If no spontaneous respiration occurs after airway opening and no respiratory devices are available, rescue breathing (mouth-to-mask or mouth-to-barrier device) is started; mouth-to-mouth ventilation is rarely recommended. Exhaled air contains 16 to 18% oxygen and 4 to 5% carbon dioxide, which is adequate to maintain blood oxygen and carbon dioxide values close to normal. Larger-than-necessary volumes of air may cause gastric distention with associated risk of aspiration.
(See also Overview of Respiratory Arrest, Airway Establishment and Control, and Tracheal Intubation.)
Bag-Valve-Mask Devices
Bag-valve-mask devices consist of a self-inflating bag (resuscitator bag) with a nonrebreathing valve mechanism and a soft mask that conforms to the tissues of the face; when connected to an oxygen supply, they deliver from 60 to 100% inspired oxygen (see also How To Do Bag-Valve-Mask Ventilation). In the hands of experienced health care professionals, a bag-valve-mask device provides adequate temporary ventilation in many situations, allowing time to systematically achieve definitive airway control. However, if bag-valve-mask ventilation is used for > 5 minutes, air is typically introduced into the stomach, and a nasogastric tube should be inserted to evacuate the accumulated air.


Bag-valve-mask devices do not maintain airway patency, so patients with soft-tissue relaxation require careful positioning and manual maneuvers (see figures and ), as well as additional devices to keep the airway open.
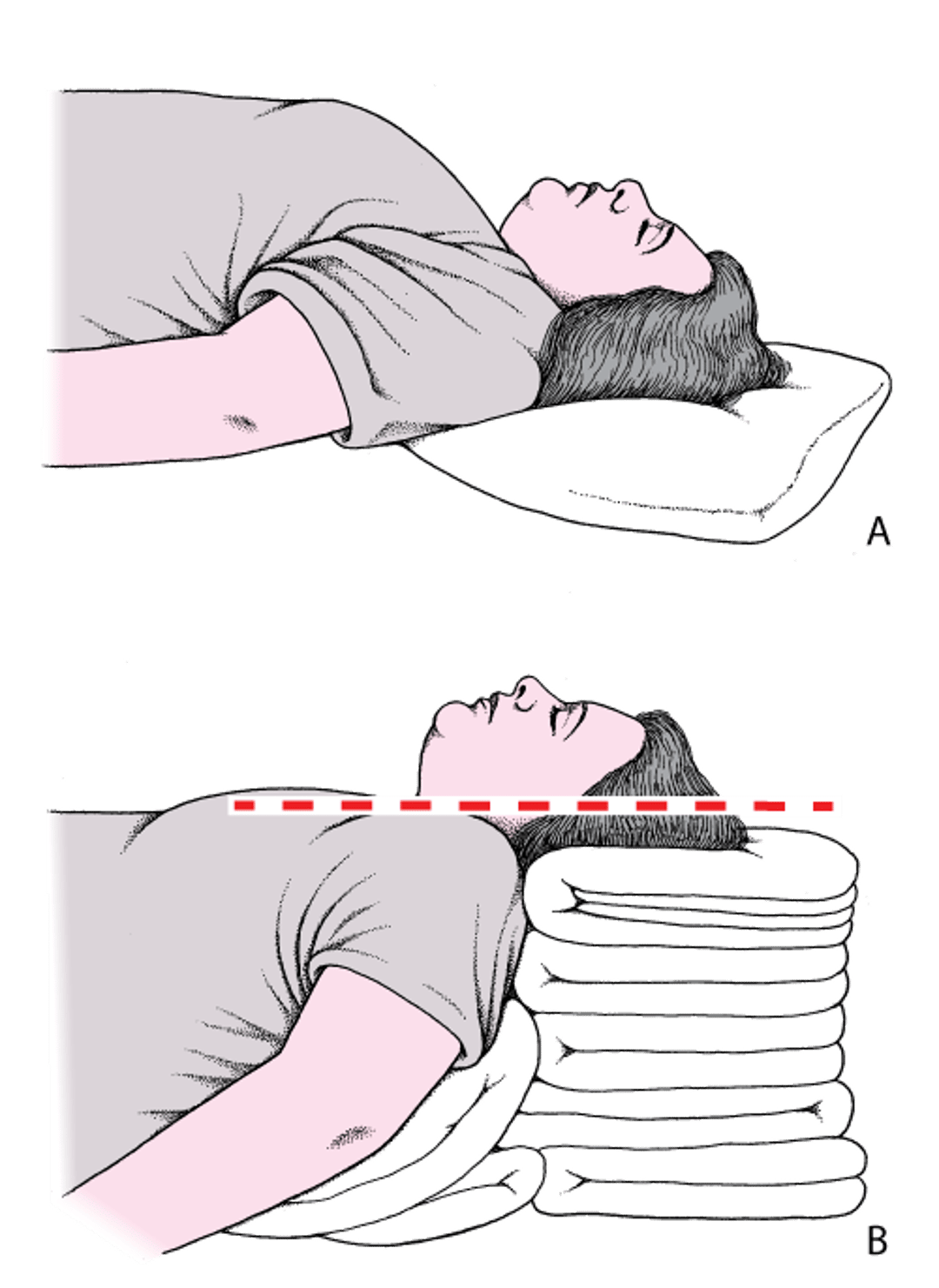
Head and Neck Positioning to Open the Airway
A: The head is flat on the stretcher; the airway is constricted. B: The ear and sternal notch are aligned, with the face parallel to the ceiling, opening the airway. Adapted from Levitan RM, Kinkle WC: The Airway Cam Pocket Guide to Intubation, ed. 2. Wayne (PA), Airway Cam Technologies, 2007. |

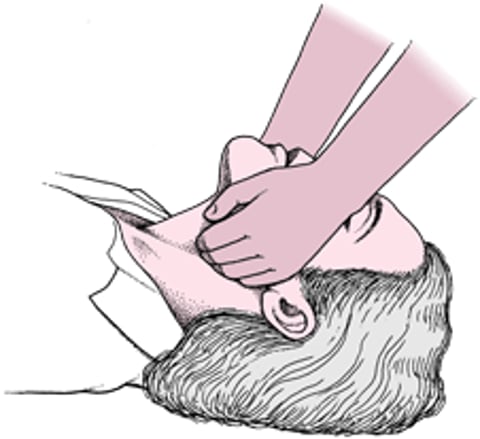
Jaw Thrust

An oropharyngeal airway or a nasopharyngeal airway may be used during bag-valve-mask ventilation to keep soft tissues of the oropharynx from blocking the airway. Oropharyngeal airways can cause gagging and the potential for vomiting and aspiration in conscious patients and so should be used with caution. Nasopharyngeal airways do not cause patients to gag and are recommended for use in patients who are awake or semiconscious and who may not tolerate an oropharyngeal airway due to the gag reflex.
Absolute contraindications for placement of a nasopharyngeal airway include significant mid-face injuries with suspected cribriform plate (basilar skull) fracture.
Relative contraindications include abnormalities in nasal anatomy (eg, significant nasal trauma, large polyps, recent nasal surgery) that could make passing a nasopharyngeal airway difficult.
The most common way to determine the proper size of oropharyngeal airway is to use an airway that is the same length as the distance between the corner of the patient’s mouth and the angle of the jaw.
Resuscitator bags are also used with artificial airways, including endotracheal tubes and supraglottic and pharyngeal airways. Pediatric bags have a pressure relief valve that limits peak airway pressures (usually to 35 to 45 cm water); clinicians must monitor the valve setting to avoid inadvertent hyperventilation. The relief valve can be shut off if necessary to provide sufficient pressure.

Laryngeal Mask Airways (LMA)
Supraglottic airways (SGAs) are inserted into the pharynx to allow ventilation, oxygenation, and administration of anesthetic gases without the need for endotracheal intubation. These devices are used for the following:
Primary airway management
Rescue ventilation when bag-valve-mask ventilation is difficult
Rescue ventilation when definitive airway management is expected to be difficult (eg, patient with anatomic abnormalities)
Ventilation when personnel are limited (eg, prehospital)
As a conduit for endotracheal intubation
The SGAs used most commonly in the operating room are the laryngeal mask airways (LMAs) and similar devices, while other SGAs are used more commonly in the emergency department and for prehospital airway management (see Other Devices).
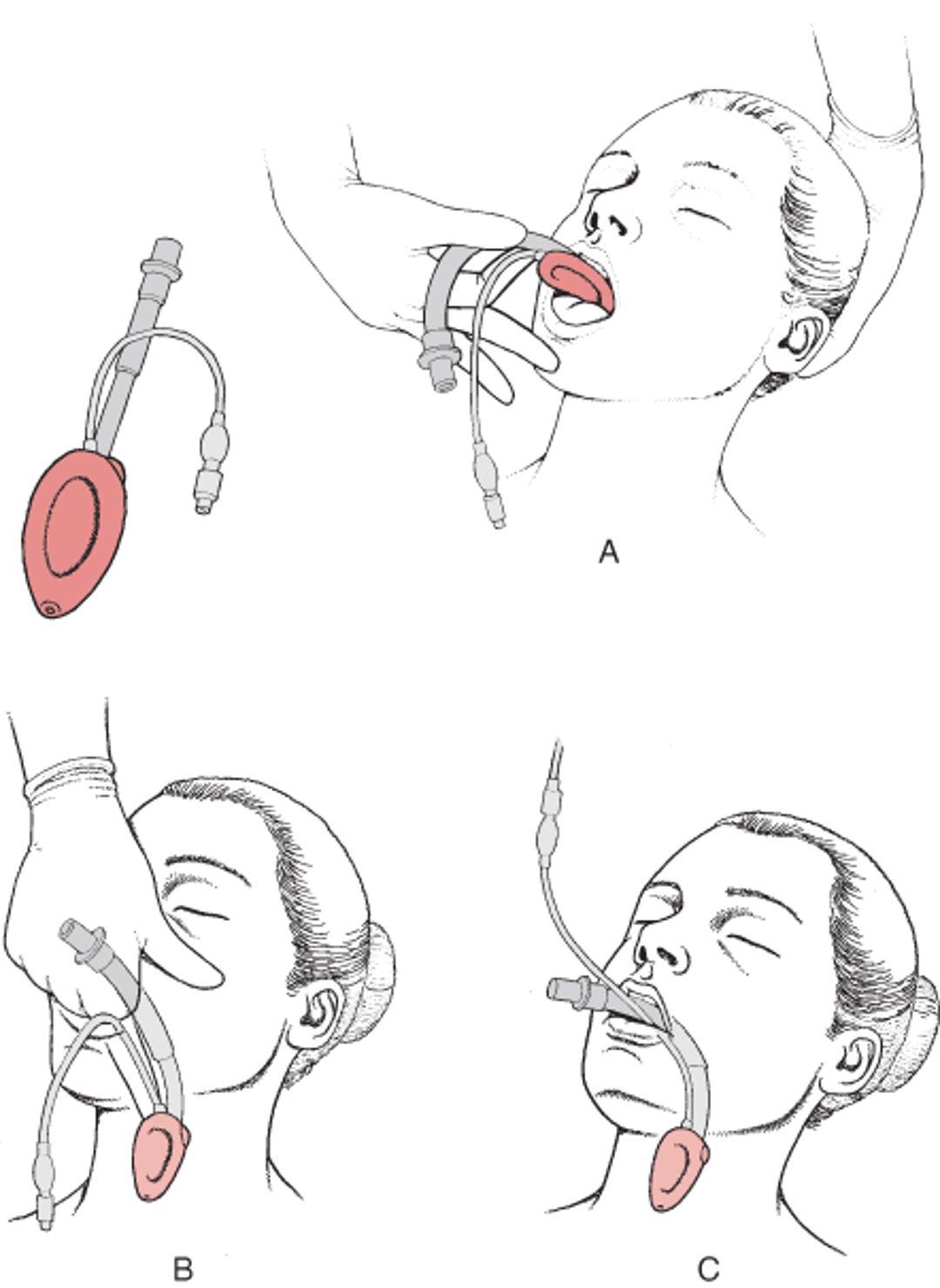
LMAs are inserted into the lower oropharynx to prevent airway obstruction by soft tissues and to create an effective channel for ventilation (see figure ). A variety of available LMAs allow passage of an endotracheal tube or a gastric decompression tube. As the name implies, these devices seal the laryngeal inlet (rather than the face-mask interface) and thus avoid the difficulty of maintaining an adequate face-mask seal and the risk of displacing the jaw and tongue. Complications include vomiting and aspiration in patients who have an intact gag reflex, who are receiving excessive ventilation, or both.
There are numerous techniques for LMA insertion (see How to Insert a Laryngeal Mask Airway). The standard approach is to press the deflated mask against the hard palate (using the long finger of the dominant hand) and rotate it past the base of the tongue until the mask reaches the hypopharynx so that the tip then sits in the upper esophagus. Once in the correct position, the mask is inflated. Inflating the mask with half the recommended volume before insertion stiffens the tip, possibly making insertion easier. Some mask versions replace the inflatable cuff with a gel that molds to the airway.
Although a LMA does not isolate the airway from the esophagus as well as an endotracheal tube, it has some advantages over bag-valve-mask ventilation:
It minimizes gastric inflation
It provides some protection against passive regurgitation
Most versions of LMAs have an opening through which a small tube can be inserted to decompress the stomach.
The efficacy of the airway seal with an LMA, unlike endotracheal tubes, is not directly correlated with the mask inflation pressure. With endotracheal tubes, higher balloon pressure causes a tighter seal; with an LMA, overinflation makes the mask more rigid and less able to adapt to the patient’s anatomy. If the seal is inadequate, mask pressure should be lowered somewhat; if this approach does not work, a larger mask size should be tried.
In emergencies, laryngeal mask airways should be viewed as bridging devices. Prolonged placement, overinflation of the mask, or both may compress the tongue and cause tongue edema. Also, if patients who are conscious are given muscle relaxants before LMA insertion (eg, for laryngoscopy), they may gag and possibly aspirate when such medications wear off. Either the device should be removed (assuming ventilation and gag reflexes are adequate), or medications should be given to eliminate the gag response and provide time for an alternative intubation technique.
A contraindication to use of an LMA is massive facial trauma.
Laryngeal Mask Airway (LMA)
The LMA is a tube with an inflatable cuff that is inserted into the oropharynx. A: The deflated cuff is inserted into the mouth. B: With the index finger, the cuff is guided into place above the larynx. C: Once in place, the cuff is inflated. Some cuffs use a gel that molds to the airway rather than an inflatable cuff. |

Endotracheal Tubes
An endotracheal tube is inserted directly into the trachea via the mouth. Endotracheal tubes have high-volume, low-pressure balloon cuffs to prevent air leakage and minimize the risk of aspiration. Cuffed tubes were traditionally used only in adults and children > 8 years; however, cuffed tubes sometimes are used in infants and younger children to limit air leakage or aspiration (particularly during transport). Sometimes cuffs are not inflated or inflated only to the extent needed to prevent obvious leakage.
An endotracheal tube is the definitive method to secure a compromised airway, limit aspiration, and initiate mechanical ventilation in patients who are comatose, cannot protect their own airways, or need prolonged mechanical ventilation. An endotracheal tube also permits suctioning of the lower respiratory tract. Although medications can be delivered via an endotracheal tube during cardiac arrest, this practice is discouraged.
Placement typically requires laryngoscopy by a skilled clinician, but a variety of novel insertion devices that provide other options are available (see Tracheal Intubation).
Other Devices
Other supraglottic airway devices include laryngeal tube or twin-lumen airways (eg, Combitube, King laryngeal tube— see How To Insert an Esophageal-Tracheal Double Lumen Tube (Combitube) or a King Laryngeal Tube). These devices use 2 balloons to create a seal above and below the larynx and have ventilation ports overlying the laryngeal inlet (which is between the balloons). As with laryngeal mask airways, prolonged placement and balloon overinflation can cause tongue edema. These devices can be used as alternative airway after failed intubation attempts with an endotracheal tube.