



Patients with or without respiratory disorders who are in the intensive care unit (ICU)—and other patients—may develop hypoxia (oxygen saturation < 90%) during a hospital stay. Hypoxia in patients with known respiratory conditions is discussed elsewhere in The Manual in chapters regarding each disorder.
Etiology of Hypoxia
Numerous disorders cause hypoxia (eg, dyspnea, respiratory failure—see table ); however, acute hypoxia developing in a patient hospitalized with a nonrespiratory illness usually has a more limited set of causes. These causes can be divided into:
Disorders of ventilation
Disorders of oxygenation
Some Causes of Hypoxia
Mechanism | Examples |
|---|---|
Disorders of ventilation | |
Decreased ventilatory drive | Decreased mental status (eg, caused by head injury, oversedation, sepsis, shock, or stroke) |
Obstructed ventilation | Bronchospasm Dislodgement of endotracheal tube Mucus plugging of the airways or endotracheal tube |
Restricted movement of chest wall | Altered respiratory mechanics from injury or splinting secondary to pain from:
|
Disorders of oxygenation | |
Pulmonary causes | Acute respiratory distress syndrome Atelectasis, pneumonia, pneumothorax, pulmonary embolus, pulmonary contusion, aspiration pneumonitis |
Nonpulmonary causes | Iatrogenic fluid overload Heart failure (eg, due to exacerbation of underlying disease or to acute myocardial infarction) |

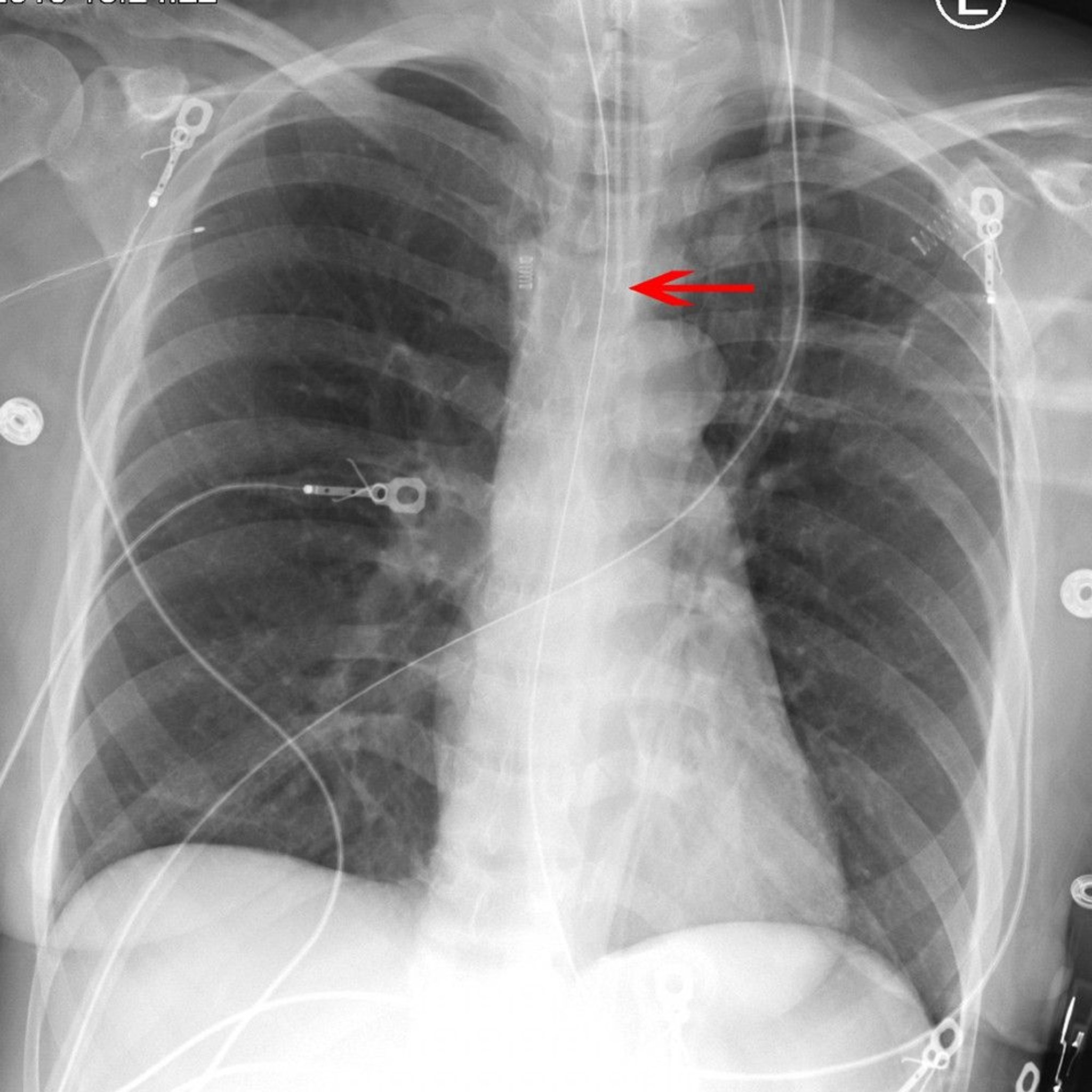
The arrow points to the tip of an endotracheal tube in the appropriate position above the carina.
© 2017 Elliot K. Fishman, MD.
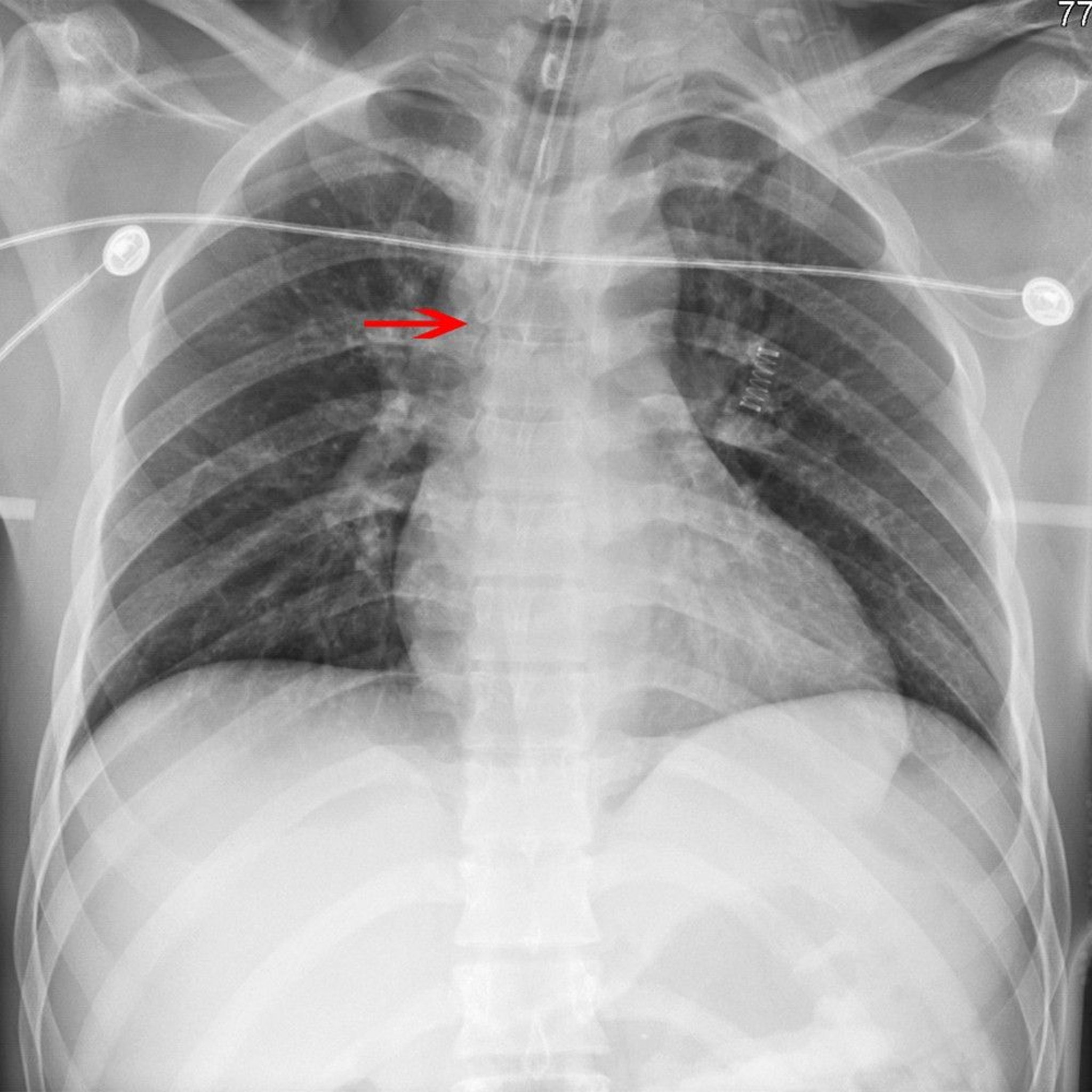
The arrow points to the tip of an endotracheal tube placed incorrectly in the right mainstem bronchus.
© 2017 Elliot K. Fishman, MD.
Evaluation of Hypoxia
Total fluid volume given during the hospital stay and, in particular, during the previous 24 hours should be ascertained to identify volume overload. Medications should be reviewed for sedative administration and dosage. In significant hypoxia (oxygen saturation < 85%), treatment begins simultaneously with evaluation.
History
Very sudden onset dyspnea and hypoxia suggest pulmonary embolus (PE) or pneumothorax (mainly in a patient receiving positive pressure ventilation). Fever, chills, and productive cough (or increased secretions) suggest pneumonia. Symptoms and signs of myocardial infarction may indicate acute valvular insufficiency, pulmonary edema, or cardiogenic shock. Unilateral extremity pain suggests deep venous thrombosis (DVT) and hence possible PE. Preceding major trauma or sepsis requiring significant resuscitation suggests acute respiratory distress syndrome. Renal failure indicates higher risk of fluid overload. Preceding chest trauma suggests pulmonary contusion.
A history of cardiopulmonary disease (eg, asthma, chronic obstructive pulmonary disease, heart failure) may indicate an exacerbation of the disease.
Physical examination
Patency of the airway and strength and adequacy of respirations should be assessed immediately. Tachypnea, tachycardia, or both may be initial indications of hypoxia. For patients on mechanical ventilation, it is important to determine that the endotracheal tube is not obstructed or dislodged. Findings are suggestive as follows:
Unilateral decreased breath sounds with clear lung fields suggest pneumothorax or right mainstem bronchus intubation; with lung crackles and fever, pneumonia is more likely.
Distended neck veins with bilateral lung crackles suggest volume overload with pulmonary edema, cardiogenic shock, pericardial tamponade (often without lung crackles), or acute valvular insufficiency.
Distended neck veins with clear lungs or unilateral decrease in breath sounds and tracheal deviation suggest tension pneumothorax.
Bilateral lower-extremity edema suggests heart failure, but unilateral edema suggests DVT and hence possible PE.
Wheezing represents bronchospasm (typically asthma or allergic reaction, but it occurs rarely with PE or heart failure).
Decreased mental status suggests hypoventilation.
Testing
Hypoxia is generally detected initially by pulse oximetry. Testing should include:
A chest radiograph (eg, to assess for pneumonia, pleural effusion, pneumothorax, heart failure, or atelectasis)
ECG (to assess for arrhythmia or ischemia)
Arterial blood gases (ABGs), to confirm hypoxia and evaluate adequacy of ventilation
Bedside echocardiography performed by an intensivist may be used to assess for hemodynamically significant pericardial effusion or reduced global left ventricular or right ventricular function until formal echocardiography can be performed. Point-of-care ultrasound can also be performed to identify pneumothorax.
Elevated serum levels of brain (B-type) natriuretic peptide (BNP) may help differentiate heart failure from other causes of hypoxia. If diagnosis remains unclear after these tests, testing for PE should be considered.
Bronchoscopy may be performed in intubated patients or in patients with a tracheostomy to exclude or remove a tracheobronchial mucous plug.
Treatment of Hypoxia
Treatment of specific diseases is discussed elsewhere in The Manual. If hypoxia persists, mechanical ventilation via noninvasive positive pressure ventilation or endotracheal intubation is necessary. Persistent hypoxia requires supplemental oxygen.
Oxygen therapy
Oxygen should be administered even if definitive etiology is not yet identified. The amount of oxygen given is guided by arterial blood gases (ABG) or pulse oximetry to maintain PaO2 between 60 and 80 mm Hg (ie, 92 to 100% saturation) without causing oxygen toxicity. This level provides satisfactory tissue oxygen delivery; because the oxyhemoglobin dissociation curve (see figure ) is sigmoidal, increasing PaO2 to > 80 mm Hg increases oxygen delivery very little and is not necessary. The lowest fractional inspired oxygen (FiO2) that provides an acceptable PaO2 should be provided. Oxygen toxicity is:
Concentration-dependent
Time-dependent
Sustained elevations in FiO2 > 60% result in inflammatory changes, alveolar infiltration, and, eventually, pulmonary fibrosis. An FiO2 > 60% should be avoided unless a PaO2 ≥ 60 mmHg cannot be maintained. An FiO2 < 60% is well tolerated for long periods.
An FiO2 < 40% can be given via nasal cannula or simple face mask. A nasal cannula uses an oxygen flow of 1 to 6 L/minute. Because 6 L/minute is sufficient to fill the nasopharynx, higher flow rates are of no benefit. Simple face masks and nasal cannulas do not deliver a precise FiO2 because of inconsistent admixture of oxygen with room air from leakage and mouth breathing. However, Venturi-type masks can deliver very accurate oxygen concentrations.

An FiO2 > 40% requires use of an oxygen mask with a reservoir that is inflated by oxygen from the supply. In the typical nonrebreather mask, the patient inhales 100% oxygen from the reservoir, but during exhalation, a rubber flap valve diverts exhaled breath to the environment, preventing admixture of carbon dioxide and water vapor with the inspired oxygen. Nonetheless, because of leakage, such masks deliver an FiO2 of at most 80 to 90%.
High-flow nasal cannula (HFNC) oxygen therapy, in contrast to traditional nasal oxygen, delivers oxygen at rates from 20 to 60 L/minute; the oxygen is humidified. Humidification helps prevent airway desiccation and inflammation, maintain mucociliary function, and improve mucus clearance. HFNC therapy tends to reduce upper airway dead space and decrease the work of breathing more than non-rebreather masks. This therapy may help patients with hypoxemic respiratory failure not due to heart failure and who are not hypercapneic.
If hypoxia does not resolve despite administration of supplemental oxygen, mechanical ventilation is required. Mechanical ventilation can help treat disorders of ventilation as well as disorders of oxygenation (see table ).
Refractory hypoxia despite mechanical ventilation may require neuromuscular blockade, recruitment maneuvers, prone ventilation, or venovenous extracorporeal membrane oxygenation (ECMO).
Key Points
Hypoxia can be caused by disorders of ventilation and/or oxygenation and is usually first detected by pulse oximetry.
Patients should have a chest radiograph, ECG, and arterial blood gas measurements (to confirm hypoxia and evaluate adequacy of ventilation); if diagnosis remains unclear, consider testing for pulmonary embolus.
Give oxygen as needed to maintain PaO2 between 60 and 80 mm Hg (ie, 92 to 100% saturation) and treat the cause.





