

Thoracic trauma causes about 25% of deaths due to trauma in the United States. Many chest injuries cause death during the first minutes or hours after trauma; they can frequently be treated at the bedside with definitive or temporizing measures that do not require advanced surgical training.

Etiology of Thoracic Trauma
Chest injuries can result from blunt or penetrating trauma. The most important chest injuries include the following:
Pneumothorax (traumatic pneumothorax, open pneumothorax, and tension pneumothorax)
Many patients have simultaneous hemothorax and pneumothorax (hemopneumothorax).
Bone injuries are common, typically involving the ribs and clavicle, but fractures of the sternum and scapula may occur. The esophagus and diaphragm (see Overview of Abdominal Trauma) also can be damaged by chest trauma. Because the diaphragm can be as high as the nipple line during exhalation, penetrating trauma to the chest at or below nipple level can also cause intra-abdominal injuries.
Pathophysiology of Thoracic Trauma
Most morbidity and mortality due to chest trauma occurs because injuries interfere with respiration, circulation, or both.
Respiration can be compromised by
Direct damage to the lungs or airways
Altered mechanics of breathing
Injuries that directly damage the lung or airways include pulmonary contusion and tracheobronchial disruption. Injuries that alter the mechanics of breathing include hemothorax, pneumothorax, and flail chest. Injury to the lung, tracheobronchial tree, or rarely esophagus may allow air to enter the soft tissues of the chest and/or neck (subcutaneous emphysema) or mediastinum (pneumomediastinum). This air itself rarely has significant physiologic consequence; the underlying injury is the problem. Tension pneumothorax impairs respiration as well as circulation. Pulmonary contusion creates a ventilation and perfusion mismatch because of lung hemorrhage and edema.
Circulation can be impaired by
Bleeding
Decreased venous return
Direct cardiac injury
Bleeding, as occurs in hemothorax, can be massive, causing shock (respiration is also impaired if hemothorax is large). Decreased venous return impairs cardiac filling, causing hypotension. Decreased venous return can occur due to increased intrathoracic pressure in tension pneumothorax or to increased intrapericardial pressure in cardiac tamponade. Heart failure and/or conduction abnormalities can result from blunt cardiac injury that damages the myocardium or the heart valves.
Complications
Because chest wall injuries typically make breathing very painful, patients often limit inspiration (splinting). A common complication of splinting is atelectasis, which can lead to hypoxemia, pneumonia, or both.
Patients treated with tube thoracostomy, particularly if a hemothorax is incompletely drained, may develop purulent intrathoracic infection (empyema).
Significant pulmonary contusion can require similar treatment strategies as needed in patients with acute respiratory distress syndrome (ARDS).
Symptoms and Signs of Thoracic Trauma
Symptoms include pain, which usually worsens with breathing if the chest wall is injured, and sometimes shortness of breath.
Common findings include chest tenderness, ecchymoses, and respiratory distress; hypotension or shock may be present.
Neck vein distention can occur in tension pneumothorax or cardiac tamponade if patients have sufficient intravascular volume.
Decreased breath sounds can result from pneumothorax or hemothorax; percussion over the affected areas is dull with hemothorax and hyperresonant with pneumothorax.
The trachea can deviate away from the side of a tension pneumothorax.
In flail chest, a segment of the chest wall moves paradoxically—that is, in the opposite direction from the rest of the chest wall (outward during expiration and inward during inspiration); the flail segment is often palpable.
Subcutaneous emphysema causes a crackling or crunch when palpated. Findings may be localized to a small area or involve a large portion of the chest wall and/or extend to the neck. Most often, pneumothorax is the cause; when extensive, injury to the tracheobronchial tree or upper airway should be considered. Air in the mediastinum may produce a characteristic crunching sound synchronous with the heartbeat (Hamman sign or Hamman crunch). Hamman sign suggests pneumomediastinum and often tracheobronchial tree injury or, rarely, esophageal injury.
Diagnosis of Thoracic Trauma
History and physical examination
Chest x-ray
Sometimes other imaging studies (eg, CT, ultrasonography, aortic imaging studies)
Initial evaluation
Five conditions are immediately life threatening and rapidly correctable:
Diagnosis and treatment begin during the primary survey (see Approach to the Trauma Patient) and are based first on clinical findings. Depth and symmetry of chest wall excursion are assessed, the lungs are auscultated, and the entire chest wall and neck are inspected and palpated. Patients in respiratory distress should be monitored with serial assessments of clinical status and of oxygenation plus ventilation (eg, with pulse oximetry, arterial blood gas tests, capnometry if intubated).
Penetrating chest wounds should not be probed. However, their location helps predict risk of injury. High-risk wounds are those medial to the nipples or scapulae and those that traverse the chest from side to side (ie, entering one hemithorax and exiting the other). Such wounds may injure the hilar or great vessels, heart, tracheobronchial tree, or rarely the esophagus.
Patients with symptoms of partial or complete airway obstruction following blunt trauma should be immediately intubated to control the airway.
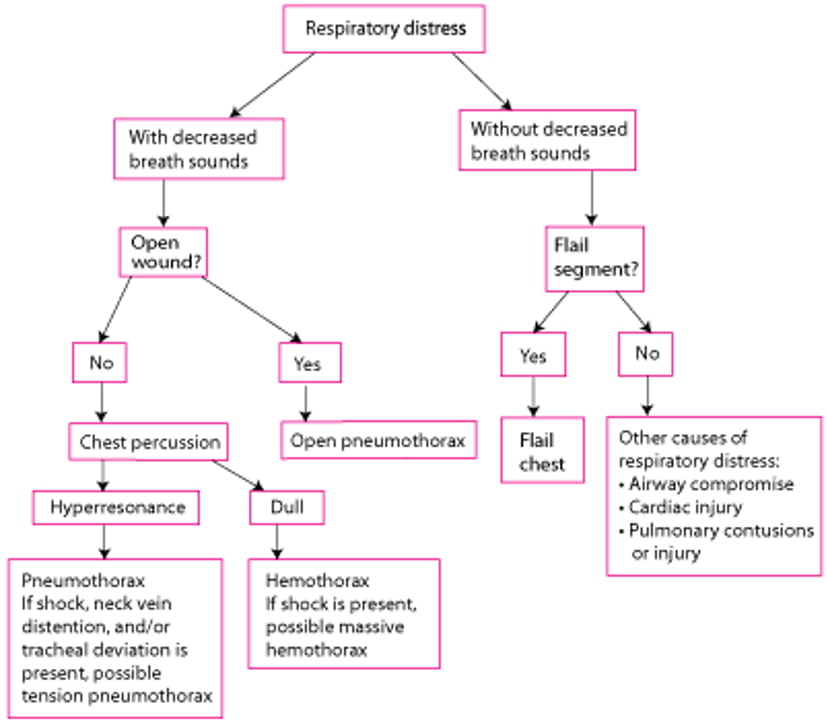
In patients with difficulty breathing, severe injuries to consider during the primary survey include the following:
Tension pneumothorax
Open pneumothorax
Massive hemothorax
Flail chest
There is a simplified, rapid approach to help differentiate these injuries (see figure A Simplified, Rapid Approach to Assessment of Patients With Chest Trauma).
A Simplified, Rapid Assessment of Patients With Thoracic Trauma and Respiratory Distress During the Primary Survey

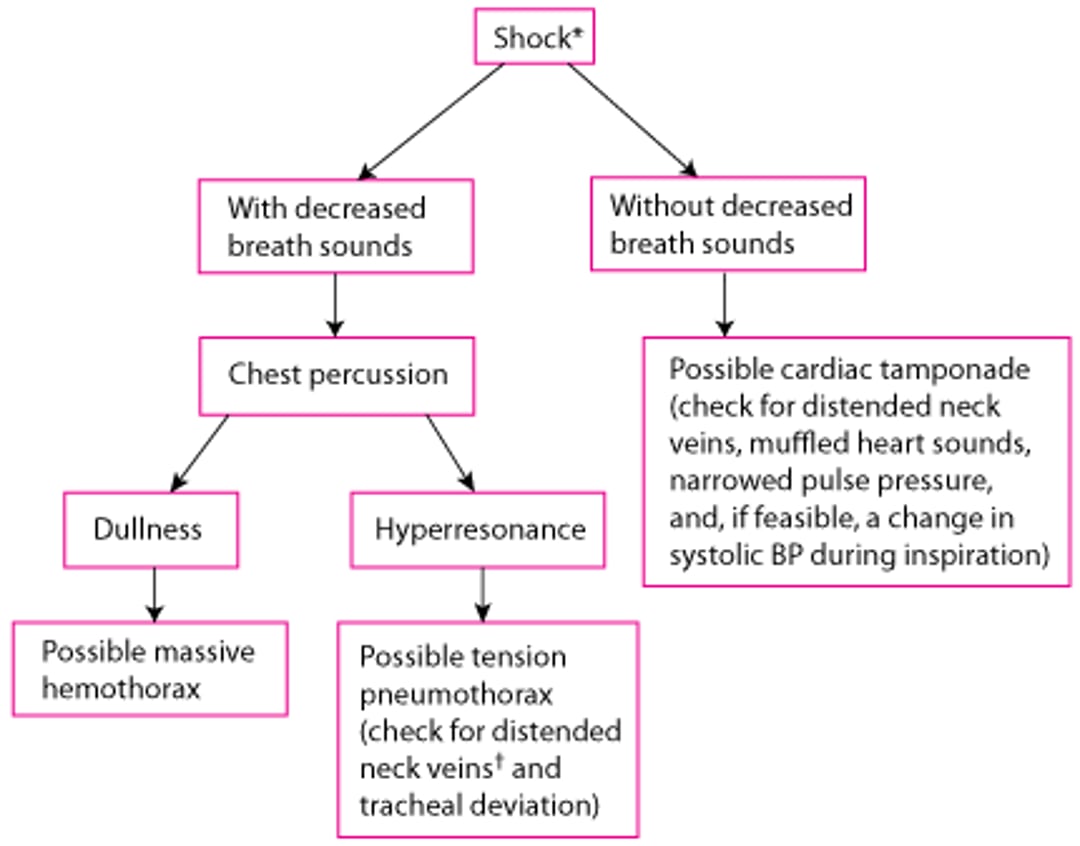
In patients with thoracic trauma and impaired circulation (signs of shock), severe injuries to consider during the primary survey include the following:
Massive hemothorax
Tension pneumothorax
Cardiac tamponade
Other chest injuries (eg, blunt cardiac injury, aortic disruption) may cause shock but are not treated during the primary survey. Simplified, rapid approaches can help differentiate among rapidly correctable causes of shock due to chest injuries (see figure A Simplified, Rapid Assessment for Chest Injuries in Patients With Shock...). However, hemorrhage should be excluded in all patients who have shock after major trauma, regardless of whether a chest injury that could cause shock is identified.
A Simplified, Rapid Assessment for Chest Injuries in Patients With Shock During the Primary Survey
* Hemorrhage should be excluded in all patients who are in shock after major trauma, regardless of whether a chest injury that could cause shock is identified † Neck vein distention may be absent in patients with hypovolemic shock. |

Treatment of injuries affecting the airway, breathing, or circulation begins during the primary survey. After the primary survey, patients are clinically assessed in more detail for other severe chest injuries as well as less severe manifestations of the injuries considered during the primary survey.
Imaging
Imaging studies are typically required in patients with significant chest trauma. Chest x-ray is virtually always done. Results are usually diagnostic of certain injuries (eg, pneumothorax, hemothorax, moderate or severe pulmonary contusion, clavicle fracture, some rib fractures) and suggestive for others (eg, aortic disruption, diaphragmatic rupture). However, findings may evolve over hours (eg, in pulmonary contusion and diaphragmatic injury). Plain x-rays of the scapula or sternum are sometimes done when there is tenderness over those structures.
In trauma centers, during the E-FAST (Extended Focused Assessment With Sonography in Trauma) examination, ultrasonography of the heart is typically done during the resuscitation phase to look for pericardial tamponade; some pneumothoraces can also be seen.
CT of the chest is often done when aortic injury is suspected and to diagnose small pneumothoraces, sternal and rib fractures, or mediastinal (eg, heart, esophageal, bronchial) injuries; thoracic spine injuries also will be identified.
Other tests for aortic injury include aortography and transesophageal echocardiography.
Laboratory and other testing
Complete blood count is often done but is mainly valuable as a baseline for detecting ongoing hemorrhage. Arterial blood gas results help monitor patients with hypoxia or respiratory distress. Normal cardiac markers (eg, troponin) can help exclude blunt cardiac injury in patients with chest trauma.
ECG is typically done for chest trauma that is severe or compatible with cardiac injury. Cardiac injury may cause arrhythmia, conduction abnormalities, ST segment abnormalities, or a combination.
Treatment of Thoracic Trauma
Supportive care
Treatment of specific injuries
Immediately life-threatening injuries are treated at the bedside at the time of diagnosis:
Respiratory distress with suspected tension pneumothorax: Needle decompression or finger thoracostomy.
Respiratory distress or shock with decreased breath sounds and suspected hemothorax: Tube thoracostomy
Respiratory distress with suspected open pneumothorax: Partially occlusive dressing followed by tube thoracostomy
Respiratory distress with suspected flail chest: Mechanical ventilation
Shock with suspected cardiac tamponade: Pericardiocentesis
Suspected hypovolemic shock: Fluid resuscitation and blood products when available
Immediate resuscitative thoracotomy can be considered for trauma victims if the clinician is proficient in the procedure and the patient has one of the following indications:
Penetrating thoracic injury with a need for cardiopulmonary resuscitation (CPR) of < 15 minutes
Penetrating nonthoracic trauma with a need for CPR of < 5 minutes
Blunt trauma with a need for CPR of < 10 minutes
Persistent systolic blood pressure of < 60 mm Hg due to suspected cardiac tamponade, hemorrhage, or air embolism
Pearls & Pitfalls
|
In the absence of any of these criteria, resuscitative thoracotomy is contraindicated because the procedure has significant risks (eg, transmission of blood-borne diseases, injury to clinician) and costs.
Specific treatment is directed at the injury. Supportive therapy typically includes analgesics, supplemental oxygen, and sometimes mechanical ventilation (1, 2).
Treatment references
1. Torres CM, Kent A, Scantling D, et al: Association of whole blood with survival among patients presenting with severe hemorrhage in US and Canadian adult civilian trauma centers. JAMA Surg 158(5):532-540, 2023. doi: 10.1001/jamasurg.2022.6978
2. Holcomb JB, Tilley BC, Baraniuk S, et al: Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA 313(5):471-482, 2015. doi: 10.1001/jama.2015.12





