

Motor neuron diseases are characterized by progressive deterioration of the nerve cells that initiate muscle movement. As a result, the muscles stimulated by these nerves deteriorate, become weak, and no longer function normally.
Amyotrophic lateral sclerosis (Lou Gehrig disease) is the most common form of motor neuron disease.
Typically, muscles are weak and waste away, and movements become stiff, clumsy, and progressively more difficult to execute.
Doctors base the diagnosis mostly on results of the evaluation and do electromyography, nerve conduction studies, magnetic resonance imaging, and blood tests to help confirm the diagnosis.
There is no cure, but medications can help lessen symptoms.
(See also Overview of the Peripheral Nervous System.)
Motor neuron diseases may involve the central nervous system (brain and spinal cord) as well as the peripheral nervous system (nerves outside the brain and spinal cord).
For normal muscle function, muscle tissue and nerve connections between the brain and muscle must be normal. Muscle movement is initiated by nerve cells (neurons) that are located in the spinal cord and in the front part of the brain (called the motor cortex). Nerve cells in the motor cortex connect with the nerve cells in the spinal cord that stimulate muscles to move (called motor nerves). In motor neuron diseases, these nerve cells progressively wither away and the peripheral nerves that connect them to the muscle deteriorate. As a result, muscles weaken, waste away (atrophy), and can become completely paralyzed even though the muscles themselves are not the cause of the problem.
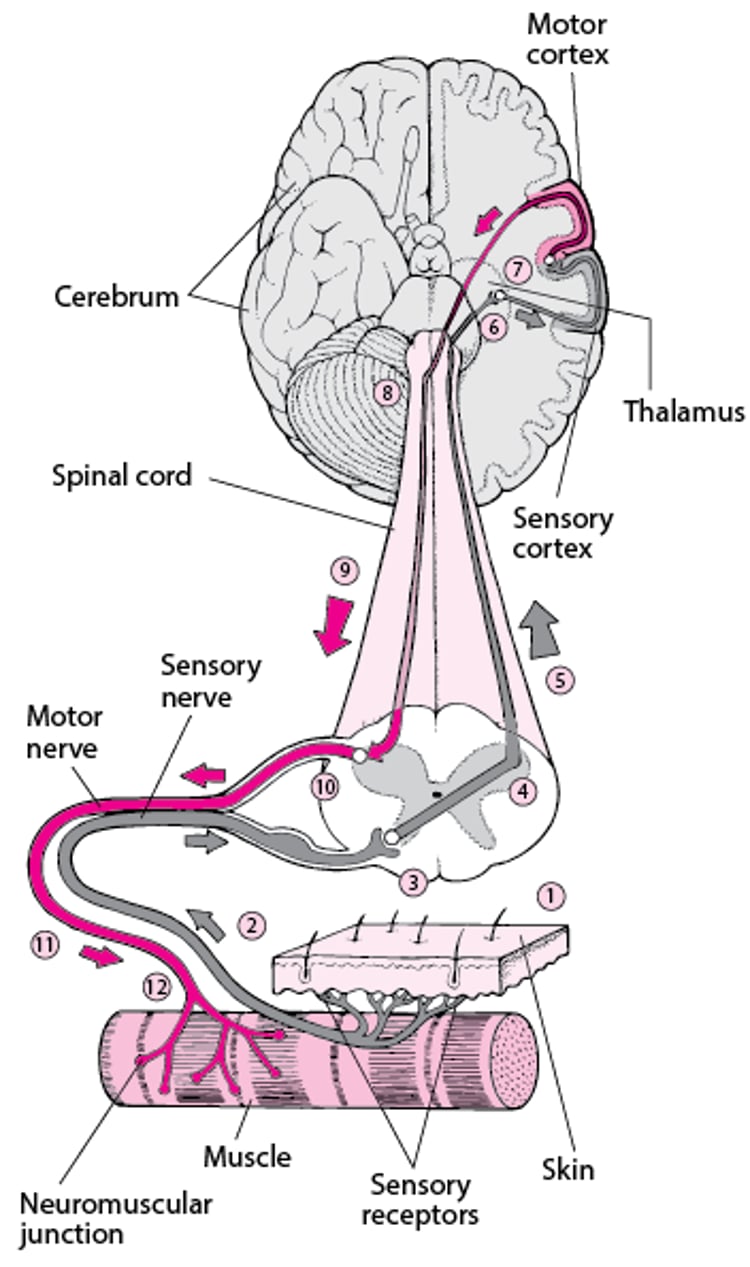
Using the Brain to Move a Muscle
Moving a muscle usually involves communication between the muscle and the brain through nerves. The impetus to move a muscle may originate in the brain, as when a person consciously decides to move a muscle—for example, to pick up a book. Or the impetus to move a muscle may originate with the senses. For example, special nerve endings in the skin (sensory receptors) enable people to sense pain or a change in temperature. This sensory information is sent to the brain, and the brain may send a message to the muscle about how to respond. This type of exchange involves two complex nerve pathways:
| |
| |
If the sensation occurs suddenly and is severe (as when stepping on a sharp rock or picking up a cup of very hot coffee), the impulse may travel to the spinal cord and directly back to the motor nerve, bypassing the brain. The result is a quick response of a muscle—by immediately withdrawing from whatever is causing the pain. This response is called a spinal reflex. | |

Motor neuron diseases have various forms, such as the following:
Amyotrophic lateral sclerosis (the most common)
Motor neuron diseases are more common among men and usually develop in people who are in their 50s to 70s. The cause is usually unknown. Some people who have a motor neuron disease have a hereditary type (caused by a mutation in a gene) and thus have family members who also have the disease.
Different parts of the nervous system may be affected first. For example, some forms of motor neuron disease affect the mouth and throat first. Others affect a hand or foot first or affect them most severely.
Long-lasting paralysis can lead to permanent shortening of muscles (contractures).
Symptoms of ALS and Other Motor Neuron Diseases
Muscle strength is affected, but people do not have pain or any changes in sensation. Depression is common.
Amyotrophic lateral sclerosis (Lou Gehrig disease)
This progressive motor neuron disease begins with weakness, often in the hands and less frequently in the feet or mouth and throat. Weakness may progress more on one side of the body than on the other and usually proceeds up the arm or leg. Muscles, usually those in the hands and feet, start to waste away (atrophy). Muscle cramps are also common and may occur before the weakness, but no changes in sensation occur. People lose weight and feel unusually tired.
Over time, weakness increases.
When amyotrophic lateral sclerosis affects motor nerves in the brain, muscle tone typically increases, and muscles tend to become stiff and tight, leading to muscle spasms (called spasticity). Movements are stiff and clumsy. When motor nerves in the spinal cord are affected, muscle tone decreases, making the limbs seem loose and floppy. When the connection between motor nerves and muscles is lost, the muscles twitch spontaneously (called fasciculations).
Controlling facial expressions may become difficult. Weakening of muscles in the throat may lead to slurred speech and difficulty swallowing (dysphagia). Because swallowing is difficult, people sometimes drool and are more likely to choke on liquids. Food or saliva can be inhaled (aspirated) into the lungs, increasing the risk of pneumonia (called aspiration pneumonia). The voice usually sounds nasal but may be hoarse.
As symptoms progress, people may be unable to control emotional responses and may laugh or cry inappropriately.
Eventually, the muscles involved in breathing weaken, leading to breathing problems. Some people need a ventilator to breathe.
How rapidly amyotrophic lateral sclerosis progresses varies:
About 50% of people with the disorder die within 3 years of the first symptoms.
About 20% live 5 years.
About 10% live 10 years or more.
A few people survive more than 30 years.
Primary lateral sclerosis and progressive pseudobulbar palsy
These motor neuron diseases are rare, slowly progressive variants of amyotrophic lateral sclerosis:
Primary lateral sclerosis affects mainly the arms and legs.
Progressive pseudobulbar palsy affects mainly the muscles of the face, jaw, and throat.
In both disorders, muscles are weak and very stiff and tight (spastic), but muscle twitching (called fasciculations) and wasting do not occur.
Emotions may be changeable: People with progressive pseudobulbar palsy may switch from happiness to sadness quickly and without reason. Inappropriate emotional outbursts (for example, sudden laughter or crying) are common.
Symptoms usually progress for several years before total disability results.
Progressive muscular atrophy
Progressive muscular atrophy can develop at any age. It is similar to amyotrophic lateral sclerosis, except motor nerves in the brain are not affected. Also, this disease progresses more slowly. Spasticity does not occur, but muscles weaken, become limp (flaccid), and waste away. Involuntary contractions or twitching of muscle fibers (fasciculations) may be the earliest symptoms.
The hands are usually affected first, followed by the arms, shoulders, and legs. Eventually, the whole body is affected.
Many people with progressive muscular atrophy survive 25 years or longer.
Progressive bulbar palsy
In progressive bulbar palsy, the nerves controlling the muscles of chewing, swallowing, and talking are affected, making these functions increasingly difficult. The voice may have a nasal tone. In some people, emotions are changeable.
Because swallowing is difficult, food or saliva is often inhaled into the lungs, causing choking or gagging and increasing the risk of aspiration pneumonia.
Death, which is often due to pneumonia, usually occurs 1 to 3 years after symptoms appear.
Diagnosis of ALS and Other Motor Neuron Diseases
A doctor's evaluation
Tests such as magnetic resonance imaging, electromyography, and nerve conduction studies
Blood and sometimes urine tests and a spinal tap
Doctors suspect motor neuron disease in adults who have progressive muscle weakness without pain or loss of sensation. Doctors ask people the following:
Which parts of the body are affected
When symptoms started
Which symptoms appeared first
How the symptoms have changed over time
This information gives them clues about the cause of symptoms.
Muscle weakness can have many causes. Diagnostic tests, such as the following, are done to help narrow the possibilities:
Electromyography, which involves recording electrical activity in the muscles, can help determine whether the problem is in nerves, neuromuscular junction, or muscles.
Nerve conduction studies, which measure how fast nerves transmit impulses, may also be done. The speed of impulses is not affected until late in motor neuron disease, so if impulses are unexpectedly slow early in the disease, the cause of symptoms may be another disorder.
Magnetic resonance imaging (MRI) of the brain and sometimes the spinal cord is done to check for abnormalities that may cause similar symptoms.
Tests are done to check for other disorders that can cause weakness.
To test for other disorders, doctors may do the following:
Blood tests to check for infections (such as syphilis) and metabolic disorders
Urine tests to check for heavy metals (such as lead or mercury) if people have been exposed to them
A spinal tap (lumbar puncture) to check for signs of inflammation in the fluid that surrounds the brain and spinal cord (cerebrospinal fluid)
Genetic tests to check for hereditary disorders such as hereditary neuropathies
Over time, motor neuron diseases tend to cause symptoms that are so characteristic that the diagnosis is obvious without any testing.
Treatment of ALS and Other Motor Neuron Diseases
Physical therapy
Medications to relieve symptoms
Motor neuron diseases have no specific treatment or cure. However, researchers continue to look for safe, effective treatments.
Care provided by a team of several types of health care practitioners (a multidisciplinary team) helps people cope with progressive disability. Physical therapy helps people maintain muscle strength and keep joints flexible and thus helps prevent contractures. Nurses or other caregivers must feed people with swallowing difficulties carefully to prevent choking. Some people must be fed through a tube inserted through the abdominal wall into the stomach (gastrostomy tube).
Certain medications can help relieve symptoms:
Baclofen may help make muscles less spastic. Baclofen may help make muscles less spastic.
Phenytoin or quinine may help decrease cramps. Phenytoin or quinine may help decrease cramps.
Medications with anticholinergic effects, such as glycopyrrolate, may be used to reduce drooling because one anticholinergic effect is to reduce saliva formation. , such as glycopyrrolate, may be used to reduce drooling because one anticholinergic effect is to reduce saliva formation.
Amitriptyline or fluvoxamine (antidepressants) may help people who have changeable emotions or depression. A medication that combines dextromethorphan (a cough suppressant) with quinidine may help control changeable emotions.Amitriptyline or fluvoxamine (antidepressants) may help people who have changeable emotions or depression. A medication that combines dextromethorphan (a cough suppressant) with quinidine may help control changeable emotions.
In some people with amyotrophic lateral sclerosis, riluzole, a medication that protects nerve cells, can prolong life for a few months. It is taken by mouth. Edaravone, a newer medication, may slow the decline in function to some degree in people with amyotrophic lateral sclerosis. Sodium phenylbutyrate/taurursodiol appears to slow the decline in the ability to function, as does tofersen, an In some people with amyotrophic lateral sclerosis, riluzole, a medication that protects nerve cells, can prolong life for a few months. It is taken by mouth. Edaravone, a newer medication, may slow the decline in function to some degree in people with amyotrophic lateral sclerosis. Sodium phenylbutyrate/taurursodiol appears to slow the decline in the ability to function, as does tofersen, anantisense therapy, which also slows progression of the disease. It must be given by injection into a vein (intravenously, IV), into a muscle (intramuscularly, IM). Tofersen must be injected into the space around the spinal cord (intrathecal injection)., which also slows progression of the disease. It must be given by injection into a vein (intravenously, IV), into a muscle (intramuscularly, IM). Tofersen must be injected into the space around the spinal cord (intrathecal injection).
If pain develops as the disease progresses (for example, if pain occurs when a person has to sit in one position too long), benzodiazepines, which are mild sedatives, may be used.
Surgery to improve swallowing helps only a few people with progressive bulbar palsy.
Because amyotrophic lateral sclerosis and progressive bulbar palsy are progressive and incurable, people who have one of these diseases are advised to establish advanced directives that specify what kind of care they want at the end of life.





