



Deep vein thrombosis is the formation of blood clots (thrombi) in the deep veins, usually in the legs.
Blood clots may form in veins if the vein is injured, a disease makes the blood more likely to clot, or something slows the return of blood to the heart.
Blood clots may cause the leg or arm to swell.
A blood clot in a deep vein can break loose and travel to the lungs, which is called a pulmonary embolism.
Doppler ultrasound and blood tests are used to detect deep vein thrombosis.
Anticoagulants are given to prevent clot enlargement and prevent pulmonary embolism.
There are 2 main types of veins, superficial and deep. Superficial veins are located in the fatty layer under the skin. Deep veins are located in the muscles and along the bones. (See also Overview of the Venous System.)
Blood clots (thrombi) can occur in the deep veins, called deep vein thrombosis, or in the superficial veins called superficial venous thrombosis. The superficial veins are usually also inflamed but without clotting (thrombosis), the combination of clotting and inflammation is referred to as superficial thrombophlebitis.
The term venous thromboembolism (VTE) can refers to the blood in a vein, or a clot that breaks free into the bloodstream, usually traveling to the lungs (pulmonary embolism). Because almost any clot (thrombus) can break loose and become an embolism, doctors sometimes refer to deep vein thrombosis as thromboembolic disease.
Deep vein thrombosis occurs most often in the legs or pelvis but may also occasionally develop in the arms.


Causes of Deep Vein Thrombosis
Three main factors can contribute to deep vein thrombosis:
Injury to the vein’s lining
An increased tendency for blood to clot
Slowing of blood flow
Injury to the vein
Veins may be damaged during surgery or during an injury to an arm or leg, by the injection of irritating substances, by inflammation, or by certain disorders, such as thromboangiitis obliterans. They may also be injured by a clot, making formation of a second clot more likely.
Increased blood clotting tendency
Some diseases, such as cancer and inherited disorders of blood clotting, cause blood to clot when it should not. Some medications, including oral contraceptives, estrogen therapy, or medications that act like estrogen (such as tamoxifen and raloxifene), can cause blood to clot more readily. Smoking also increases the tendency of blood to clot. Sometimes blood clots more readily after childbirth or surgery. Among older adults, dehydration commonly causes the blood to clot more readily and can therefore contribute to deep vein thrombosis.(such as tamoxifen and raloxifene), can cause blood to clot more readily. Smoking also increases the tendency of blood to clot. Sometimes blood clots more readily after childbirth or surgery. Among older adults, dehydration commonly causes the blood to clot more readily and can therefore contribute to deep vein thrombosis.
Slowing of blood flow
During prolonged bed rest and other occasions when the legs are not moving normally, blood flow slows because the person is lying down and the calf muscles are not contracting and squeezing the blood toward the heart. For example, deep vein thrombosis may develop in people who have had a heart attack or other serious disorder (such as heart failure, chronic obstructive pulmonary disease [COPD], or a stroke) and lie in a hospital bed for several days without sufficiently moving their legs or in people whose legs and lower body are paralyzed (paraplegia). Deep vein thrombosis can develop after major surgery, particularly pelvic, hip, or knee surgery. Thrombosis can even occur in healthy people who sit for long periods, for example, during long drives or airplane flights, but thrombosis is uncommon in this circumstance and usually occurs in people with other risk factors.
Did You Know...
|
Complications of Deep Vein Thrombosis
Although deep vein thrombosis is uncomfortable, the main concern is with the complications, including:
Chronic venous insufficiency, causing long-term leg swelling, pain, and leg ulcers
Lack of blood flow (ischemia) to the leg, causing massive swelling and pain (a rare complication)
Pulmonary embolism
In people who have deep vein thrombosis, a blood clot may break loose from an affected vein in the leg. A clot that breaks loose is called an embolus. The embolus can travel through the bloodstream, through the heart, and into the lungs, where it lodges in a blood vessel, blocking blood flow to a portion of the lung. This blockage is called pulmonary embolism and can be fatal, depending on how large the embolus is and the size of the blocked lung artery. Generally, only thrombi in the deep veins are potentially dangerous if they break off and travel to the lungs; the small blood clots that occur in superficial venous thrombosis usually do not become emboli.
Blood clots in the legs or pelvis are more likely to become emboli than blood clots in the arms, perhaps because the squeezing action of the calf and leg muscles can dislodge them.
The consequences of pulmonary embolism depend on the size and number of emboli:
A small embolus may block a small artery in the lungs, causing the death of a small piece of lung tissue (called pulmonary infarction).
A large pulmonary embolus can block all or nearly all of the blood traveling from the right side of the heart to the lungs, leading to low blood pressure and low oxygen levels and quickly causing death.
Large emboli are not common, but no one can predict which case of deep vein thrombosis, if untreated, will lead to a large embolus.
Multiple emboli may occur. Multiple emboli typically go to different parts of the lungs.
Sometimes, people have an abnormal opening between the right and left upper chambers of the heart (the atria), called a patent foramen ovale . If this opening is present, an embolus can pass into the arterial circulation and block an artery in another part of the body, such as the brain where it will cause a stroke.
Chronic venous insufficiency
Some blood clots heal by being converted to scar tissue, which may damage the valves in the veins. The damaged valves prevent the veins from functioning normally, a disorder called chronic venous insufficiency. In this disorder, fluid accumulates (a condition called edema) and the ankle and sometimes lower leg swells. The skin can become scaly, itchy, and reddish brown on light skin or purple and/or brown on dark skin. Sometimes open sores (ulcers) can develop in the leg, ankle, or foot.
Ischemia (lack of blood flow)
Rarely, a very large blood clot in a leg causes so much swelling that it blocks the blood flow through the leg. The leg becomes pale or blue and extremely painful. Gangrene (dead tissue) can develop if the blood flow is not restored.
Infection
Infection can develop in venous clots, although it is rare. A bacterial infection of the internal jugular vein and surrounding tissues in the neck, called jugular vein suppurative thrombophlebitis or Lemierre syndrome, may follow an infection of the tonsils. Blood clots may develop in the pelvis after childbirth and become infected, causing fever. Infection and clotting of a superficial vein, called suppurative or septic thrombophlebitis, is usually caused by placement of an IV.
Symptoms of Deep Vein Thrombosis
Many people with deep vein thrombosis have no symptoms at all. In other people, if a deep leg vein is involved, the calf swells and may be painful, tender to the touch, and warm. The ankle, foot, or thigh may also swell, depending on which veins are involved. Similarly, if an arm vein is involved, the arm may swell.
When a pulmonary embolism occurs, chest pain or shortness of breath may be the first indication that a blood clot is present.
Diagnosis of Deep Vein Thrombosis
Doppler ultrasound
Blood tests to measure D-dimer
Deep vein thrombosis may be difficult for doctors to detect, especially when pain and swelling are absent or very slight. When this disorder is suspected, Doppler ultrasound is used to confirm the diagnosis.
Sometimes doctors also do a blood test to measure a substance called D-dimer that is released from blood clots. If the level of D-dimer in the blood is not increased, the person probably does not have deep vein thrombosis.

If the person has symptoms of pulmonary embolism, computed tomography (CT) angiography or, rarely, nuclear lung scanning using a radioactive marker, is done to detect pulmonary embolism. Doppler ultrasound is done to check the legs for clots, if it was not done already. When a person collapses due to very low blood pressure or very low oxygen levels from a massive pulmonary embolism, immediate treatment is required, and there may not be time for testing.
Sometimes other tests are needed to determine the cause of deep vein thrombosis, such as cancer or other disease that causes blood clots.
Treatment of Deep Vein Thrombosis
Anticoagulant medications (sometimes called blood thinners)
Sometimes, clot-dissolving medications, clot-blocking filter, or surgery
For deep vein thrombosis, a doctor’s main goal is to prevent pulmonary embolism. Preventing post-thrombotic syndrome is also important. Hospitalization may be necessary at first, but most people with deep vein thrombosis can be treated at home. Bed rest is unnecessary except to help relieve symptoms. People may be as active as they want. Physical activity does not increase the risk that a blood clot will break loose and cause a pulmonary embolism.
Treatment usually consists of:
Anticoagulant medications (most common)
Clot-dissolving medications
Rarely, a clot-blocking filter
Did You Know...
|
Anticoagulant medications
Anticoagulants are sometimes called blood thinners. They decrease the blood’s ability to clot, so they can prevent new clots from forming and can stop existing clots from getting bigger. They do not break up or dissolve clots that have already formed. Almost all people with deep venous thrombosis are given anticoagulants. However, use of anticoagulants increases the risk of bleeding, both internally and externally, so doctors take the individual person's risk of bleeding into account when recommending specific anticoagulant medications for blood clots.
Doctors usually use an injectable heparin (either a low molecular weight Doctors usually use an injectable heparin (either a low molecular weightheparin such as enoxaparin, or regular "unfractionated" such as enoxaparin, or regular "unfractionated"heparin) or fondaparinux, also given by injection under the skin (subcutaneously), followed by longer term treatment with an anticoagulant medication that can be taken by mouth. The injectable medications work immediately. In some cases, people continue taking the injectable medication and do not start an oral medication at all. ) or fondaparinux, also given by injection under the skin (subcutaneously), followed by longer term treatment with an anticoagulant medication that can be taken by mouth. The injectable medications work immediately. In some cases, people continue taking the injectable medication and do not start an oral medication at all.
When an oral medicine is used, it may be a direct oral anticoagulant (DOAC), which include rivaroxaban, apixaban, edoxaban, and dabigatran; or warfarin. DOACs and When an oral medicine is used, it may be a direct oral anticoagulant (DOAC), which include rivaroxaban, apixaban, edoxaban, and dabigatran; or warfarin. DOACs andwarfarin work equally well, but warfarin requires periodic blood tests to monitor its effectiveness and often takes longer to become effective. DOACs, on the other hand, are generally more expensive. For people whose clots are thought to be related to cancer, many doctors prefer to use the injectable medications or a DOAC rather than warfarin. Several days of treatment with the injectables are needed before starting some of the DOACs.
The effect of DOACs on people's blood is more predictable than the effect of warfarin. Therefore, people taking DOACs do not need to have frequent blood tests to adjust the dose. Also, DOACs tend to cause fewer episodes of serious bleeding than warfarin. However, bleeding caused by DOACs can be harder to stop because antidotes for these medications are not as widely available as antidotes for warfarin.
If people are going to use warfarin, it takes several days to be fully effective, and the person must start taking it while still receiving the injectable anticoagulant. Once the warfarin has taken effect, people stop taking the injectable medication.
People taking warfarin must have periodic blood tests to see how much their blood is anticoagulated. Doctors then use the blood test result to adjust the dose of warfarin. The blood tests are usually done once or twice a week for 1 or 2 months, and then every 4 to 6 weeks thereafter.
Many different medications and foods change how the body breaks down warfarin (see also Drug Interactions). Some medications and foods increase its breakdown, making a warfarin dose less effective and increasing the risk of another blood clot. Other medications and foods slow warfarin's breakdown, making a dose more effective but also more likely to cause bleeding. Some people are also more sensitive to warfarin and may need warfarin-sensitivity testing to help doctors adjust their levels.
How long people continue anticoagulants (with DOACs, warfarin, or an injectable medication) varies according to the degree of risk. People whose deep vein thrombosis resulted from a specific, temporary cause (such as surgery or a medication they have stopped taking) usually continue anticoagulants for 3 to 6 months. When a specific cause is not found, the cause is not temporary (for example, a blood clotting disorder), or people have had 2 or more episodes of deep vein thrombosis, people are usually on anticoagulants for a longer period of time (sometimes for the rest of their life).
Excessive bleeding, which may be life-threatening, is the most common complication of anticoagulants. Risk factors for excessive bleeding include being age 65 years or older or having:
A recent heart attack, stroke, or bleeding in the digestive tract
A low platelet count (because platelets help blood clot)
Cancer
For people who are taking warfarin, doctors can give vitamin K, transfusions of plasma (which contains clotting factors), or prothrombin complex concentrate to reverse the effects of the For people who are taking warfarin, doctors can give vitamin K, transfusions of plasma (which contains clotting factors), or prothrombin complex concentrate to reverse the effects of thewarfarin and stop the bleeding. For people who are taking heparin, doctors can give protamine to partially reverse the effects.and stop the bleeding. For people who are taking heparin, doctors can give protamine to partially reverse the effects.
For people taking some of the DOACs, doctors can give andexanet alfa or prothrombin complex concentrate to reverse the effects of the DOACs and stop the bleeding.
Clot-blocking filter
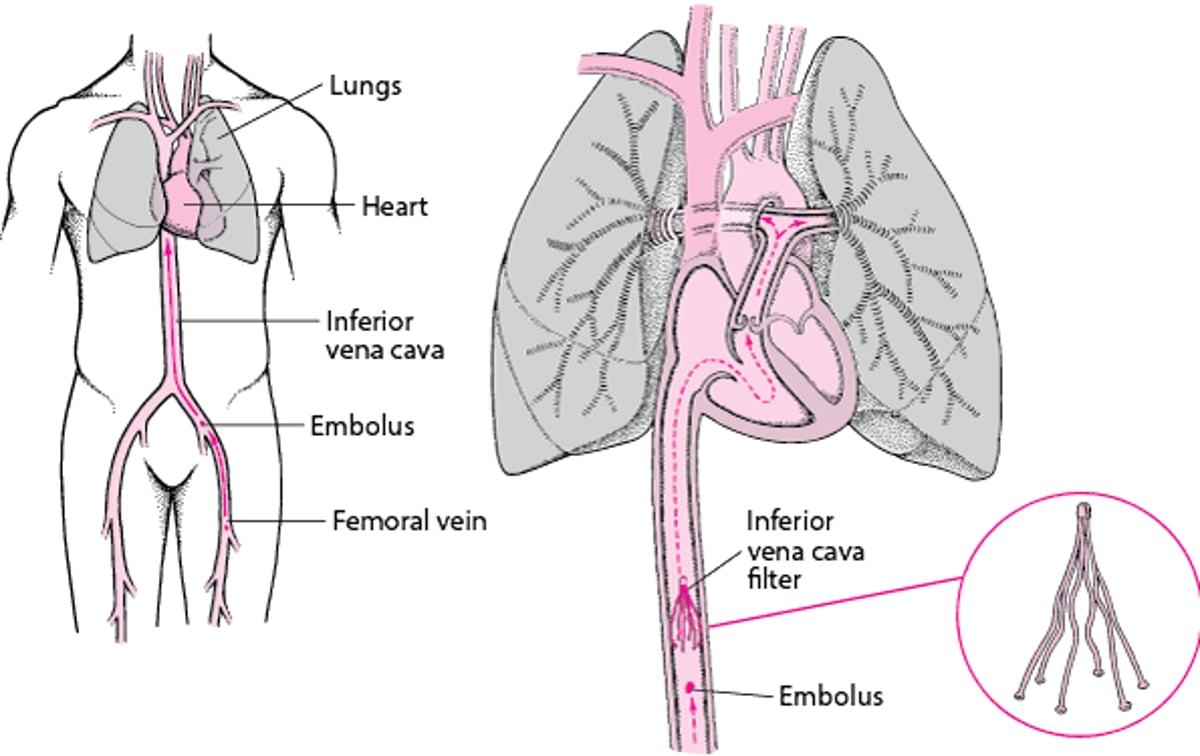
Very rarely, as an alternative to anticoagulants, doctors place a filter (formerly called an umbrella) inside a large vein between the heart and the area affected by deep vein thrombosis, usually the inferior vena cava. The inferior vena cava is a large vein that returns blood to the heart from the lower part of the body. The filter can trap emboli, preventing them from reaching the lungs.
However, unlike anticoagulants, filters do not prevent new clots from forming. Filters are usually reserved for people in whom anticoagulant therapy is not possible.
Inferior Vena Cava Filters: One Way to Prevent Pulmonary Embolism in People who Cannot Take Anticoagulants
In people who have deep vein thrombosis, a blood clot may break loose from an affected vein in the leg and travel through the bloodstream. A clot that breaks loose is called an embolus. The embolus travels toward the heart and passes through the right atrium and ventricle and into one of the pulmonary arteries, which carry blood to the lungs. The clot may lodge in an artery in a lung and block blood flow, resulting in pulmonary embolism. Pulmonary embolism may be life threatening, depending on how large the embolus is and the size of the blocked artery. To prevent pulmonary embolism, doctors usually use medications that limit blood clotting (anticoagulants, or blood thinners). However, for some people, doctors may recommend that a filter be temporarily or permanently placed in the inferior vena cava. The inferior vena cava is a large vein that returns blood to the heart from the lower part of the body. The filter typically is recommended when anticoagulants cannot be used, for example, when a person is also having bleeding. The filter can trap emboli before they reach the heart but allow blood to flow through freely. Emboli that are trapped sometimes dissolve on their own. However, filters do not completely eliminate the risk of emboli. Sometimes other veins from the legs enlarge, allowing blood and emboli to bypass the filter. Also, filters can break loose or become blocked by a clot. Filters are much less effective at preventing pulmonary embolism than treatment with anticoagulants. |

Clot-dissolving medications
Doctors only occasionally use intravenous medications, such as alteplase, to dissolve venous blood clots. These medications (also called thrombolytic, fibrinolytic, or clot-busting drugs) may be given to a person with extensive blood clots. When they are used, usually a catheter is placed into the vein so the medicine can be directed into the clot. Clot-dissolving medications have a higher risk of bleeding complications.Doctors only occasionally use intravenous medications, such as alteplase, to dissolve venous blood clots. These medications (also called thrombolytic, fibrinolytic, or clot-busting drugs) may be given to a person with extensive blood clots. When they are used, usually a catheter is placed into the vein so the medicine can be directed into the clot. Clot-dissolving medications have a higher risk of bleeding complications.
Doctors sometimes use clot-dissolving medications in combination with mechanical removal methods in people who have large clots in their upper leg. In such cases, doctors may put a small, flexible tube (catheter) into the blocked vein, remove as much clot as possible with an instrument, and then administer the clot-dissolving medication through the catheter.
Treatment of complications
If pulmonary embolism occurs, treatment usually includes oxygen (usually given by a face mask or nasal prongs), analgesics to relieve pain, and anticoagulants. If pulmonary embolism is life threatening, clot-dissolving medications are given or surgery is done to remove the embolus.
In many cases, the veins never completely recover after deep vein thrombosis develops. Elastic compression stockings worn below the knee may be helpful if chronic venous insufficiency develops. Treatment of this condition, and the painful skin ulcers (venous stasis ulcers) that can develop with it, are discussed in Post-Thrombotic Syndrome.
Prevention of Deep Vein Thrombosis
Although the risk of deep vein thrombosis cannot be entirely eliminated, it can be reduced in several ways:
Keeping people as mobile as possible and minimizing bedrest
Anticoagulant medications
Intermittent pneumatic compression devices
Preventive measures are selected depending on the person's risk factors and individual characteristics.
People at low risk of deep vein thrombosis, such as those who must be temporarily inactive for long periods, as during an airplane flight, and those who are undergoing minor surgery but have no other risk factors for deep vein thrombosis, can take simple measures. Such people should elevate their legs, flex and extend their ankles about 10 times every 30 minutes, and walk and stretch every 2 hours while awake during long flights.
People at higher risk of deep vein thrombosis require additional preventive treatment. Such people include:
People undergoing minor surgery who have specific risk factors for deep vein thrombosis (for example, old age, cancer or excessive blood clotting)
People without risk factors undergoing major surgery (especially orthopedic surgery like a hip or knee replacement or repair of a hip fracture)
People who are hospitalized with a serious illness (for example a heart attack or serious injury)
Such higher risk people should keep their legs elevated and begin moving around and walking as soon as possible. Additionally, anticoagulants, such as low-molecular weight heparin or a direct oral anticoagulant, are often used. These medications help prevent deep vein thrombosis by reducing the blood's ability to clot but have a slight risk of causing excessive bleeding.
Intermittent pneumatic compression (IPC) uses a pump to repeatedly inflate and deflate hollow plastic leggings. The leggings squeeze the calves and empty the veins to prevent clots. The leggings may be used in combination with anticoagulants or instead of anticoagulants in people with a high risk of bleeding, such as those who had a serious injury. In people having surgery that has a high risk of bleeding, the leggings are put on before surgery and kept on during and after surgery, until the person can walk again.
Continuously wearing high-compression elastic stockings (support hose) makes the veins narrow slightly and the blood flow more rapidly. As a result, clotting may be less likely. However, elastic stockings alone are not sufficient protection against developing deep vein thrombosis. Also, they may give a false sense of security and discourage more effective methods of prevention. If not worn correctly, they may bunch up and aggravate the problem by blocking blood flow in the legs.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
Drug Information for the Topic





