

"Numbness" can be used by patients to describe various symptoms, including loss of sensation, abnormal sensations, weakness, or paralysis. However, numbness in the clinical context refers to loss of sensation, either partial (hypesthesia) or complete (anesthesia). Clinicians must determine exactly what patients mean when they use the term numbness.
Numbness may involve some or all of the 3 major sensory modalities:
Light touch
Pain and temperature sensation
Position and vibration sensation
Touch abnormality may also involve fine touch (discriminative touch), which often is affected by disturbances in the central nervous system (CNS)—for example, the ability to identify an object such as a key or coin by handling it or to perceive and identify numbers written on the palm of the hand.
Numbness is often accompanied by abnormal sensations of tingling ("pins-and-needles" or paresthesias) unrelated to a sensory stimulus.
Depending on the cause, numbness may be accompanied by other neurologic manifestations (eg, pain, extremity weakness, nonsensory cranial nerve dysfunction). Numbness may be transient , often due to localized positional nerve compression, or ongoing (chronic), due to more intense nerve damage. The onset may be acute, following a brief compression (eg, sleeping on it), trauma, or ischemia; or numbness may come on subacutely, often pointing to an underlying condition (eg, diabetes and diabetic neuropathy).
Adverse effects of chronic numbness include:
Difficulty walking and driving
Difficulty with balance, leading to increased risk of falls
Difficulty sleeping
In addition, numbness may interfere with recognition of wounds, skin infections, diabetic foot ulcers, and other injuries, leading to delayed treatment.
Pathophysiology of Numbness
Anatomy
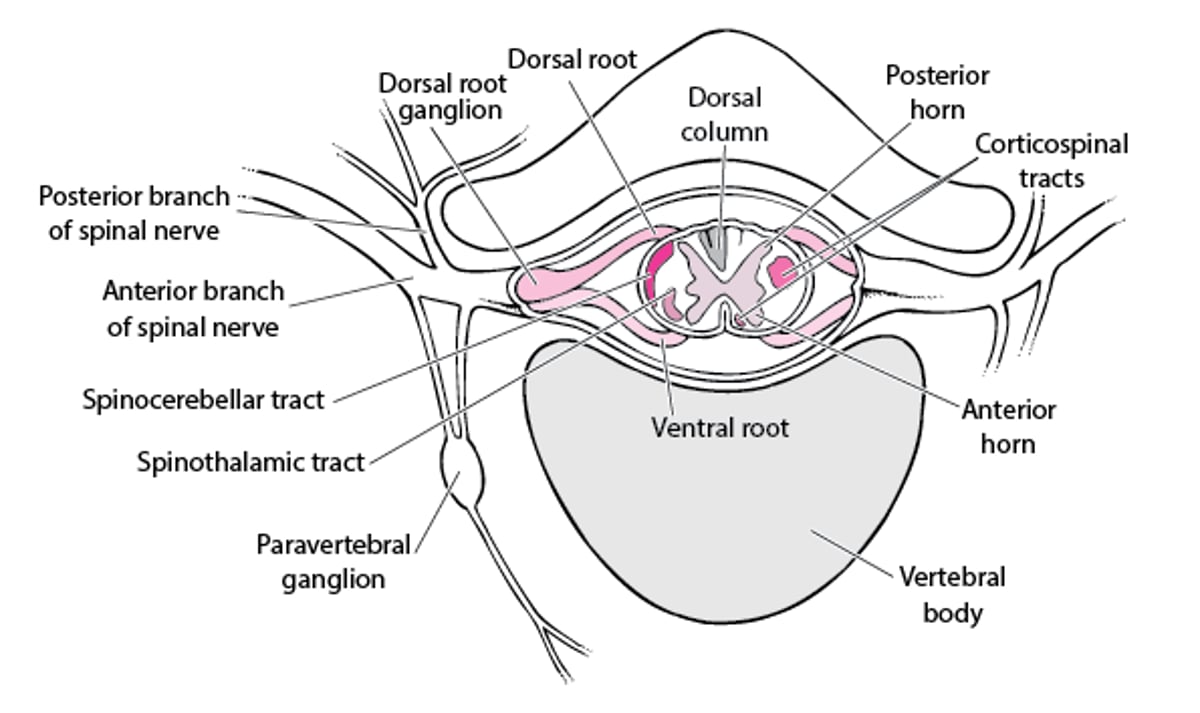
Sensory processing areas within the brain connect with cranial nerves or spinal cord sensory pathways. Sensory fibers exiting the spinal cord join just outside the cord to form dorsal nerve roots (except for C1—see figure ). These 30 dorsal sensory roots join with corresponding motor ventral roots to form spinal nerves. Branches of the cervical and lumbosacral spinal nerves join more distally to form plexuses and then branch into nerve trunks. The intercostal nerves do not form plexuses; these nerves correspond to their segment of origin in the spinal cord. The term peripheral nerve refers to the part of the nerve distal to the nerve root and plexus.
Spinal Nerve

Nerve roots from the most distal spinal cord segments descend within the spinal column below the end of the spinal cord, forming the cauda equina. The cauda equina supplies sensation to the legs and the pubic, perineal, and sacral areas (saddle area).
The spinal cord is divided into functional segments (levels) that correspond approximately to the attachments of the pairs of spinal nerve roots. The area of skin supplied mostly by a particular spinal nerve is the dermatome corresponding to that spinal segment (see figure ).
Sensory Dermatomes


Mechanisms
Numbness can occur from dysfunction anywhere along the pathway from the sensory receptors up to and including the cerebral cortex. Common mechanisms include the following:
Ischemia (eg, brain infarction, spinal cord infarction, vasculitis)
Demyelinating disorders (eg, multiple sclerosis, Guillain-Barré syndrome)
Mechanical nerve compression (eg, by tumors, a herniated disk [nucleus pulposus], or entrapment of a peripheral nerve as in carpal tunnel syndrome)
Toxins or medications (eg, heavy metals, certain chemotherapy agents)
Metabolic disorders (eg, diabetes, chronic kidney disease, thiamin deficiency, vitamin B12 deficiency)
Immune-mediated disorders (eg, postinfectious inflammation, such as transverse myelitis)
Degenerative disorders (eg, hereditary neuropathies)
Etiology of Numbness
There are many causes of numbness. Although there is some overlap, dividing the causes based on the pattern of numbness can be helpful (see table ).
Some Causes of Numbness
Cause | Suggestive Findings | Diagnostic Approach* |
|---|---|---|
Unilateral numbness of both limbs† | ||
Cortical dysfunction (eg, stroke, tumor, multiple sclerosis, degenerative brain disorders) | Facial and body sensations lost on the side contralateral to the lesion, plus loss of cortical sensation (eg, agraphesthesia, astereognosis, extinction) Usually nonsensory neurologic deficits (eg, weakness, hyperreflexia, ataxia) | MRI or CT |
Upper brain stem or thalamus dysfunction (eg, stroke, tumor, abscess) | Facial and body sensations lost on the side contralateral to the lesion Often cranial nerve deficits (eg, oculomotor nerve palsy on the side opposite the numbness in some upper brain stem strokes) | MRI (preferred for brain stem dysfunction) or CT |
Lower brain stem dysfunction (eg, stroke, tumor, degenerative brain disorders) | Facial sensations lost on the side ipsilateral to the lesion and body sensations lost on the side contralateral to the lesion (crossed face-body distribution) Often cranial nerve deficits | MRI |
Bilateral numbness of the limbs or trunk | ||
Transverse myelopathy‡ (eg, spinal cord compression, transverse myelitis) | Loss of sensory, motor, and reflex function below a specific spinal segment Autonomic dysfunction (eg, bowel, bladder, and erectile dysfunction; anhidrosis) | MRI |
Dorsal column spinal cord dysfunction (eg, multiple sclerosis, vitamin B12 deficiency, tabes dorsalis, HIV infection) | Disproportionate loss of vibration and position sensation In multiple sclerosis, or other conditions that affect the posterior columns of the spinal cord (eg, B12 deficiency), numbness often described by the patient in a different way (ie, the limb feels thick or wrapped like wearing a glove or stockings) In vitamin B12 deficiency, bilateral and symmetric findings (usually due to spinal cord dysfunction but often accompanied by a peripheral neuropathy) | MRI Vitamin B12 level, CSF cell count and protein, CSF and blood tests for syphilis, blood tests for HIV infection Electromyography and nerve conduction testing (electrodiagnostic testing) |
Compression of the cauda equina—also called cauda equina syndrome† (eg, due to a herniated disk or spinal or vertebral metastases) | Numbness affecting primarily the perineum (saddle area) Often urinary or fecal retention or incontinence, and/or loss of sphincter reflexes (eg, anal wink, bulbocavernosus) | MRI |
Central cord syndrome (eg, due to trauma, tumor, or syrinx) | Numbness and weakness disproportionately affecting both upper limbs | MRI |
Polyneuropathies such as
| Bilateral, roughly symmetric, mostly distal (stocking-glove distribution) paresthesias and sensory deficits Sometimes weakness and hyporeflexia (eg, in demyelinating polyneuropathies) | Electrodiagnostic testing Laboratory testing based on suspected disorder |
Multiple mononeuropathy—also called mononeuritis multiplex (eg, associated with diabetes, systemic rheumatic diseases, infection, or metabolic disorders) | Numbness with or without pain Usually motor and reflex deficits in the distribution of ≥ 2 peripheral nerves, sometimes affecting specific nerves sequentially (but may be clinically indistinguishable from stocking-glove distribution) | Usually electrodiagnostic testing and laboratory testing based on suspected disorder |
Numbness of part of a single limb | ||
Radiculopathy§ (eg, a herniated disk, bone compression due to osteoarthritis or rheumatoid arthritis, carcinomatous meningitis, infectious radiculopathy) | Pain (sometimes like an electric shock), sensory and often motor and/or reflex deficits in a nerve root distribution (see table ) Pain possibly worsened by moving the spine or a Valsalva maneuver | MRI or CT Sometimes electrodiagnostic testing |
Plexopathy (eg, brachial or lumbar plexopathy, brachial neuritis, thoracic outlet compression syndrome) | Sensory deficits, pain, and motor deficits in part of a limb (sometimes most of a limb) in a distribution larger than that caused by radiculopathy or single mononeuropathy | Electrodiagnostic testing MRI unless the cause is trauma or suspected brachial neuritis |
Single mononeuropathy (eg, carpal, cubital, radial, and tarsal tunnel syndromes; ulnar, radial, and peroneal nerve palsies) | Numbness (with or without pain) and motor and reflex deficits in the distribution of a single peripheral nerve | Sometimes history and physical examination alone Sometimes electrodiagnostic testing |
* Clinical examination is always done but is mentioned in this column only when that can be the sole means of diagnosis. | ||
† Only a single entire limb may be affected; the trunk may be affected. | ||
‡ Conus medullaris syndrome is a transverse myelopathy at about the L1 level. Findings are similar to those of cauda equina syndrome. | ||
§ Findings may be bilateral. | ||
CSF = cerebrospinal fluid. | ||
Evaluation of Numbness
Because so many disorders can cause numbness, a sequential evaluation is done.
First, the distribution of numbness is used to localize the part of the nervous system that is involved.
Then, other clinical features—particularly rate of onset, regularity of symptoms (intermittent or persistent), associated neurologic symptoms and signs, and symmetry—further narrow the differential diagnosis and guide additional questions and tests to diagnose specific causative disorders.
Although in practice certain elements of the history are typically asked selectively (eg, patients with a typical stroke syndrome are not usually asked at length about risk factors for polyneuropathy and vice versa), many of the potentially relevant components of the history are presented here for informational purposes.
History
History of present illness should include using an open-ended question to ask patients to describe numbness. Symptom onset, duration, and time course should be ascertained. Most important are:
The location of numbness (numbness, described as "tightness" in multiple sclerosis, may feel like one is wearing socks, which is a feature of posterior spinal cord involvement)
Associated neurologic symptoms (eg, paresis, dysesthesias, sphincter dysfunction such as incontinence or retention, dysphasia, visual loss, diplopia, dysphagia, cognitive decline)
Possible precipitating causes (eg, compression of an extremity, trauma, recent intoxication, sleeping in an awkward position, symptoms of infection) are sought. Increased body temperature may bring on numbness in patients with multiple sclerosis (Uhthoff phenomenon), that may resolve with cooling.
Review of systems should identify symptoms of causative disorders. Some examples are:
Back and/or neck pain: Osteoarthritis-associated herniated disk or spinal cord compression
Fever, rash, or both: Infectious neuropathy, infectious radiculopathy, brain infection, or systemic rheumatic diseases
Headache: Brain tumor, stroke, or encephalopathy
Joint pain: Systemic rheumatic diseases
Vegan diet or pernicious anemia: Vitamin B12 deficiency
Excessive intake of high-mercury seafood: Toxic polyneuropathy
History of alcohol use disorder
Past medical history should identify known conditions that can cause numbness, particularly the following:
Diabetes, chronic kidney disease, liver disease, or thyroid disease: Polyneuropathy
Infections such as HIV, syphilis, or Lyme disease: Infectious peripheral neuropathy or brain infection
Coronary artery disease, atrial fibrillation, atherosclerosis, or smoking: Stroke
Cancer (particularly lung cancer): Paraneoplastic anti-Hu subacute sensory or motor neuropathy
Osteoarthritis or rheumatoid arthritis: Radiculopathy
Family history should include information about any familial neurologic disorders. Medication and drinking history should include use of all medications and substances and occupational exposures to toxins. For example, B6 (pyridoxine) supplements, when taken in excess, can cause a crippling loss of body sensations.Family history should include information about any familial neurologic disorders. Medication and drinking history should include use of all medications and substances and occupational exposures to toxins. For example, B6 (pyridoxine) supplements, when taken in excess, can cause a crippling loss of body sensations.
Physical examination
A complete neurologic examination is done, emphasizing the location and neurologic territories of deficits in reflex, motor, and sensory function. In general, reflex testing is the most objective examination, and sensory testing is the most subjective; often, the area of sensory loss cannot be precisely defined. The most subjective but clinically important finding is the affected sensory level, which could point to a specific area of the spinal cord.
Red flags
In patients with numbness, the following findings are of particular concern:
Sudden onset (eg, within minutes or hours) of numbness
Sudden or rapid onset (eg, within hours or days) of accompanying weakness
Onset only with increased body temperature (exercise, fever, hot baths) indicative of Uhthoff phenomenon
Dyspnea
Signs of cauda equina or conus medullaris syndrome (eg, saddle anesthesia, incontinence, loss of anal wink reflex)
Bilateral neurologic deficits below a spinal segment
Loss of sensation on both the face and body (on the same side or opposite side of the body)
Numbness of an entire limb
Interpretation of findings
The anatomic pattern of symptoms suggests the location of the lesion but is often not specific. In general:
Numbness of part of one limb: Peripheral nervous system lesion
Hemibody numbness (with or without the trunk): Brain lesion
Bilateral numbness below a specific dermatomal level: Transverse myelopathy (a spinal cord lesion)
Bilateral numbness not corresponding to a specific dermatomal level: Polyneuropathy, multiple mononeuropathy, or a patchy spinal cord or brain disorder
More specific localizing patterns include the following:
Stocking-glove distribution: When motor signs are minimal or absent, usually an axonal polyneuropathy; when accompanied by weakness and spasticity (eg, hyperreflexia, increased tone, extensor plantar response), sometimes cervical spondylosis or a demyelinating polyneuropathy or demyelinating lesion of the spinal cord
Single dermatomal distribution: Nerve root lesion (radiculopathy)
Single extremity with more than one nerve or nerve root affected: Plexus lesion (plexopathy)
Multiple related or unrelated peripheral nerves: Multiple mononeuropathy
Loss of sensation affecting position and vibration disproportionately: Dysfunction of the dorsal columns or a demyelinating peripheral neuropathy
Saddle area distribution: Conus medullaris syndrome or compression of the cauda equina (cauda equina syndrome)
Crossed face-body distribution (ie, face and body affected on different sides): Lower brain stem lesion
Ipsilateral face and body distribution: Upper brain stem, thalamic, or cortical lesion
Bilateral numbness in a cape-like distribution over the neck and shoulders: Central cervical spinal cord abnormality, typically a syrinx
Findings that indicate involvement of multiple anatomic areas (eg, both brain and spinal cord lesions) suggest more than one lesion (eg, multiple sclerosis, metastatic tumors, multifocal degenerative brain or spinal cord disorders) or more than one causative disorder.
The rate of symptom onset helps suggest likely pathophysiology:
Nearly instantaneous (usually seconds, occasionally minutes): Ischemic or traumatic
Hours to days: Infectious or toxic-metabolic or autoimmune (eg, multiple sclerosis)
Days to weeks: Infectious, toxic-metabolic, or immune-mediated
Weeks to months: Neoplastic, or degenerative, or occasionally infectious due to chronic central nervous system (CNS) infection (eg, fungal infection)
Degree of symmetry also provides clues:
Highly symmetric involvement: A systemic cause (eg, a metabolic, toxic, medication- or substance–related, infectious, or postinfectious cause; vitamin deficiency)
Clearly asymmetric involvement: A structural cause (eg, tumor, trauma, stroke, peripheral plexus or nerve compression, a focal or multifocal degenerative disorder)
After location of the lesion, rate of onset, and degree of symmetry have been determined, the list of potential specific diagnoses is much smaller, so that focusing on clinical features that differentiate among them is practical (see table ). For example, if initial evaluation suggests an axonal polyneuropathy, subsequent evaluation focuses on features of each of the many possible medications, toxins, and disorders that can cause these polyneuropathies.
Testing
Testing is required unless the diagnosis is clinically obvious and conservative treatment is elected (eg, in some cases of carpal tunnel syndrome, for a herniated disk or traumatic neuropraxia). Test selection is based on anatomic location of the suspected cause:
Peripheral nerves or nerve roots: Nerve conduction studies and electromyography (electrodiagnostic testing)
Plexuses: Nerve conduction studies and electromyography and sometimes contrast MRI
Brain or spinal cord: MRI
Electrodiagnostic tests can help differentiate between neuropathies and plexopathies (lesions distal to the nerve root) and more proximal lesions (eg, radiculopathies) and between types of polyneuropathies (eg, axonal and demyelinating, hereditary and acquired).
If clinical findings suggest a structural lesion of the brain or spinal cord or a radiculopathy, MRI is usually indicated. CT is usually a second choice but may be particularly helpful if MRI is not available soon enough (eg, in emergencies).
After the lesion is localized, subsequent testing can focus on specific disorders (eg, metabolic, infectious, toxic, autoimmune, or other systemic disorders). For example, if findings indicate a polyneuropathy, subsequent tests typically include complete blood count (CBC), electrolytes, renal function tests, rapid plasma reagin test, and measurement of fasting plasma glucose, hemoglobin A1C, vitamin B12, folate, thyroid-stimulating hormone, and usually serum immunoelectrophoresis and serum protein electrophoresis (particularly if the neuropathy is painful). Serum immunoelectrophoresis and serum protein electrophoresis can help diagnose multiple myeloma.
Treatment of Numbness
Treatment is directed at the disorder causing numbness. Other methods and medications (eg, those used to treat neuropathic pain) may help relieve symptoms.
Patients with insensitive feet, particularly if circulation is impaired, should take precautions to prevent and recognize injury. Socks and well-fitting shoes are needed when walking, and shoes must be inspected for hidden foreign material before wear. The feet should be inspected frequently for ulcers and signs of infection. Patients with insensitive hands or fingers must be alert when handling potentially hot or sharp objects.
Patients with diffuse sensory loss or loss of position sense should be referred to a physical therapist for gait training. Precautions to prevent falls should be taken.
Driving skill should be monitored.
Key Points
Use an open-ended question to ask patients to describe their numbness.
The anatomic pattern and time course of symptoms helps narrow the list of possible diagnoses.
If part of a limb is numb, suspect a peripheral nerve, plexus, or nerve root lesion.
If both limbs are numb on one side, with or without numbness of the trunk on the same side, suspect a brain lesion.
If patients have bilateral numbness below a specific spinal cord segment, particularly with motor and reflex deficits, suspect a transverse myelopathy.
If patients have bilateral numbness not corresponding to a spinal cord segment, suspect a polyneuropathy, multiple mononeuropathy, or a patchy spinal cord or brain lesion.
If numbness occurs in a stocking-glove distribution, suspect an axonal polyneuropathy.
If numbness occurs nearly instantaneously in the absence of trauma, suspect an acute ischemic event.
Consider electrodiagnostic testing for suspected peripheral nervous system causes and MRI for CNS causes.





