

Mediastinal masses are caused by a variety of cysts and tumors; likely causes differ by patient age and location of the mass (anterior, middle, or posterior mediastinum). They may be asymptomatic (common in adults) or cause systemic symptoms or obstructive respiratory symptoms (more likely in children). Testing involves CT with biopsy or surgical resection and adjunctive tests as needed. Treatment differs by cause.
Mediastinal masses are divided into those that occur in the anterior, middle, and posterior mediastinum. The anterior mediastinum extends from the sternum to the pericardium in the inferior region and from the sternum to the brachiocephalic vessels in the superior region. The middle mediastinum lies between the anterior and posterior mediastinum. The posterior mediastinum is bounded by the pericardium and trachea anteriorly and the vertebral column posteriorly.
Etiology of Mediastinal Masses
Adults
In adults, the most common causes of mediastinal masses vary by location (1, 2, 3):
Anterior (prevascular) mediastinum: Thymomas, benign cysts, and lymphomas (both Hodgkin and non-Hodgkin)
Middle (visceral) mediastinum: Benign cysts, lymph node enlargement (as in lymphoma, sarcoidosis, tuberculosis, lung cancer), and vascular masses
Posterior (paravertebral) mediastinum: Neurogenic tumors and esophageal abnormalities
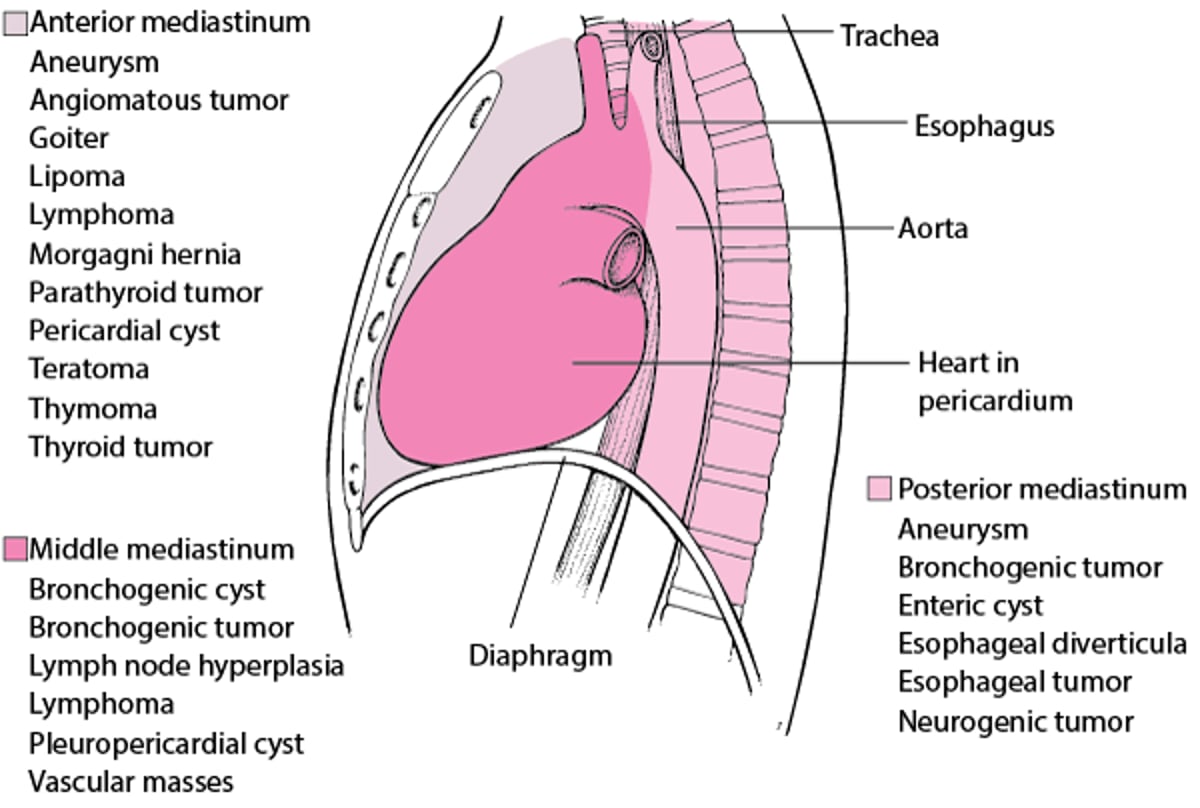
For other causes, see figure . Chronic fibrosing mediastinitis (eg, caused by tuberculosis, histoplasmosis) is a rare cause of mediastinal masses.
Some Causes of Mediastinal Masses in Adults

Children
In children, the most common mediastinal masses are neurogenic tumors and cysts. For other causes, see table .
Some Causes of Mediastinal Masses in Children
Location | Cause |
|---|---|
Anterior (prevascular) | Ectopic thyroid Sarcoma Teratoma Thymic lesions |
Middle (visceral) | Bronchogenic cyst Cardiac tumor Cystic hygroma Lymphadenopathy (due to infection, malignancy, or inflammation) Lymphoma Pericardial cyst Vascular abnormalities |
Posterior (paravertebral) | Esophageal duplication Meningomyelocele Neuroenteric abnormalities Neurogenic tumors |
Data from Biko DM, Lichtenberger JP 3rd, Rapp JB, Khwaja A, Huppmann AR, Chung EM. Mediastinal Masses in Children: Radiologic-Pathologic Correlation [published correction appears in Radiographics 2021 Sep-Oct;41(5):E164. doi: 10.1148/rg.2021219008]. Radiographic 2021;41(4):1186-1207. doi:10.1148/rg.2021200180 and Gerber TS, Porubsky S. Benign lesions of the mediastinum. Histopathology 2024;84(1):183-195. doi:10.1111/his.15088 | |
Etiology references
1. Gerber TS, Porubsky S. Benign lesions of the mediastinum. Histopathology 2024;84(1):183-195. doi:10.1111/his.15088
2. Jiang Y, Lin Y, Yang C, et al. Spatiotemporal distribution of mediastinal neoplasms: A comprehensive multi-center study. Lung Cancer 2024;191:107558. doi:10.1016/j.lungcan.2024.107558
3. Roden AC, Fang W, Shen Y, et al. Distribution of Mediastinal Lesions Across Multi-Institutional, International, Radiology Databases. J Thorac Oncol 2020;15(4):568-579. doi:10.1016/j.jtho.2019.12.108
Symptoms and Signs of Mediastinal Masses
Many mediastinal masses are asymptomatic. In general, malignant lesions and masses in children are much more likely to cause symptoms. The most common symptoms are chest pain and weight loss. Lymphomas may manifest with fever and weight loss.
In children, mediastinal masses are more likely to cause tracheobronchial compression and stridor or symptoms of recurrent bronchitis or pneumonia.
Symptoms and signs also depend on location. Large anterior mediastinal masses may cause dyspnea when patients are lying supine. Lesions in the middle mediastinum may compress blood vessels or airways, causing the superior vena cava syndrome or airway obstruction. Lesions in the posterior mediastinum may encroach on the esophagus, causing dysphagia or odynophagia.
Diagnosis of Mediastinal Masses
Chest radiograph
CT and sometimes MRI
Sometimes tissue examination
Mediastinal masses are most often incidentally discovered on chest radiograph or other imaging tests during an examination for chest symptoms. Additional diagnostic testing, usually imaging and biopsy, is indicated to determine etiology.
CT with IV contrast is the most valuable imaging technique. With thoracic CT, normal variants and benign tumors, such as fat- and fluid-filled cysts, can be distinguished from other processes. An MRI is performed if the structure is cystic. MRI may be useful in determining whether the mass is compressing or invading adjacent structures.
A definitive diagnosis can be obtained for many mediastinal masses with needle aspiration or needle biopsy. Fine-needle aspiration techniques usually suffice for carcinomatous lesions, but a cutting-needle biopsy should be performed to provide sufficient tissue for diagnostic analysis whenever lymphoma, thymoma, or a neural mass is suspected.
If ectopic thyroid tissue is considered a cause, thyroid-stimulating hormone is measured.
Surgical excision is performed when there is high suspicion of malignancy based on results of imaging or other tests and when complete resection can be achieved.
Treatment of Mediastinal Masses
Depends on cause
Treatment depends on etiology.
Some benign lesions, such as pericardial cysts, can be observed. Most malignant tumors should be removed surgically, but some, such as lymphomas, are best treated with chemotherapy.
Granulomatous disease such as tuberculosis or histoplasmosis should be treated with the appropriate antimicrobial medication.
Airway management in patients, particularly children, with anterior mediastinal masses requires caution, planning, and expertise. Because both airway compression and hemodynamic status can worsen when supine, especially with sedation, traditional anesthetic and airway management practices may be dangerous (1). Patients may be transported to definitive care awake and upright. Procedures such as biopsy are performed with minimal sedation while the patient is in an upright or semi-upright position. When definitive airway management is required, intubation is often performed in patients who are awake, and spontaneous ventilation is maintained.
Treatment reference
1. Blank RS, de Souza DG. Anesthetic management of patients with an anterior mediastinal mass: continuing professional development. Can J Anaesth 2011;58(9):853-867. doi:10.1007/s12630-011-9539-x
Key Points
In adults, thymomas, benign cysts, and lymphomas (both Hodgkin and non-Hodgkin) are the most common anterior lesions; benign cysts, lymph node enlargement, and vascular masses are the most common middle lesions; and neurogenic tumors and esophageal abnormalities are the most common posterior lesions.
In children, the most common mediastinal masses are neurogenic tumors, lymphomas, germ cell tumors, and cysts.
The most common symptoms are chest pain and weight loss, but many masses are asymptomatic.
Obstructive respiratory symptoms and systemic symptoms can occur in children and rarely in adults.
CT with IV contrast is the most valuable imaging technique.
Treatment depends on the etiology of the mass.





