



Toxoplasmosis is infection with Toxoplasma gondii. Symptoms range from none to benign lymphadenopathy, a mononucleosis-like illness, to life-threatening central nervous system disease or involvement of other organs in immunocompromised people. Encephalitis can develop in patients with advanced HIV infection and low CD4 counts. Retinochoroiditis, seizures, and intellectual disability occur in congenital infection. Diagnosis is made by serologic tests, histopathology, or polymerase chain reaction tests. Treatment is most often with pyrimethamine plus either sulfadiazine or clindamycin. Corticosteroids are given concurrently for retinochoroiditis.
Human exposure to toxoplasmosis is common wherever cats are found.
A study in 2010 found that 12.4% of people ≥ 6 years in the United States were seropositive (1), which indicated they had been infected. In Europe, the seroprevalence range is 30 to 50%, and in South America, seroprevalence ranges from 30 to 80% (2).
The risk of developing serious disease is very low except for a fetus infected in utero and people who are or become severely immunocompromised due to advanced HIV infection or other diseases. Other factors that may contribute include lack of access to safe drinking water, inadequate sanitation, and poor hygiene (3).
General references
1. Jones JL, Kruszon-Moran D, Rivera HN, Price C, Wilkins PP. Toxoplasma gondii seroprevalence in the United States 2009-2010 and comparison with the past two decades. Am J Trop Med Hyg. 2014;90(6):1135-1139. doi:10.4269/ajtmh.14-0013
2. Molan A, Nosaka K, Hunter M, Wang W. Global status of Toxoplasma gondii infection: systematic review and prevalence snapshots. Trop Biomed. 2019;36(4):898-925.
3. World Health Organization (WHO): Toxoplasma gondii. Background document for the WHO Guidelines for drinking-water quality and the WHO Guidelines on sanitation and health. 2025.
Pathophysiology of Toxoplasmosis
T. gondii is ubiquitous in birds and mammals (see also Toxoplasmosis in Animals). This obligate intracellular parasite invades and multiplies asexually as tachyzoites within the cytoplasm of any nucleated cell. When host immunity develops, multiplication of tachyzoites ceases and tissue cysts form; cysts persist in a dormant state for years, especially in brain, eyes, and muscle. The dormant Toxoplasma forms within the cysts are called bradyzoites.
Sexual reproduction of T. gondii occurs only in the intestinal tract of cats; the resultant oocysts passed in the feces remain infectious in moist soil for months. The only known definitive hosts for T. gondii are members of family Felidae (domestic cats and their relatives).


1. Oocysts are shed in the cat’s feces. Large numbers are shed but usually only for 1–2 weeks. Oocysts take 1–5 days to sporulate and become infective. Cats become reinfected by ingesting sporulated oocysts.
2. Soil, water, plant material, or cat litter can become contaminated with oocysts. Intermediate hosts in nature (eg, birds, rodents, wild game, animals bred for human consumption) can also become infected after ingesting infective materials.
3. Oocysts develop into tachyzoites shortly after ingestion. Tachyzoites spread throughout the body and form tissue cysts in nerve, eye, and muscle tissue.
4. Cats become infected after consuming intermediate hosts containing tissue cysts. Cats may also become infected directly by ingestion of sporulated oocysts.
5. Animals bred for human consumption and wild game may also become infected with tissue cysts after ingestion of sporulated oocysts in the environment.
6. Humans can become infected by ingesting undercooked meat containing tissue cysts.
7. Humans can become infected by ingesting food or water contaminated with cat feces or other feces-contaminated materials (eg, soil) or contact with a pet cat’s litter.
8. Rarely, human infection results from blood transfusion or organ transplantation.
9. Rarely, transplacental transmission from mother to fetus occurs.
10. In the human host, parasites form tissue cysts, most commonly in skeletal muscle, cardiac muscle, the brain, and the eyes; these cysts may remain dormant throughout the life of the host and can reactivate if the host becomes immunocompromised.
11. Diagnosis of congenital toxoplasmosis can be made by detecting T. gondii DNA in amniotic fluid using molecular methods such as PCR.
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Infection can occur by:
Ingestion of oocysts
Ingestion of tissue cysts
Transplacental transmission
Blood transfusion or organ transplantation
Ingestion of oocysts in food or water contaminated with cat feces is the most common mode of oral infection. Infection can also occur by eating raw or undercooked meat containing tissue cysts, most commonly lamb and pork and rarely beef. Infection may also be contracted by eating raw or undercooked shellfish or, less commonly, other types of fish.
After the ingestion of oocysts or tissue cysts, tachyzoites are released and spread throughout the body. This acute infection is followed by the development of protective immune responses and the formation of tissue cysts in many organs. The cysts can reactivate, causing disease, primarily in immunocompromised patients. Toxoplasmosis reactivates in patients with advanced HIV infection who are not taking antibiotic prophylaxis, but the widespread use of trimethoprim/sulfamethoxazole for Pneumocystis prophylaxis has dramatically reduced the incidence (1).
Toxoplasmosis can be transmitted transplacentally if the mother becomes infected during pregnancy or if immunosuppression reactivates a prior infection. Transmission of Toxoplasma to a fetus is extraordinarily rare in immunocompetent pregnant patients who were infected with Toxoplasma and developed immunity prior to pregnancy.
Transmission may occur via transfusion of whole blood or white blood cells or via transplantation of an organ from a seropositive donor.
In otherwise healthy people, congenital or acquired infection can reactivate in the eyes. Nonocular reactivation is very rare in healthy people. Past infection typically confers resistance to reinfection. In immunocompromised patients, a reactivated infection is most likely to occur in the brain, but it may affect the eyes or disseminate.
Pathophysiology reference
1. Abgrall S, Rabaud C, Costagliola D; Clinical Epidemiology Group of the French Hospital Database on HIV. Incidence and risk factors for toxoplasmic encephalitis in human immunodeficiency virus-infected patients before and during the highly active antiretroviral therapy era. Clin Infect Dis. 2001;33(10):1747-1755. doi:10.1086/322622
Symptoms and Signs of Toxoplasmosis
Infections may manifest in several ways:
Acute toxoplasmosis
Central nervous system (CNS) toxoplasmosis
Congenital toxoplasmosis
Ocular toxoplasmosis
Disseminated or non-CNS disease in immunocompromised patients
Acute toxoplasmosis
Acute infection is usually asymptomatic, but 10 to 20% of patients develop bilateral, nontender cervical or axillary lymphadenopathy (1). A few of these patients also have a mild flu-like syndrome of fever, malaise, myalgia, hepatosplenomegaly, and, less commonly, pharyngitis, which can mimic infectious mononucleosis and include lymphadenitis. Atypical lymphocytosis, mild anemia, leukopenia, and slightly elevated liver enzymes are common.
The syndrome may persist for weeks but is almost always self-limited.
CNS toxoplasmosis
Most immunocompromised patients who develop toxoplasmosis present with encephalitis and ring-enhancing intracranial mass lesions seen on CT or MRI scans both with contrast.
Risk is greatest among patients with HIV infection who have a CD4 count < 50/mcL; toxoplasmic encephalitis is rare when CD4 counts are > 200/mcL. These patients typically have headache, altered mental status, seizures, coma, fever, and sometimes focal neurologic deficits, such as motor or sensory loss, cranial nerve palsies, visual abnormalities, and focal seizures.
Congenital toxoplasmosis
Congenital toxoplasmosis results from a primary, often asymptomatic infection acquired by the mother during pregnancy. Patients infected before conception ordinarily do not transmit toxoplasmosis to the fetus unless the infection is reactivated during pregnancy by immunosuppression.
The likelihood of vertical transmission to the fetus increases with gestational age, and risk of transmission is estimated to be at 2.2% at 6 weeks, 23% at 18 weeks, and 56% at 30 weeks of pregnancy (2).
Congenital infection may result in spontaneous abortion, stillbirth, or birth defects.
Disease in neonates may be severe, particularly if acquired early in pregnancy; symptoms include jaundice, rash, hepatosplenomegaly, and the characteristic tetrad of abnormalities:
Bilateral retinochoroiditis
Cerebral calcifications
Hydrocephalus or microcephaly
Psychomotor retardation
For infants born with severe disease, the prognosis is poor.
The severity of congenital disease decreases if the mother becomes infected later in pregnancy. Many children with less severe infections and most infants born to mothers infected during the third trimester appear healthy at birth but are at high risk of seizures, intellectual disability, retinochoroiditis, or other symptoms developing months or even years later.
Ocular toxoplasmosis
Ocular toxoplasmosis usually results from congenital infection that is reactivated, often during adolescence and the 20s, but, rarely, it occurs with acquired infections. Focal necrotizing retinitis and a secondary granulomatous inflammation of the choroid occur and may cause ocular pain, blurred vision, and sometimes blindness.
Relapses are common.

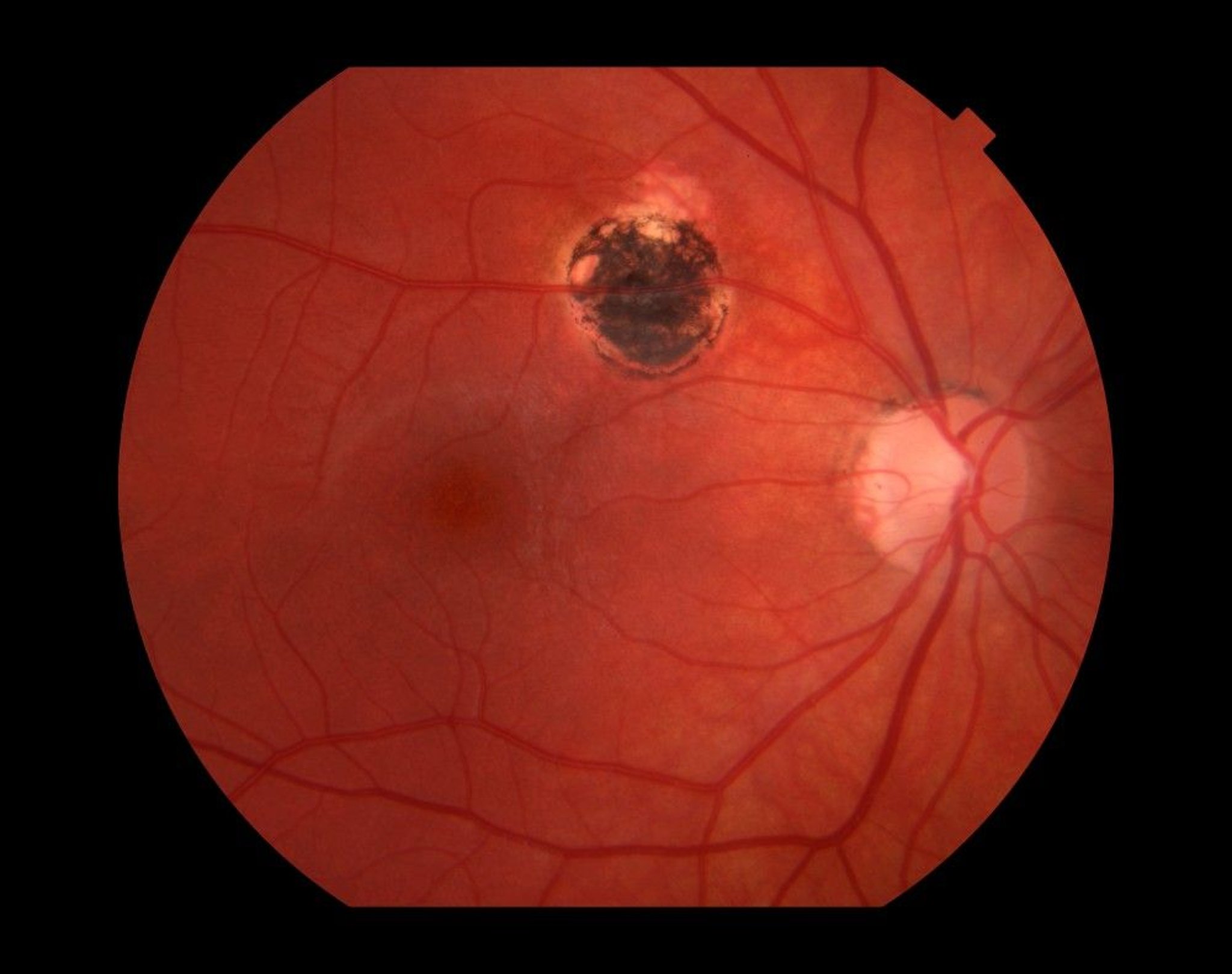
This image shows a retinal scar (upper center) caused by toxoplasmosis infection.
Paul Whitten/SCIENCE PHOTO LIBRARY
Disseminated infection and non-CNS involvement
Disease outside the eye and CNS is much less common and occurs primarily in severely immunocompromised patients. They may present with pneumonitis, myocarditis, polymyositis, diffuse maculopapular rash, high fevers, chills, and prostration.
In toxoplasmic pneumonitis, diffuse interstitial infiltrates may progress rapidly to consolidation and cause respiratory failure, whereas endarteritis may lead to infarction of small lung segments. Myocarditis, in which conduction defects are common but often asymptomatic, may rapidly lead to heart failure.
Untreated disseminated infections are usually fatal.
Symptoms and signs references
1. Centers for Disease Control and Prevention (CDC). Toxoplasmosis. Accessed April 22, 2025.
2. Rabilloud M, Wallon M, Peyron F. In utero and at birth diagnosis of congenital toxoplasmosis: use of likelihood ratios for clinical management. Pediatr Infect Dis J. 2010;29(5):421-425. doi:10.1097/INF.0b013e3181c80493
Diagnosis of Toxoplasmosis
Serologic testing
Histopathologic evaluation of biopsies
Polymerase chain reaction–based assays of blood, cerebrospinal fluid, tissue, or, during pregnancy, amniotic fluid
For central nervous system involvement, CT or MRI and lumbar puncture (rarely, brain biopsy)
Toxoplasmosis is usually diagnosed using serologic testing that includes an indirect fluorescent antibody (IFA) test or enzyme immunoassay (EIA) for both IgG and IgM antibody titers (see table ). Specific IgM antibodies appear during the first 2 weeks of acute illness, peak within 4 to 8 weeks, and eventually become undetectable, but they may be present for as long as 18 months after acute infection. IgG antibodies arise more slowly, peak in 1 to 2 months, and may remain high and stable for months to years. Assays for Toxoplasma IgM lack specificity; in regions with a low incidence of Toxoplasma infection, a proportion of the positive IgM test results will be false-positive (1).
Interpretation of Toxoplasma Serologic Testing*
IgG | IgM | Interpretation† |
|---|---|---|
Negative | Negative | No evidence of infection |
Negative | Equivocal | Possibly early infection or false-positive IgM result |
Negative | Positive | Possibly acute infection or false-positive IgM result |
Equivocal | Negative | Chronic indeterminate |
Equivocal | Equivocal | Chronic indeterminate |
Equivocal | Positive | Possibly acute infection |
Positive | Negative | Infection for ≥ 6 months |
Positive | Equivocal | Infection for probably > 1 year or false-positive IgM result |
Positive | Positive | Possibly recent infection in the last 12 months or false-positive IgM result |
* Except in infants less than 12 months. | ||
† If results are equivocal or interpretation is uncertain, testing additional samples at a reference laboratory or testing samples taken ≥ 2 weeks later may provide useful information. | ||
The diagnosis of acute toxoplasmosis during pregnancy and in the fetus or neonate can be difficult, and consultation with an expert is recommended. If the patient is pregnant and IgG and IgM are positive, an IgG avidity test should be performed. The presence of high avidity antibodies in the first 12 to 16 weeks of pregnancy essentially excludes an infection acquired during gestation. However, a low IgG avidity result cannot always be interpreted as indicating recent infection because some patients can have persistent low IgG avidity for many months after infection. Suspected recent infection in a pregnant patient should be confirmed before intervention by having samples tested at a toxoplasmosis reference laboratory. If the patient has clinical illness compatible with toxoplasmosis but the IgG titer is low, a follow-up titer 2 to 3 weeks later should show an increase in antibody titer if the illness is due to acute toxoplasmosis, unless the host is severely immunocompromised. If the titer is still low, amniocentesis should be considered for polymerase chain reaction (PCR) testing.
In general, the detection of Toxoplasma-specific IgM antibody in neonates suggests congenital infection. Maternal IgG crosses the placenta, but IgM does not; this suggests the source of the IgM is the fetus or neonate while in utero. Detection of Toxoplasma-specific IgA antibodies is more sensitive than IgM in congenitally infected infants, but IgA testing for toxoplasmosis is available only at special reference facilities (eg, the Dr. Jack S. Remington Laboratory for Specialty Diagnostics). An expert should be consulted when fetal or congenital infection is suspected. In immunocompromised patients, acute infection should be suspected if the IgG is positive. However, IgG antibody levels in patients with HIV infection and Toxoplasma encephalitis are usually low to moderate, and IgG antibodies are sometimes absent; IgM antibodies are not present.
Toxoplasma are occasionally demonstrated histopathologically. Tachyzoites, which are present during acute infection, take up Giemsa or Wright stain but may be difficult to find in routine tissue sections. Tissue cysts do not distinguish acute from chronic infection. Toxoplasma must be distinguished from other intracellular organisms, such as Histoplasma, Trypanosoma cruzi, and Leishmania. For parasite DNA in blood, PCR tests of cerebrospinal fluid (CSF), or amniotic fluid obtained via amniocentesis are available at several reference laboratories. PCR-based analysis of amniotic fluid is the preferred method to diagnose toxoplasmosis during pregnancy.
If central nervous system (CNS) toxoplasmosis is suspected, patients should have head CT with contrast, MRI with contrast, or both plus a lumbar puncture if there are no signs of increased intracranial pressure. MRI is more sensitive than CT. MRI and CT with contrast typically show single or multiple, rounded, ring-enhancing lesions. Although these lesions are not pathognomonic, their presence in patients with advanced HIV infection and CNS symptoms warrants a trial of chemotherapy for T. gondii. CSF may be positive for lymphocytic pleocytosis, and the protein level may be elevated.
If the suspected diagnosis of CNS toxoplasmosis is correct, clinical and radiographic improvement should become evident within 7 to 14 days. If symptoms worsen over the first week or do not lessen by the end of the second week, a brain biopsy should be considered. Hematoxylin-eosin staining showing cysts is definitive for diagnosis of CNS toxoplasmosis.


This image shows a T. gondii cyst in brain tissue stained with hematoxylin and eosin.
CDC/DPDx
Ocular disease is diagnosed based on the appearance of the lesions in the eye, symptoms, course of disease, and results of serologic testing.
Diagnosis reference
1. Kaul R, Chen P, Binder SR. Detection of immunoglobulin M antibodies specific for Toxoplasma gondii with increased selectivity for recently acquired infections. J Clin Microbiol. 2004;42(12):5705-5709. doi:10.1128/JCM.42.12.5705-5709.2004
Treatment of Toxoplasmosis
Pyrimethamine and sulfadiazine plus leucovorin (to prevent bone marrow suppression); alternatively, the fixed drug combination trimethoprim/sulfamethoxazole in some situations
Clindamycin or atovaquone plus pyrimethamine when the patient is allergic to sulfonamides or does not tolerate sulfadiazine
Spiramycin in pregnant patients (without evidence of fetal infection)
Treatment of toxoplasmosis is not indicated for immunocompetent patients who are asymptomatic or have mild, uncomplicated acute infection; treatment is required only when visceral disease is present or symptoms are severe or persist.
However, specific treatment is indicated for acute toxoplasmosis in the following patients:
Neonates
Pregnant patients with acute toxoplasmosis
Immunocompromised patients
Pearls & Pitfalls
|
Treatment of immunocompetent patients
The most effective regimen in immunocompetent patients with visceral involvement or severe or persistent symptoms is pyrimethamine plus sulfadiazine, for 2 to 4 weeks.
Leucovorin (folinic acid) is given concurrently to help protect against bone marrow suppression.
In patients who have or develop sulfonamide hypersensitivity, clindamycin is given with pyrimethamine and leucovorin instead of sulfonamides. Another option is atovaquone plus pyrimethamine and leucovorin. The fixed combination of trimethoprim/sulfamethoxazole has been used as an alternative as well as pyrimethamine and leucovorin plus clarithromycin, or dapsone, or azithromycin, but they have not been extensively studied.
Treatment of immunocompromised patients
Toxoplasmosis in immunocompromised patients is often fatal if untreated. In addition to antiparasitics, antiretroviral therapy should be optimized for patients with toxoplasmosis and HIV co-infection. Untreated or undertreated infections may disseminate.
Higher doses of pyrimethamine are used in immunocompromised patients, in patients with CNS toxoplasmosis, or, uncommonly, with involvement of other organs. A loading dose of pyrimethamine is given the first day, then regular doses are given once a day. Sulfadiazine is added for at least 6 weeks and for 4 to 6 weeks after resolution of clinical symptoms and signs. Pyrimethamine bone marrow suppression can be minimized with leucovorin, also called folinic acid (but not folate, which blocks the therapeutic effect). Even when leucovorin is given, the complete blood count should be monitored weekly.
If pyrimethamine is not available, trimethoprim/sulfamethoxazole IV or orally twice a day is a potentially effective alternative, but pyrimethamine is more active than trimethoprim against the parasite's dihydrofolate reductase.
If patients cannot take sulfonamides, pyrimethamine and leucovorin plus clindamycin can be used. Atovaquone with or without pyrimethamine and leucovorin is another option.
Chronic maintenance therapy is used after successful treatment of acute disease to prevent relapses in patients who remain immunocompromised. Relapses are particularly common in patients with advanced HIV infection who have a CD4 count < 200/mcL. Maintenance therapy is continued until the CD4 count remains > 200/mcL for > 6 months on antiretroviral therapy.
There are several options for maintenance therapy:
Sulfadiazine, pyrimethamine, and leucovorin
Clindamycin, pyrimethamine, and leucovorin
Atovaquone, pyrimethamine, and leucovorin
Atovaquone and sulfadiazine
Atovaquone only
Sulfadiazine and pyrimethamine plus leucovorin can be continued at lower doses than used for initial treatment. An alternative for patients who do not tolerate sulfonamides is clindamycin plus pyrimethamine plus leucovorin, but an additional agent is needed to prevent Pneumocystis jirovecii pneumonia. If pyrimethamine is not available or not tolerated, trimethoprim/sulfamethoxazole can be used for maintenance.
Other options for chronic maintenance therapy include atovaquone. The relapse rate may be higher with the atovaquone-based alternatives.
Treatment of ocular toxoplasmosis
Treatment of ocular toxoplasmosis is based on results of a complete ophthalmologic evaluation (degree of inflammation; visual acuity; size, location, and persistence of lesion).
Treatment is initiated with sulfadiazine, pyrimethamine, and leucovorin (1). In severe cases and in patients requiring additional local therapy, intravitreal clindamycin is a therapeutic option. Once treatment is completed, long-term trimethoprim/sulfamethoxazole prophylaxis is highly effective in preventing recurrences. Patients with ocular toxoplasmosis are also frequently given corticosteroids to reduce inflammation.
The Centers for Disease Control and Prevention (CDC) recommends that therapy for ocular toxoplasmosis be continued for 4 to 6 weeks, followed by reevaluation of the patient's condition (see also CDC: Clinical Care of Toxoplasmosis).
Treatment of pregnant patients
Treatment of pregnant patients with acute toxoplasmosis can decrease the incidence of fetal infection.
Spiramycin has been used safely to reduce transmission to the fetus in pregnant patients with acute toxoplasmosis during the first 18 weeks of pregnancy, but spiramycin is less active than pyrimethamine plus sulfonamide and does not cross the placenta. Spiramycin is continued until fetal infection is documented or excluded at 18 weeks gestational age when amniotic fluid is obtained and tested using a polymerase chain reaction (PCR)–based assay. If no transmission has occurred, spiramycin can be continued to term.
If the fetus is infected or a mother becomes infected after 18 weeks, pyrimethamine plus sulfadiazine plus leucovorin are used. NOTE: Pyrimethamine is a potent teratogen and should not be used during the first or early second trimester. Spiramycin is not commercially available in the United States but is available through the U.S. Food and Drug Administration's Office of Infectious Diseases.
Consultation with an infectious diseases expert is recommended.
Treatment of infants with congenital toxoplasmosis
Infants with congenital toxoplasmosis should be treated with pyrimethamine plus a sulfonamide for 1 year. Infants should also receive leucovorin while receiving pyrimethamine and for 1 week after pyrimethamine is stopped to prevent bone marrow suppression. The National Reference Laboratory for Toxoplasmosis (PAMF-TSL) and the Toxoplasmosis Center at the University of Chicago recommend pyrimethamine plus sulfadiazine plus leucovorin for the treatment of congenitally infected infants (2).
Treatment references
1. Durand ML, Barshak MB, Sobrin L. Eye Infections. N Engl J Med. 2023;389(25):2363-2375. doi:10.1056/NEJMra2216081
2. Maldonado YA, Read JS, Committee on Infectious Diseases. Diagnosis, treatment, and prevention of congenital toxoplasmosis in the United States. Pediatrics. 2017;139(2):e20163860. doi:10.1542/peds.2016-3860
Prevention of Toxoplasmosis
Patients at high risk of severe disease, including pregnant and immunocompromised patients, should be counselled as soon as possible on best practices for avoiding infection (1):
Cook all meat to an internal temperature of 74° C or higher, and use a meat thermometer if possible.
Avoid raw shellfish (clams, mussels, oysters), unpasteurized goat milk, and meat that has been smoked, cured in brine, or dried because these foods may still contain infectious cysts.
Peel or thoroughly wash fruits and vegetables before eating.
Wear gloves when handling raw meat.
Wash cutting boards, dishes, counters, utensils, and hands with hot soapy water after they have come in contact with raw meat, poultry, seafood, or unwashed fruits or vegetables.
Avoid untreated well water, which may be contaminated with cat feces.
Avoid contact with cat feces, especially handling of cat litter or when gardening. If changing cat litter or contact with soil cannot be avoided, wear disposable gloves and thoroughly wash hands with soap and warm water afterward.
Change cat litter boxes daily because T. gondii oocysts become infectious 1 to 5 days after being shed in cat feces.
Keep pet cats indoors and do not feed them raw or undercooked meat.
Do not handle or adopt stray cats during pregnancy.
Potential organ or blood donors may be screened to prevent the spread of toxoplasmosis through transplanted organs or donated blood.
Primary chemoprophylaxis is recommended for patients with HIV infection and a positive IgG T. gondii serologic test if their CD4 cell count is < 100/mcL. Trimethoprim/sulfamethoxazole, which also is prophylactic against Pneumocystis jirovecii, is typically used. Alternatives for patients who cannot tolerate trimethoprim/sulfamethoxazole at all include dapsone plus pyrimethamine and leucovorin or atovaquone with or without pyrimethamine. Chemoprophylaxis is continued until the CD4 cell count is > 200/mcL.
Prevention reference
1. Maldonado YA, Read JS; COMMITTEE ON INFECTIOUS DISEASES. Diagnosis, Treatment, and Prevention of Congenital Toxoplasmosis in the United States. Pediatrics. 2017;139(2):e20163860. doi:10.1542/peds.2016-3860
Key Points
T. gondii reproduces sexually in the intestinal tract of cats; most human infections result from direct or indirect contact with cat feces but can be acquired transplacentally or by ingestion of poorly cooked meat that contains cysts.
Approximately 12% of the United States population has been infected with T. gondii, but symptomatic disease is rare and occurs mainly in fetuses who are infected when the mother acquires acute infection during pregnancy and transmits the infection transplacentally or in people who are immunocompromised due to HIV or other causes.
Acute infection is usually asymptomatic in immunocompetent patients, but 10 to 20% have manifestations, similar to those of mononucleosis, including lymphadenopathy.
Immunocompromised patients typically present with encephalitis and have ring-enhancing intracranial mass lesions, seen on MRI or CT with contrast.
To diagnose, use serologic tests (for IgG and IgM antibodies), histopathology, or polymerase chain reaction tests.
Treatment is indicated mainly for congenitally infected neonates, pregnant patients with acute infection, and immunocompromised patients.
Use pyrimethamine and sulfadiazine plus leucovorin or, if the patient is allergic to sulfonamides or sulfadiazine is not tolerated, pyrimethamine and clindamycin.
Pyrimethamine is a potent teratogen and should not be used during the first and early second trimesters of pregnancy; spiramycin is recommended then for maternal infection.
Antiretroviral therapy should be optimized in patients with advanced HIV infection; suppressive treatment is continued until patients are asymptomatic and CD4 cell counts are > 200/mcL for > 6 months.
Drug Information for the Topic





