

Corneal abrasions are self-limited, superficial epithelial defects. Superficial foreign bodies frequently cause corneal abrasions and should be removed.
(See also Overview of Eye Trauma.)
The most common corneal injuries are retained foreign bodies and abrasions. As many as 25% of patients presenting to an emergency department with ocular complaints have a corneal abrasion (1, 2).
Although superficial foreign bodies often spontaneously exit the cornea in the tear film, occasionally leaving a residual abrasion, other foreign bodies remain on or within the cornea. A foreign body trapped under the upper eyelid may cause 1 or more vertical corneal abrasion that worsen as a result of blinking. Intraocular penetration can occur with seemingly minor trauma and may resemble corneal abrasions in its presentation (3), particularly when foreign bodies result from the debris thrown off by high-speed machines (eg, drills, saws, grinders, rotary tools, anything with a metal-on-metal mechanism), hammering, or explosions.
Infection does not usually develop in a corneal injury from a metallic foreign body. However, corneal scarring and rust deposits can develop.
If a corneal foreign body is contaminated organic material or if the corneal abrasion is secondary to a contact lens, infection can develop. A common cause of corneal damage is improper use of contact lenses. Also, if intraocular penetration is not recognized, regardless of foreign body composition, infection within the eye (endophthalmitis) or inflammation (iridocyclitis) may develop and may put vision at risk.
References
1. Edwards RS: Ophthalmic emergencies in a district general hospital casualty department. Br J Ophthalmol 71(12):938-942, 1987. doi: 10.1136/bjo.71.12.938
2. Channa R, Zafar SN, Canner JK, et al: Epidemiology of eye-related emergency department visits. JAMA Ophthalmol 134(3):312-319, 2016. doi: 10.1001/jamaophthalmol.2015.5778
3. Chronopoulos A, Ong JM, Thumann G, et al: Occult globe rupture: diagnostic and treatment challenge. Surv Ophthalmol 63(5):694-699, 2018. doi: 10.1016/j.survophthal.2018.04.0015
Symptoms and Signs of Corneal Abrasions and Corneal Foreign Bodies
Symptoms and signs of corneal abrasion or foreign body include foreign body sensation in the eye, tearing, redness, and occasionally discharge. Vision may be affected if the abrasion involves the visual axis (central cornea).

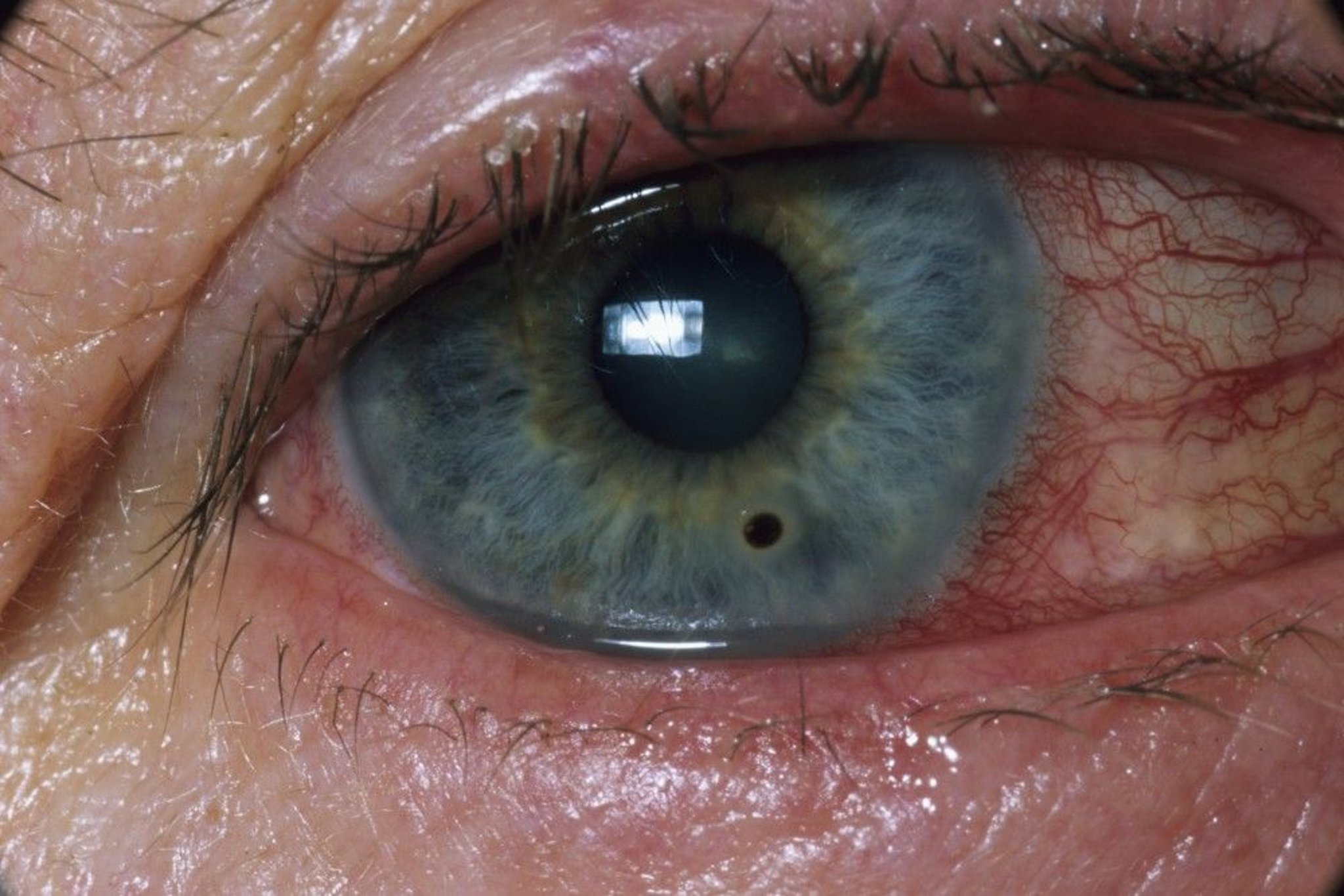
A small foreign body (black, inferior to the pupil) in the cornea of a stone grinder.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Diagnosis of Corneal Abrasions and Corneal Foreign Bodies
Slit-lamp examination, usually with fluorescein stainingSlit-lamp examination, usually with fluorescein staining
Upper eyelid eversion to examine for a foreign body
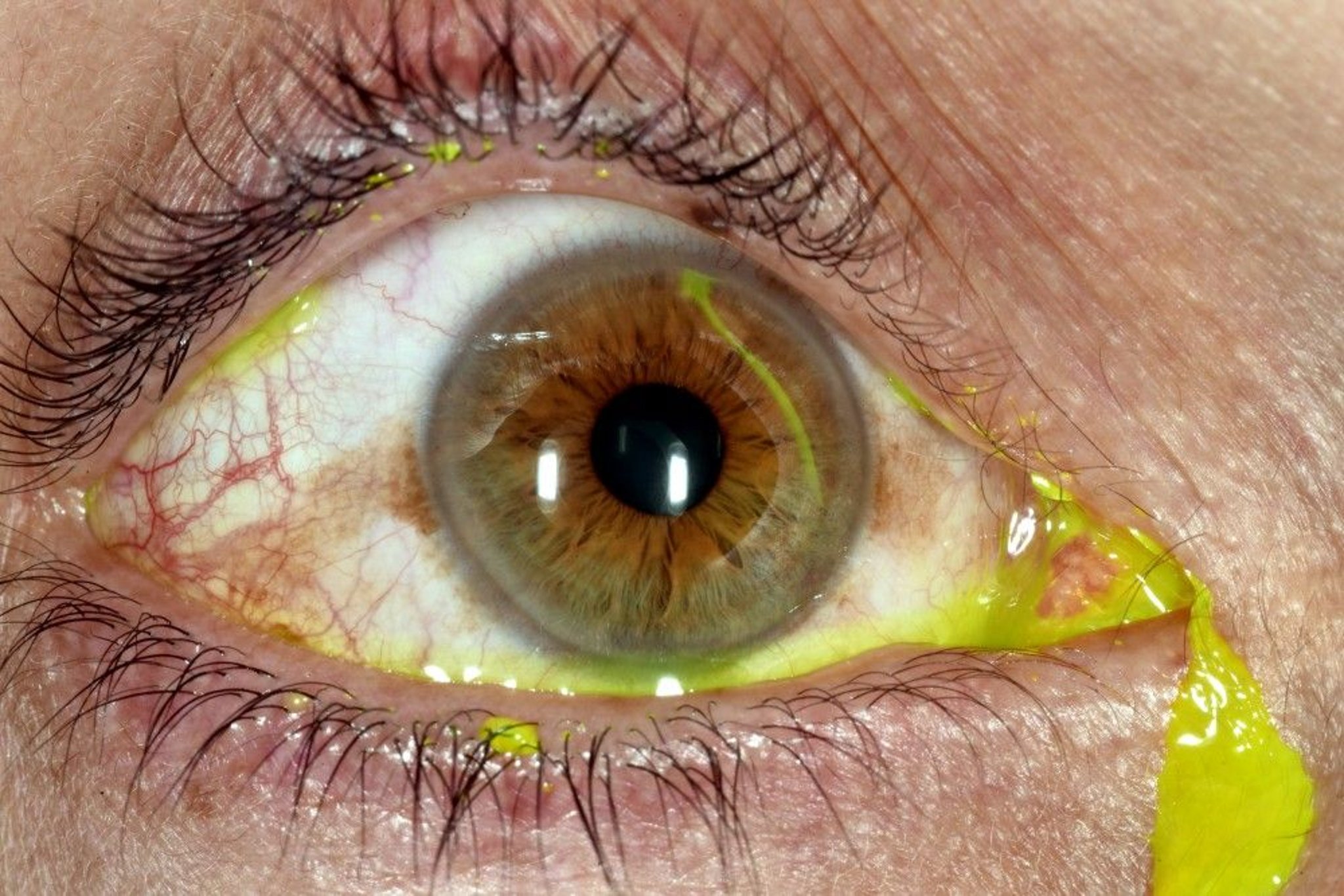
A curvilinear corneal abrasion medial to the pupil seen with fluorescein staining.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
After a topical anesthetic (eg, 1 to 2 drops of proparacaine 0.5%) is instilled into the inferior fornix, the upper and lower eyelids are everted, and the entire conjunctiva and cornea are inspected with a binocular lens (loupe) or a slit lamp. Fluorescein is applied to the inferior fornix and will distribute into the tear film (see After a topical anesthetic (eg, 1 to 2 drops of proparacaine 0.5%) is instilled into the inferior fornix, the upper and lower eyelids are everted, and the entire conjunctiva and cornea are inspected with a binocular lens (loupe) or a slit lamp. Fluorescein is applied to the inferior fornix and will distribute into the tear film (seecorneal examination). Cobalt blue light illumination of the fluorescein during ). Cobalt blue light illumination of the fluorescein duringslit-lamp examination renders abrasions and nonmetallic foreign bodies more apparent. A positive Seidel sign, streaming of fluorescein away from a corneal laceration, indicates leakage of aqueous fluid from the anterior chamber through a corneal perforation. renders abrasions and nonmetallic foreign bodies more apparent. A positive Seidel sign, streaming of fluorescein away from a corneal laceration, indicates leakage of aqueous fluid from the anterior chamber through a corneal perforation.
Patients with multiple vertical linear abrasions should have their eyelids everted to search for a foreign body under the upper lid.
Patients with a high-risk intraocular injury or (more rarely) visible globe perforation or a misshapen pupil should undergo CT to rule out an intraocular foreign body; these patients should be seen by an ophthalmologist emergently. The globe should be protected with an eye shield until perforation has been ruled out. If a shield is unavailable, a paper or Styrofoam cup can be cut so that the diameter of the cup approximates the diameter of the orbital rim, over which it is placed as a temporary shield. No pressure is placed on the globe because doing so may cause extrusion of intraocular contents through the rupture site. Extra caution should be taken to ensure that any bandages, eye patches, or eye shields are secured to the orbital rim without contacting the eyelid or globe. CT is the imaging modality of choice in cases of ocular and periocular trauma (1, 2).
Diagnosis references
1. Balakrishnan S, Harsini S, Reddy S, et al. Imaging review of ocular and optic nerve trauma. Emerg Radiol 27(1):75-85, 2020. doi: 10.1007/s10140-019-01730-y
2. Thelen J, Bhatt AA, Bhatt AA: Acute ocular traumatic imaging: what the radiologist should know [corrected]. Emerg Radiol 24(5):585-592, 2017. doi: 10.1007/s10140-017-1528-0. Epub 2017 Jun 17. Erratum in: Emerg Radiol 24(5):593, 2017. doi: 10.1007/s10140-017-1536-0
Treatment of Corneal Abrasions and Corneal Foreign Bodies
For corneal surface or conjunctival foreign bodies, irrigation or removal with a damp, cotton-tipped swab or a small needle
For corneal abrasions, antibiotic ointment and sometimes pupillary dilation
For intraocular foreign bodies, surgical removal
After a topical anesthetic is instilled into the conjunctiva, clinicians can remove conjunctival foreign bodies by irrigation or lift them out with a moist sterile cotton applicator. A corneal foreign body that cannot be dislodged by irrigation may be lifted out carefully on the point of a sterile spud (an instrument designed to remove ocular foreign bodies) or of a 25- or 27-gauge hypodermic needle while visualizing using loupes (magnifying eyeglasses) or, preferably, slit-lamp magnification; the patient must be able to stare without moving the eye during removal. Of note, the tip of the hypodermic needle is always applied to the cornea from the side; it should never approach the cornea head on, as this may result in inadvertent corneal penetration.
Steel or iron foreign bodies remaining on the cornea for more than a few hours may leave a rust ring on the cornea that also requires removal under slit-lamp magnification by scraping or using a low-speed rotary burr; removal should be done by an ophthalmologist. After this procedure, residual corneal abrasions are treated.
Corneal abrasions
Eye pressure patches do not reduce pain or improve healing time, and they may increase risk of infection. Pressure patches are usually not used, particularly for an abrasion caused by a contact lens or an object that may be contaminated with soil or vegetation (1, 2).
Although there are no studies showing that ophthalmic antibiotic ointments (eg, bacitracin/polymyxin B or erythromycin) are associated with decreased infection rates, they are used for most abrasions until the epithelial defect is healed. Contact lens wearers with corneal abrasions require an antibiotic with optimal antipseudomonal coverage (eg, ciprofloxacin 0.3% ointment).Although there are no studies showing that ophthalmic antibiotic ointments (eg, bacitracin/polymyxin B or erythromycin) are associated with decreased infection rates, they are used for most abrasions until the epithelial defect is healed. Contact lens wearers with corneal abrasions require an antibiotic with optimal antipseudomonal coverage (eg, ciprofloxacin 0.3% ointment).
Ophthalmic corticosteroids are contraindicated because they tend to promote the growth of fungi and reactivation of herpes simplex virus. Continued use of topical anesthetics are also contraindicated because they can potentially impair healing and may mask the pain associated with a nonhealing or worsening abrasion. Studies have not demonstrated a difference in pain relief for patients who were given short-term topical anesthetics versus placebo (3). Pain can be managed with oral analgesics. For symptomatic relief of larger abrasions (eg, area > 10 mm2), the pupil is also dilated once with a short-acting cycloplegic (eg, 1 drop cyclopentolate 1% or homatropine 5%). Topical nonsteroidal anti-inflammatory drugs (NSAIDs) (eg, diclofenac) are not approved for treatment of corneal abrasions and do not appear to be more effective than oral analgesics (), the pupil is also dilated once with a short-acting cycloplegic (eg, 1 drop cyclopentolate 1% or homatropine 5%). Topical nonsteroidal anti-inflammatory drugs (NSAIDs) (eg, diclofenac) are not approved for treatment of corneal abrasions and do not appear to be more effective than oral analgesics (4).
The corneal epithelium regenerates rapidly; even large abrasions generally heal within 1 to 3 days. A contact lens should not be worn until the injury is healed. Follow-up examination by an ophthalmologist 1 or 2 days after injury is recommended, especially if a foreign body was removed or the abrasion was caused by organic material.
Treatment references
1. Lim CH, Turner A, Lim BX: Patching for corneal abrasion. Cochrane Database Syst Rev 7(7):CD004764, 2016. doi: 10.1002/14651858.CD004764.pub3
2. Kaiser PK: A comparison of pressure patching versus no patching for corneal abrasions due to trauma or foreign body removal. Corneal Abrasion Patching Study Group. Ophthalmology 102(12):1936-1942, 1995. doi: 10.1016/s0161-6420(95)30772-5
3. Puls HA, Cabrera D, Murad MH, et al: Safety and effectiveness of topical anesthetics in corneal abrasions: Systematic review and meta-analysis. J Emerg Med 49(5):816-824, 2015. doi: 10.1016/j.jemermed.2015.02.051
4. Wakai A, Lawrenson JG, Lawrenson AL, et al: Topical non-steroidal anti-inflammatory drugs for analgesia in traumatic corneal abrasions. Cochrane Database Syst Rev 5(5):CD009781, 2017. doi: 10.1002/14651858.CD009781.pub2
Key Points
Symptoms of corneal abrasion or foreign body include foreign body sensation, tearing, and redness; visual acuity is typically unchanged.
Diagnosis is usually by slit-lamp examination with fluorescein staining.Diagnosis is usually by slit-lamp examination with fluorescein staining.
Suspect an intraocular foreign body if fluorescein streams away from a corneal defect, if the pupil is irregular, or if the mechanism of injury involves a high-speed machine (eg, drill, saw, anything with a metal-on-metal mechanism), hammering, or explosion. Suspect an intraocular foreign body if fluorescein streams away from a corneal defect, if the pupil is irregular, or if the mechanism of injury involves a high-speed machine (eg, drill, saw, anything with a metal-on-metal mechanism), hammering, or explosion.
Never patch an eye with a suspected penetrating injury. Always use only an eye shield.
For intraocular foreign bodies, give systemic and topical antibiotics, apply a shield, control pain and nausea, and consult an ophthalmologist for surgical removal.





