



Vitiligo is a loss of melanocytes that causes patches of skin to turn white.
Patches of whitened skin are present on various parts of the body.
Doctors usually base the diagnosis on the appearance of the skin.
People may be treated with corticosteroid creams or sometimes pills, other creams, phototherapy, or, if needed, skin grafts or tattooing may be done.
(See also Overview of Skin Pigment.)
Vitiligo affects up to 2% of people.
Causes of Vitiligo
The cause of vitiligo is unknown, but it is a disorder of skin pigmentation that may involve an attack by the immune system on the cells that produce the skin pigment melanin (melanocytes).
Vitiligo tends to run in families, or people may spontaneously develop it.
Vitiligo may occur with certain other diseases, such as autoimmune disorders (when the body attacks its own tissues) and particularly thyroid disease. It is most strongly associated with an overactive thyroid (hyperthyroidism, particularly when caused by Graves disease) and an underactive thyroid (hypothyroidism, particularly when caused by Hashimoto thyroiditis). People with diabetes, Addison disease, and pernicious anemia also are somewhat more likely to develop vitiligo. However, the relationship between these disorders and vitiligo is unclear.
Occasionally, vitiligo occurs after physical injury to the skin, for example, as a response to a chemical burn or sunburn. People may also notice vitiligo is triggered by an episode of emotional stress.
Immunotherapy can also trigger vitiligo as a side effect (for example, when immunotherapy is used for treatment of melanoma).
Symptoms of Vitiligo
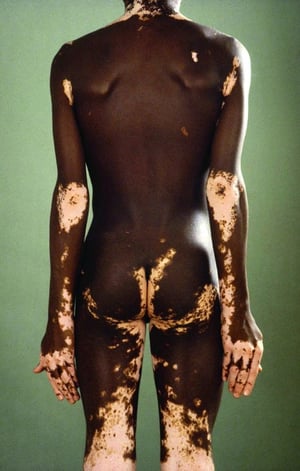
In some people, 1 or 2 well-defined patches of vitiligo appear. In other people, patches appear over a large part of the body. Rarely, vitiligo occurs over most of the skin surface. The changes are most striking in people with dark skin.
Commonly affected areas are the face, fingers and toes, wrists, elbows, knees, hands, shins, ankles, armpits, anus and genital area, navel, and nipples. The affected skin is extremely prone to sunburn. The areas of skin affected by vitiligo also produce white hair because melanocytes are lost from the hair follicles.


The white spots on the ankle are vitiligo, which is caused by loss of skin pigment–producing cells (melanocytes).
The white spots on the ankle are vitiligo, which is caused by loss of skin pigment–producing cells (melanocytes).
Photo provided by Thomas Habif, MD.


© Springer Science+Business Media

© Springer Science+Business Media

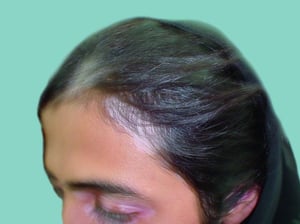
Hair in areas affected by vitiligo is usually white.
Hair in areas affected by vitiligo is usually white.
© Springer Science+Business Media
The white spots on the ankle are vitiligo, which is caused by loss of skin pigment–producing cells (melanocytes).
The white spots on the ankle are vitiligo, which is caused by loss of skin pigment–producing cells (melanocytes).
Photo provided by Thomas Habif, MD.
© Springer Science+Business Media
© Springer Science+Business Media
Hair in areas affected by vitiligo is usually white.
Hair in areas affected by vitiligo is usually white.
© Springer Science+Business Media
Diagnosis of Vitiligo
A doctor's evaluation
Vitiligo is recognized by its typical appearance.
A Wood light examination is often done to help distinguish vitiligo from other causes of lightened skin.
Other tests, including skin biopsies, are rarely necessary.


Vitiligo is viewed more easily under a Wood light (right).
Treatment of Vitiligo
Sun protection
Cream containing a corticosteroid and calcipotriene or sometimes other substances applied to the skin (topical therapy) Cream containing a corticosteroid and calcipotriene or sometimes other substances applied to the skin (topical therapy)
Phototherapy
Corticosteroids taken by mouth (oral therapy)
Surgery or tattooing
Bleaching unaffected skin
No cure is known for vitiligo, and the disorder can be challenging to manage. However, skin color may return spontaneously. Treatment may be helpful.
All affected areas of skin are at risk of severe sunburn and should be protected from the sun with clothing and sunscreen. Long-term sun exposure can increase the risk of skin cancer.
Topical therapy
Small patches sometimes darken (repigment) when treated with strong corticosteroid creams. Medications such as tacrolimus or pimecrolimus may be applied to patches on the face or groin, where strong corticosteroid creams may cause side effects. A cream containing calcipotriene (also called calcipotriol), which is a form of vitamin D, and betamethasone (a corticosteroid cream) is more effective than either cream used alone. Small patches sometimes darken (repigment) when treated with strong corticosteroid creams. Medications such as tacrolimus or pimecrolimus may be applied to patches on the face or groin, where strong corticosteroid creams may cause side effects. A cream containing calcipotriene (also called calcipotriol), which is a form of vitamin D, and betamethasone (a corticosteroid cream) is more effective than either cream used alone.
Ruxolitinib cream is available for the treatment of vitiligo. However, depigmentation can recur after use of this medication is stopped.Ruxolitinib cream is available for the treatment of vitiligo. However, depigmentation can recur after use of this medication is stopped.
Some people simply use bronzers, skin stains, or makeup to darken the affected area.
Phototherapy
Because many people still have a few melanocytes in the patches of vitiligo, exposure to ultraviolet (UV) light in a doctor’s office (phototherapy) restimulates pigment production in more than half of them (see sidebar ). However, phototherapy takes months to years to be effective and may need to be continued indefinitely. It can also lead to skin cancer.
Doctors also use lasers on some people who have small patches that do not darken after use of corticosteroid creams.
Oral therapy
Some people have vitiligo that rapidly spreads over weeks to months. Doctors sometimes give these people a low-dose oral corticosteroid for a couple of weeks to limit the spread.
Because oral corticosteroids do not darken the skin, people are also given phototherapy to stimulate pigment production.
Surgery
Areas that do not respond to phototherapy may be treated with various skin-grafting techniques and even transplantation of melanocytes grown from unaffected areas of the person’s skin.
Tattooing is especially useful for areas where it is difficult to restimulate pigment production (such as the nipples, lips, and fingertips).
Bleaching
Some people who have very large areas of vitiligo sometimes prefer to bleach the pigment out of the unaffected skin to achieve an even color. Bleaching is done with repeated applications of a strong hydroquinone cream to the skin for weeks to 1 year or more. The cream can be extremely irritating. Some people who have very large areas of vitiligo sometimes prefer to bleach the pigment out of the unaffected skin to achieve an even color. Bleaching is done with repeated applications of a strong hydroquinone cream to the skin for weeks to 1 year or more. The cream can be extremely irritating.
The effects of bleaching (such as permanent loss of pigment) are irreversible.
Drug Information for the Topic





