





In gastroesophageal reflux disease, stomach contents, including acid and bile, flow backward from the stomach into the esophagus, causing inflammation in the esophagus and pain in the bottom of the chest.
Reflux occurs when the ring-shaped muscle that normally prevents the contents of the stomach from flowing back into the esophagus (called the lower esophageal sphincter) does not function properly.
The most typical symptom is heartburn (a burning pain behind the breastbone).
The diagnosis is based on symptoms and sometimes esophageal pH testing.
The first treatments include weight loss, smoking cessation, avoiding bedtime meals, elevating the head of the bed, and taking medications that reduce stomach acid. If these methods fail, doctors sometimes do surgery.
The esophagus is the hollow tube that leads from the throat (pharynx) to the stomach. The lower esophageal sphincter is the ring of muscle that holds the bottom of the esophagus closed so that food and stomach acid do not flow back up the esophagus. When people swallow, this sphincter normally relaxes to allow food into the stomach. (See also Overview of the Esophagus.)
Gastroesophageal reflux disease (GERD) is common. It occurs in about 13% of people worldwide. Reflux of stomach contents into the esophagus occurs frequently in infants and can be normal and is not always considered GERD.
The stomach lining protects the stomach from the effects of its own acid. Because the esophagus lacks a similar protective lining, stomach acid and bile that flow backward (reflux) into the esophagus may cause symptoms and in some cases damage.
Acid and bile reflux into the esophagus when the lower esophageal sphincter is not functioning properly. When a person is standing or sitting, gravity helps prevent the reflux of stomach contents into the esophagus, which explains why reflux can worsen when a person is lying down. Reflux is also more likely to occur soon after meals, when the volume and acidity of contents in the stomach are higher and the sphincter is less likely to work properly. Factors contributing to reflux include:
Obesity
Tobacco smoking
Fatty foods
Caffeinated and carbonated beverages
Alcohol
Certain medications
Types of medications that interfere with lower esophageal sphincter function include those that have anticholinergic effects (such as many antihistamines and some antidepressants), calcium channel blockers, progesterone, and nitrates. Delayed emptying of the stomach (for example, due to diabetes or use of opioids) can also worsen reflux. Some people also seem to have a genetic predisposition to GERD.
Symptoms of GERD
Heartburn (a burning pain behind the breastbone) is the most obvious symptom of gastroesophageal reflux. Heartburn may be accompanied by regurgitation, in which the stomach contents reach the mouth. If stomach contents reach the mouth, they sometimes cause sore throat, hoarseness, cough, or a sensation of a lump in the throat. Rarely, stomach contents trickle into the lungs, causing cough and/or wheezing. People who have longstanding heartburn sometimes develop difficulty swallowing (dysphagia).
Complications of gastroesophageal reflux
Prolonged exposure of the lower part of the esophagus to repeated reflux may cause:
Inflammation of the esophagus (esophagitis)
Ulcers of the esophagus (erosive esophagitis)
Narrowing of the esophagus (esophageal stricture)
Changes to the cells lining the esophagus (Barrett esophagus)
Abnormal cells in the esophagus that may become cancerous (see Esophageal Cancer)
Inflammation of the esophagus (esophagitis or erosive esophagitis) causes symptoms typical of gastroesophageal reflux disease but perhaps more severe. It also may cause pain with swallowing (odynophagia).
Some people have bleeding that is usually slight but can be massive. The blood may be vomited up or may pass through the digestive tract, resulting in the passage of dark, tarry stools (melena) or bright red blood, if the bleeding is heavy enough. Mild bleeding over a long period of time can cause iron deficiency anemia.

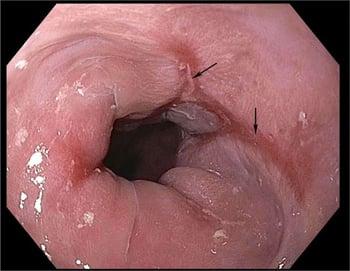
Repeated reflux may cause ulcers (arrows) to form on the inner surface of the esophagus.
Photo provided by Kristle Lynch, MD.
Esophageal ulcers are open sores on the inner lining of the esophagus, a type of disruption of that surface. They can cause chest pain upon swallowing that is usually located behind the breastbone or just below it, similar to the location of heartburn.
Narrowing (stricture) of the esophagus caused by reflux makes swallowing solid foods increasingly more difficult.

Reflux may cause the esophagus to become narrow. This photo shows ulcers of the inner surface of the esophagus (arrows) above a narrowing (stricture) of the esophagus.
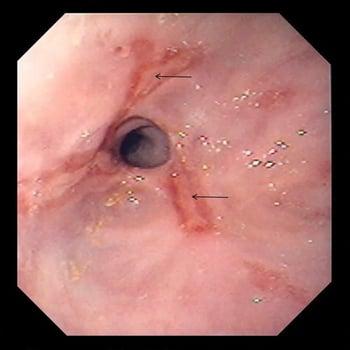
Prolonged irritation causes the cells lining the esophagus to change, which results in a condition called Barrett esophagus. Changes may occur without symptoms. These abnormal cells are precancerous and can sometimes progress to cancer.


Repeated backflow of stomach acid (reflux) may cause the cells in the esophagus to change and become precancerous. In this photo, the red areas are examples of these changes.
Diagnosis of GERD
Usually, no specific testing
Sometimes endoscopy with biopsy
Sometimes pH testing
Sometimes manometry
When symptoms point to the diagnosis of GERD, treatment can be started without testing. Testing is usually done when the diagnosis is not clear, treatment has not controlled symptoms, or symptoms have been present for a long time.
When testing is needed, the first test is usually to examine the esophagus using a flexible viewing tube (endoscopy). Endoscopy is the best test for diagnosing esophagitis, erosive esophagitis, esophageal ulcer, esophageal strictures, esophageal cancer, and Barrett esophagus. During endoscopy, doctors may remove tissue for examination under a microscope (biopsy).
If endoscopy and biopsy results are normal in people whose symptoms are very suggestive of GERD, doctors may do esophageal pH testing (pH is a measure of acidity—see catheter-based monitoring). In this test, a thin, flexible tube with a sensor probe on the tip is placed through the nose and into the lower esophagus. The tube stays in place for 24 hours. The other end of this tube is attached to a monitor that is worn by the person. The monitor records the acid levels in the esophagus, usually for 24 hours. Besides determining how much reflux is occurring, this test identifies the relationship between symptoms and reflux. This test is also helpful for people who have symptoms that are not typical of reflux. The esophageal pH test is suggested for all people being considered for surgery to correct gastroesophageal reflux. People who cannot tolerate a tube in their nose can have a small pH capsule attached to the lower part of their esophagus (see wireless monitoring).
Pressure measurements at the lower esophageal sphincter using a test called manometry indicate how well the sphincter is functioning and also provide information on the strength with which the esophageal muscles push. The information gained from this test helps the doctor decide whether surgery is an appropriate treatment.
Treatment of GERD
Weight loss, for people with overweight or obesity
Avoiding eating before bedtime
Quitting smoking
Elevating the head of the bed
Proton pump inhibitors (PPIs) or other medications
Sometimes antireflux surgery (fundoplication)
Nonmedication treatment
Several measures besides taking medication often help with gastroesophageal reflux.
Weight loss often helps prevent or reduce reflux symptoms in people with overweight.
People should avoid eating 4 hours before bedtime.
Quitting smoking often reduces reflux symptoms.
Raising the head of the bed about 6 inches (about 15 centimeters) by placing 6- to 8-inch (about 15- to 20-centimeter) blocks under the legs at the head of the bed, by using a wedge pillow, or by placing a wedge under the mattress can help prevent acid from flowing into the esophagus as a person sleeps.
In addition, medications that cause symptoms should be avoided, as should smoking. Caffeine, alcohol, fatty foods, chocolate, acid-containing beverages such as orange juice, cola drinks, vinegar-based salad dressings, and other substances that strongly stimulate the stomach to produce acid or that delay stomach emptying should be avoided as well.
Medication
Proton pump inhibitors, the most powerful medications for reducing stomach acid production, are usually the most effective treatment for gastroesophageal reflux and for esophagitis and erosive esophagitis due to gastroesophageal reflux. Once the inflammation in the esophagus has healed, these medications may be continued long-term, but if this is necessary, doctors try to use a lower dose.
Histamine-2 (H2) blockers are other acid-reducing medications that are effective in people who have mild symptoms of GERD, especially at night.
Potassium-competitive acid blockers are a newer type of medication that block acid secretion and can be effective in more severe disease.
Medications that stimulate the movement of contents through the esophagus, stomach, and intestines (called promotility medications, such as metoclopramide) are not as effective as proton pump inhibitors but may be added to a proton pump inhibitor regimen.
Surgical and endoscopic treatment
Esophageal narrowing is treated by repeatedly dilating the narrowed area using balloons or tubes. If dilation is successful, narrowing does not seriously limit what a person can eat.
Surgery is an option for treatment of gastroesophageal reflux for people who cannot tolerate medications, who have large amounts of reflux that is not acidic but that does cause symptoms, or who have ulcers, bleeding, large hernias, or severe esophagitis. In addition, surgery may be the preferred treatment for people who do not like the prospect of having to take medications for many years. A minimally invasive procedure done through a laparoscope (called fundoplication) is available. However, some people who undergo this procedure have side effects, most commonly difficulty swallowing and a feeling of bloating or abdominal discomfort after eating.
Treatment of Barrett esophagus
Barrett esophagus rarely disappears after use of a proton pump inhibitor and typically remains unchanged. If the cells become precancerous, treatment options that can be done during endoscopy include methods that destroy the abnormal tissue using radio waves (radiofrequency ablation), extreme cold (cryotherapy), or a laser beam (laser ablation). Alternatively, the tissue may also be surgically removed. However, abnormal cells may still remain even after treatment relieves symptoms. Therefore, people with Barrett esophagus are asked to undergo an endoscopic examination periodically to ensure that the condition is not progressing to cancer.
Drug Information for the Topic





