



Cutaneous myiasis is skin infestation by the larvae of certain fly species.
Myiasis involves the larvae (maggots) of two-winged flies (dipterous flies). Three types of cutaneous infestation exist, depending on the species involved:
Furuncular
Wound
Migratory


© Springer Science+Business Media
Other organs are sometimes involved (eg, nasopharynx, gastrointestinal tract, genitourinary tract). Infestation usually occurs in tropical countries, so most cases in the United States occur in people who have recently arrived from endemic areas.
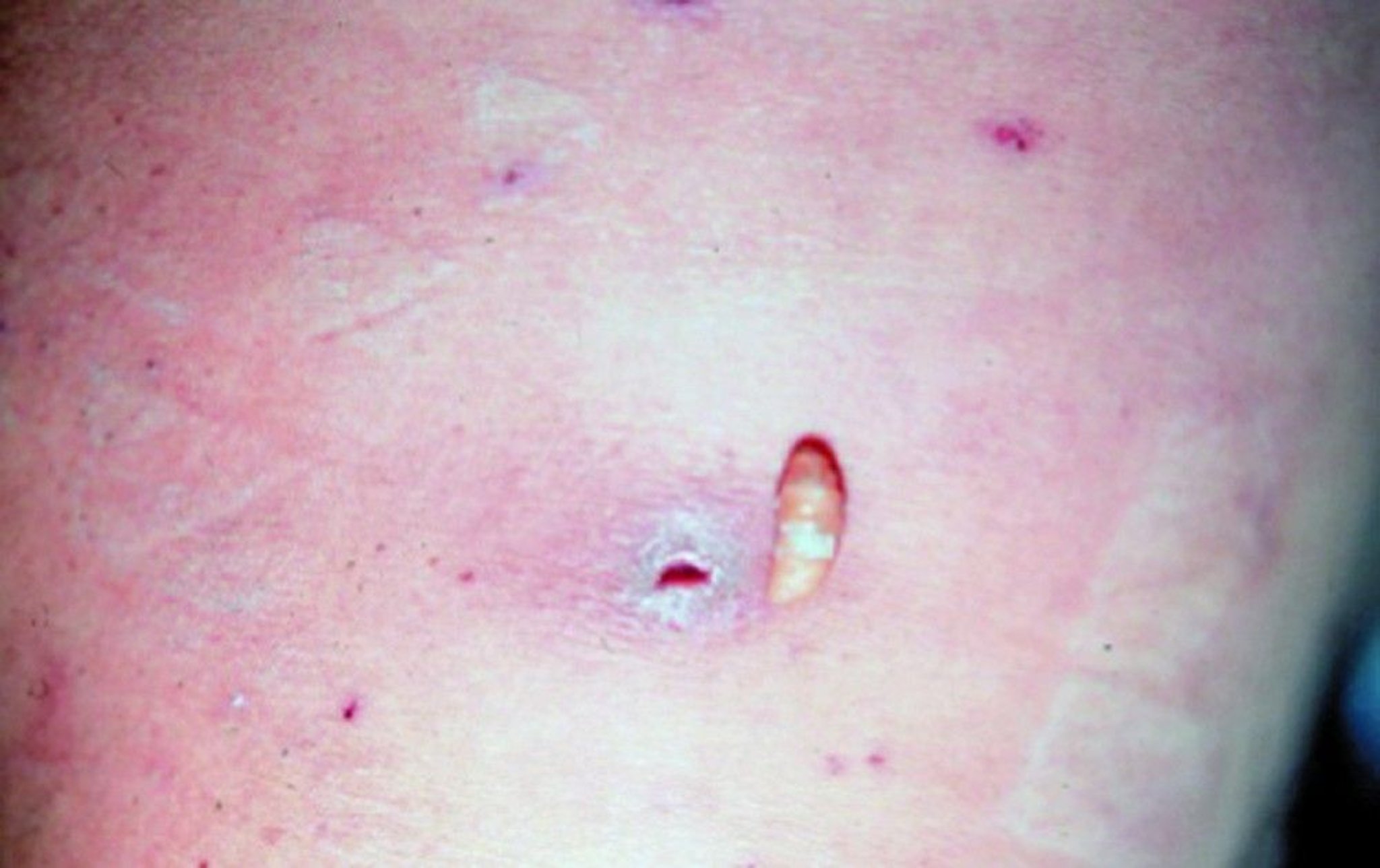
Furuncular Myiasis
A common source for furuncular myiasis is bot flies. Species of bot flies include Dermatobia hominis, native to South and Central America and the most common cause of furuncular myiasis in travelers returning to the United States, Cordylobia anthropophaga (in sub-Saharan Africa), various Cuterebra species (in North America), and Wohlfahrtia species (in North America, Europe, and Pakistan) (1). Many of the flies do not lay their eggs on humans but on other insects (eg, mosquitoes) or objects (eg, drying laundry) that may then come in contact with human skin. Eggs on the skin hatch into larvae, which subsequently burrow into the skin and develop through successive stages (instars) into mature larvae; mature larvae may be 1 to 2 cm long, depending on the species. If the infestation is untreated, larvae eventually emerge from the skin and drop to the ground to continue their life cycle.
Typical symptoms include pruritus, a sensation of movement, and sometimes lancinating pain. The initial lesion may resemble an arthropod bite or bacterial furuncle but may be distinguished by the presence of a central punctum with serosanguineous drainage; sometimes a small portion of the end of the larva is visible. D. hominis lesions are more common on the face, scalp, and extremities, whereas C. anthropophaga lesions usually occur in areas that are covered by clothing and appear on the head, neck, and back.
There is no single standardized treatment approach, but it generally involves occlusive techniques or administration of agents toxic to the worm or larvae followed by manual removal (2). The approach varies depending on the availability of interventions. Expectant management is inadvisable because of the risk of inadequate larval control and intense local inflammation, potentially leading to secondary infection.
Because larvae require atmospheric oxygen, production of localized hypoxia via occlusion of the skin opening (eg, application of petroleum jelly or a transparent adhesive film) may cause them to depart or at least come closer to the surface, facilitating manual removal (3).The numerous occlusive methods include use of petroleum jelly, transparent adhesive films, nail polish, bacon, or a paste of tobacco. One dose of oral ivermectin or topically applied ivermectin may kill the larvae or induce migration. Larvae may be extracted through a small incision under local anesthesia.
Furuncular myiasis references
1. Ragi SD, Kapila R, Schwartz RA. The Botfly, A Tropical Menace: A Distinctive Myiasis Caused by Dermatobia hominis. Am J Clin Dermatol. 2021;22(1):81-88. doi:10.1007/s40257-020-00522-2
2. Francesconi F, Lupi O. Myiasis. Clin Microbiol Rev. 2012;25(1):79-105. doi:10.1128/CMR.00010-11
3. Solomon M, Lachish T, Schwartz E. Cutaneous myiasis. Curr Infect Dis Rep. 8(9):28, 2016. doi: 10.1007/s11908-016-0537-6
Wound Myiasis

This maggot is adjacent to an ulcerated wound.
© Springer Science+Business Media
Wound myiasis refers to infestation of pre-existing wounds or ulcers, with visible maggots (most often from green or black blowflies but not common houseflies) feeding on necrotic or healthy tissue. Open wounds and mucous membranes, especially in people who are unsheltered, those who have alcohol use disorder, and anyone experiencing substandard hygienic conditions, may be at higher risk of infestation, most often from the screwworm fly, but also sometimes from green or black blowflies.
Treatment of wound myiasis is usually with irrigation and manual debridement.
New World screwworm fly
Cochliomyia hominivorax, the New World screwworm, is primarily a cause of veterinary disease and can pose a threat to animal health, infesting livestock (especially cattle), pets, and wildlife (1, 2, 3). Outbreaks spreading northward from South America (through Central America and Mexico) and the Caribbean have led to cross-species transmission. Rarely, it can spread to humans living in endemic regions by depositing eggs, typically in wounds or body cavities lined by mucosa, but sometimes on healthy skin.


U.S. Department of Agriculture Animal and Plant Health Inspection Service (APHIS)
The clinical presentation is typically wound myiasis. Symptoms include painful, malodorous cutaneous or mucosal lesions, often with serosanguinous or purulent discharge. Conspicuous motile larvae in wounds and ulcers are generally visible. Rapid spread within the individual is typical with expanding ulceration, necrosis, and tissue destruction (4). Older and immunocompromised adults can develop more severe infection.
Diagnosis is primarily clinical, based on the identification via morphological examination of extracted larvae with species confirmation, when available, by molecular methods (eg, cytochrome c oxidase gene sequencing).
Treatment is by thorough mechanical removal of all visible larvae, which is the mainstay of therapy. Supportive measures include wound debridement, irrigation, and management of secondary bacterial infection with appropriate antibiotics. Pharmacotherapy with ivermectin has demonstrated efficacy in facilitating larval death (5).
Prevention is key and requires a multifaceted strategy involving (6):
Minimizing exposure to infested animals (eg, covering wounds, wearing appropriate clothing, enhancing overall sanitation and personal hygiene)
Early, rapid, and thorough wound care
Public health education
Robust surveillance
Sterile insect technique (ie, where mass-released sterilized male flies mate with wild females, resulting in no viable offspring) (7)
Wound myiasis references
1. Valdez-Espinoza UM, Fadda LA, Marques R, Osorio-Olvera L, Jiménez-García D, Lira-Noriega A. The reemergence of the New World screwworm and its potential distribution in North America. Sci Rep. 2025;15(1):23819. Published 2025 Jul 3. doi:10.1038/s41598-025-04804-9
2. U.S. Department of Agriculture: Animal and Plant Health Inspection Service. New World Screwworm Outbreak in Central America and Mexico, September 26, 2025. Accessed October 16, 2025.
3. U.S. Centers for Disease and Prevention (CDC). Clinical Overview of New World Screwworm. September 30, 2025. Accessed October 16, 2025.
4. Venegas-Montero DP, Alfaro-Vellanero MJ, Rojas-Araya D, et al. Case Report: Re-Emergence of Cochliomyia hominivorax in Costa Rica: Report of a Human Myiasis Case 23 Years after Elimination. Am J Trop Med Hyg. 2024;111(5):1020-1023. Published 2024 Sep 17. doi:10.4269/ajtmh.24-0342
5. Osorio J, Moncada L, Molano A, Valderrama S, Gualtero S, Franco-Paredes C. Role of ivermectin in the treatment of severe orbital myiasis due to Cochliomyia hominivorax. Clin Infect Dis. 2006;43(6):e57-e59. doi:10.1086/507038
6. U.S. Centers for Disease Control and Prevention (CDC). About New World Screwworm. August 27, 2025. Accessed October 3, 2025.
7. Skoda SR, Phillips PL, Welch JB. Screwworm (Diptera: Calliphoridae) in the United States: Response to and Elimination of the 2016-2017 Outbreak in Florida. J Med Entomol. 2018 Jun 28;55(4):777-786. doi: 10.1093/jme/tjy049. PMID: 29722869.
Migratory Myiasis
Migratory myiasis (also called creeping myiasis) refers to infestation caused by the movement of dipterous fly larvae through the skin, producing serpiginous, migratory tracks. The most common species are Gasterophilus intestinalis and Hypoderma species. These flies typically infest livestock, including horses and cattle. People acquire them via contact with infested animals or, less often, via direct egg-laying on their skin.
The clinical presentation of migratory myiasis is distinct from furuncular and wound myiasis. Larvae of these flies burrow under the skin, causing erythematous, pruritic, advancing lesions. These lesions may be mistaken for cutaneous larva migrans; however, fly larvae are much larger than nematodes, and the lesions resulting from fly larvae extend much more slowly, and persist much longer than the lesions of cutaneous larva migrans (1).
Diagnosis is primarily clinical and is based on the characteristic appearance of migratory tracks and supported by exposure history (especially exposure to livestock). Treatment of migratory myiasis is similar to that of furuncular myiasis.
Migratory myiasis reference
1. Francesconi F, Lupi O. Myiasis. Clin Microbiol Rev. 2012;25(1):79-105. doi:10.1128/CMR.00010-11
Drug Information for the Topic





