or metastatic disease (). Programmed death receptor 1 (PD-1) inhibitors (eg, cemiplimab, pembrolizumab) are reserved for patients with inoperable, advanced, or metastatic disease (3, 4).
Treatment references
1. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Squamous Cell Skin Cancer, version 1.2026. https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Accessed November 13, 2025.
2. Trodello C, Higgins S, Ahadiat O, et al. Cetuximab as a Component of Multimodality Treatment of High-Risk Cutaneous Squamous Cell Carcinoma: A Retrospective Analysis From a Single Tertiary Academic Medical Center. . Cetuximab as a Component of Multimodality Treatment of High-Risk Cutaneous Squamous Cell Carcinoma: A Retrospective Analysis From a Single Tertiary Academic Medical Center.Dermatol Surg.2019 Feb;45(2):254-267. doi: 10.1097/DSS.0000000000001755. PMID: 30672860.
3. Rischin D, Porceddu S, Day F, et al. C-POST Trial Investigators. Adjuvant Cemiplimab or Placebo in High-Risk Cutaneous Squamous-Cell Carcinoma. N Engl J Med. 2025 Aug 21;393(8):774-785. doi: 10.1056/NEJMoa2502449.
4. Hughes BGM, Munoz-Couselo E, Mortier L, et al. Pembrolizumab for locally advanced and recurrent/metastatic cutaneous squamous cell carcinoma (KEYNOTE-629 study): an open-label, nonrandomized, multicenter, phase II trial. Ann Oncol. 2021 Oct;32(10):1276-1285. doi: 10.1016/j.annonc.2021.07.008. Epub 2021 Jul 20. Erratum in: Ann Oncol. 2022 Aug;33(8):853. doi: 10.1016/j.annonc.2022.05.517. PMID: 34293460.
Prognosis for Squamous Cell Carcinoma
In general, the prognosis for small lesions removed early and adequately is excellent. The 5-year survival rate for cutaneous forms of squamous cell carcinoma is approximately 98% for the general population; however, the rate is significantly lower in patients with high-risk features or more invasive or metastatic disease (1). Regional and distant metastases of squamous cell carcinomas on sun-exposed skin are uncommon but do occur, particularly with poorly differentiated tumors. Characteristics of more aggressive tumors include:
Size > 2 cm in diameter
Invasion depth of > 2 mm
Perineural invasion
Location near the ear or vermilion border
Late-stage disease, which may require extensive surgery, is far more likely to metastasize. It spreads initially regionally to surrounding skin and lymph nodes and eventually to nearby organs. Cancers that occur near the ears or the vermilion border, in scars, or that have perineural invasion are more likely to metastasize. In one longitudinal retrospective cohort study, cutaneous squamous cell carcinoma carried a 3.7% risk of metastasis and 2.1% risk of disease-specific death over a 10 year-period (2).
Prognosis references
1. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Squamous Cell Skin Cancer, version 1.2026. https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf. Accessed November 13, 2025.
2. Schmults CD, Karia PS, Carter JB, et al. Factors predictive of recurrence and death from cutaneous squamous cell carcinoma: a 10-year, single-institution cohort study. JAMA Dermatol. 2013 May;149(5):541-7. doi: 10.1001/jamadermatol.2013.2139. PMID: 23677079.
Prevention of Squamous Cell Carcinoma
Because squamous cell carcinoma is associated with ultraviolet (UV) radiation exposure, a number of measures are recommended to limit exposure (eg, sun avoidance measures, use of protective clothing, use of sunscreen). For more detailed information, see Prevention of Effects of Sun Exposure.
Key Points
Because of its high frequency of occurrence and highly variable appearance, squamous cell carcinoma should be considered in any nonhealing lesion in a sun-exposed area.
Metastases are uncommon but are more likely in cancers involving the lingual or mucosal surfaces; that occur near the ears, the vermilion border, or in scars; or that have perineural invasion.
Treatment is usually with locally destructive methods, sometimes also with radiation therapy (eg, for tumors that are large, recurrent, or have perineural invasion).
PD-1 inhibitors such as cemiplimab and pembrolizumab or EGFR inhibitors such as cetuximab may be useful in patients with advanced or metastatic disease.PD-1 inhibitors such as cemiplimab and pembrolizumab or EGFR inhibitors such as cetuximab may be useful in patients with advanced or metastatic disease.





