

Immunoglobulin A (IgA) nephropathy is deposition of IgA immune complexes in glomeruli, manifesting as slowly progressive hematuria, proteinuria, and, often, chronic kidney disease. Diagnosis is based on urinalysis and renal biopsy. Treatment options include angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), corticosteroids and sometimes other immunosuppressants. Prognosis is generally good.
(See also Overview of Nephritic Syndrome.)
IgA nephropathy is a nephritic syndrome, a form of chronic glomerulonephritis characterized by the deposition of IgA immune complexes in glomeruli. It is the most common form of glomerulonephritis worldwide and is more common in Asian and certain European countries than in African and South American countries (1). It occurs at all ages, with a peak onset in the 20s and 30s, and generally affects males more than females, though prevalence varies throughout the world (2, 3). A substantial number of healthy people have IgA kidney deposits, but not all people with IgA deposits develop clinical disease.
Cause is unknown, but evidence suggests that there may be several mechanisms, including:
Increased IgA1 production
Defective IgA1 glycosylation causing increased binding to mesangial cells
Decreased IgA1 clearance
A defective mucosal immune system
Overproduction of cytokines stimulating mesangial cell proliferation
Familial clustering has also been observed, suggesting genetic factors at least in some cases.
Kidney function is initially normal, but symptomatic kidney disease may develop. A few patients present with acute kidney injury or chronic kidney disease, severe hypertension, or nephrotic syndrome.
General references
1. Schena FP, Nistor I. Epidemiology of IgA Nephropathy: A Global Perspective. Semin Nephrol 2018;38(5):435-442. doi:10.1016/j.semnephrol.2018.05.013
2. Goto K, Imaizumi T, Hamada R, et al. Renal pathology in adult and paediatric population of Japan: review of the Japan renal biopsy registry database from 2007 to 2017. J Nephrol 2023;36(8):2257-2267. doi:10.1007/s40620-023-01687-9
3. Lee M, Suzuki H, Nihei Y, Matsuzaki K, Suzuki Y. Ethnicity and IgA nephropathy: worldwide differences in epidemiology, timing of diagnosis, clinical manifestations, management and prognosis. Clin Kidney J 2023;16(Suppl 2):ii1-ii8. doi:10.1093/ckj/sfad199
Symptoms and Signs of IgA Nephropathy
The most common manifestations are persistent or recurrent macroscopic hematuria or asymptomatic microscopic hematuria with mild proteinuria. Flank pain and low-grade fever may accompany acute episodes. Other symptoms are usually not prominent.
Gross hematuria usually begins 1 or 2 days after a febrile mucosal (upper respiratory, sinus, enteral) illness, thus mimicking acute postinfectious glomerulonephritis, except the onset of hematuria is earlier (coinciding with or immediately after the febrile illness). When this occurs with an upper respiratory illness, it is sometimes referred to as synpharyngitic hematuria.
Rapidly progressive glomerulonephritis is the initial manifestation in approximately 5% of patients (1).
Symptoms and signs reference
1. Shimizu A, Takei T, Moriyama T, Itabashi M, Uchida K, Nitta K. Clinical and pathological studies of IgA nephropathy presenting as a rapidly progressive form of glomerulonephritis. Intern Med 2013;52(22):2489-2494. doi:10.2169/internalmedicine.52.0420
Diagnosis of IgA Nephropathy
Urinalysis
Renal biopsy
Diagnosis is suggested by any of the following:
Gross hematuria, particularly within 2 days of a febrile mucosal illness or with flank pain
Incidentally noted findings on urinalysis
Occasionally, rapidly progressive glomerulonephritis
When manifestations are moderate or severe, diagnosis is confirmed by biopsy.
Urinalysis demonstrates microscopic hematuria, usually with dysmorphic red blood cells (RBCs) and occasionally RBC casts. Mild proteinuria (< 1 g/day) is typical and may occur without hematuria; nephrotic syndrome develops in approximately 10% (1). Serum creatinine level is usually normal.

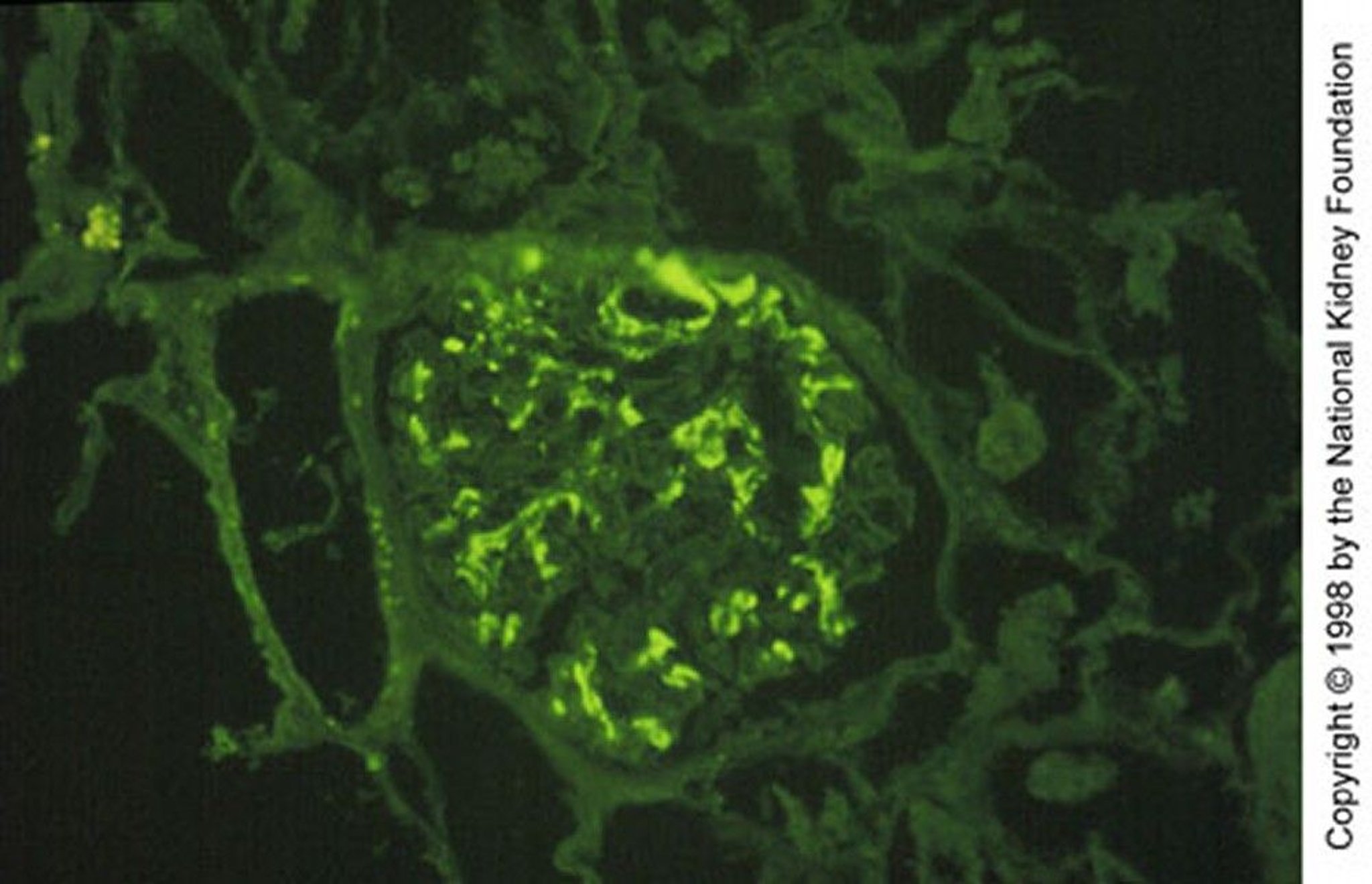
Immunofluorescent staining with anti-IgA demonstrates granular mesangial IgA deposition (×200).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).

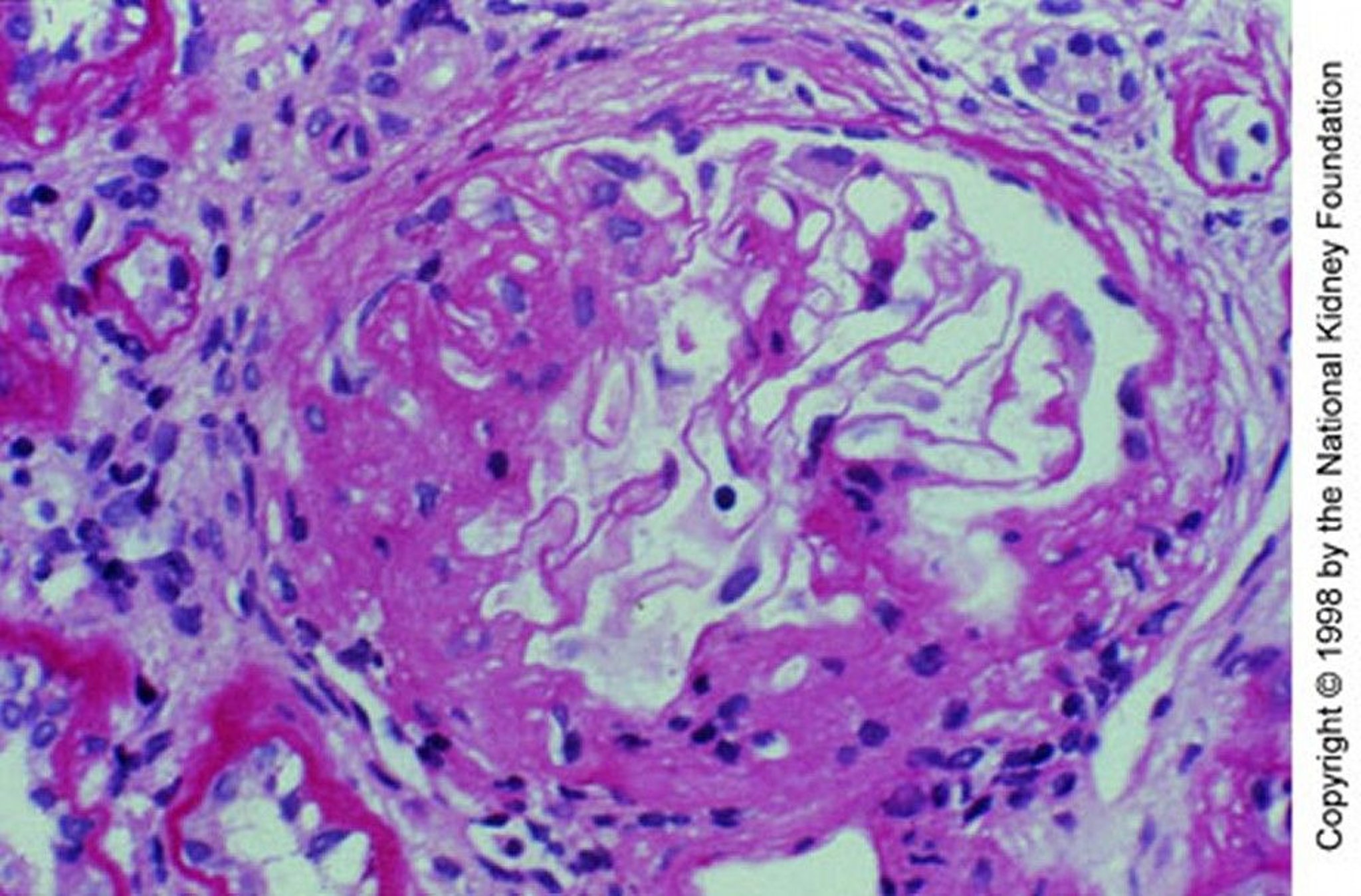
Mesangial expansion with segmental sclerosis (periodic acid-Schiff stain, ×200).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Renal biopsy shows granular deposition of IgA and complement (C3) on immunofluorescent staining in an expanded mesangium with foci of segmental proliferative or necrotizing lesions. Importantly, mesangial IgA deposits are nonspecific and also occur in many other disorders, including immunoglobulin A vasculitis, cirrhosis, inflammatory bowel disease, celiac disease, psoriasis, HIV infection, lung cancer, and several systemic rheumatic diseases.
Glomerular IgA deposition is a primary feature of immunoglobulin A vasculitis, and it may be indistinguishable from IgA nephropathy based on biopsy specimens, leading to speculation that immunoglobulin A vasculitis may be a systemic form of IgA nephropathy. However, immunoglobulin A vasculitis is clinically distinct from IgA nephropathy, usually manifesting as hematuria, purpuric rash, arthralgias, and abdominal pain.
Other serum immunologic tests are usually unnecessary. Complement concentrations are usually normal. Plasma IgA concentration may be elevated, and circulating IgA-fibronectin complexes are present; however, these findings are not helpful diagnostically.
Diagnosis reference
1. Kim JK, Kim JH, Lee SC, et al. Clinical features and outcomes of IgA nephropathy with nephrotic syndrome. Clin J Am Soc Nephrol 2012;7(3):427-436. doi:10.2215/CJN.04820511
Treatment of IgA Nephropathy
Often angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs) for hypertension, serum creatinine > 1.2 mg/dL (106.08 micromol/L), or macroalbuminuria (urinary protein > 300 mg/day) and with a target urinary protein of < 500 mg/day
A dual endothelin angiotensin receptor antagonists (eg, sparsentan) is indicated for patients at risk of rapid disease progressionA dual endothelin angiotensin receptor antagonists (eg, sparsentan) is indicated for patients at risk of rapid disease progression
A sodium-glucose cotransporter 2 (SGLT2) inhibitor may be added for persistent proteinuria despite angiotensin inhibition
Corticosteroids for progressive disease, including increasing proteinuria, especially into the nephrotic range (≥ 3 g/day), and increasing serum creatinine level
Corticosteroids and cyclophosphamide for proliferative injury or Corticosteroids and cyclophosphamide for proliferative injury orrapidly progressive glomerulonephritis
Transplantation in advanced disease
Patients who are normotensive and have intact kidney function (serum creatinine < 1.2 mg/dL [106.08 micromol/L]) and only mild proteinuria (< 0.5 g/day) usually are not treated beyond angiotensin inhibition (with an ACE inhibitor or ARB) and an SGLT2 inhibitor. Patients with more severe kidney disease or more severe proteinuria and hematuria are usually offered corticosteroids, which ideally should be started before significant kidney disease develops.
Angiotensin inhibition in IgA nephropathy
ACE inhibitors or ARBs are used on the premise that they reduce blood pressure, proteinuria, and glomerular fibrosis. Patients with the DD genotype for the ACE gene may be at greater risk of disease progression but may also be more likely to respond to ACE inhibitors or ARBs. For patients with hypertension, ACE inhibitors or ARBs are the antihypertensives of choice even for relatively mild chronic kidney disease.
Dual endothelin receptor antagonists
Sparsentan, a dual endothelin receptor antagonist, is used for management of proteinuria in patients with IgA nephropathy who have a risk for rapid disease progression (defined as a urine protein to creatinine ratio of ≥ 1.5). It should not be used as the initial treatment, but rather is the medication of choice when an ACE inhibitor or ARB fails. The ACE inhibitor or ARB should be stopped before starting a duel endothelin receptor antagonist (Sparsentan, a dual endothelin receptor antagonist, is used for management of proteinuria in patients with IgA nephropathy who have a risk for rapid disease progression (defined as a urine protein to creatinine ratio of ≥ 1.5). It should not be used as the initial treatment, but rather is the medication of choice when an ACE inhibitor or ARB fails. The ACE inhibitor or ARB should be stopped before starting a duel endothelin receptor antagonist (1).
Sodium-glucose cotransporter 2 inhibitors
An SGLT2 inhibitor may also be used for patients with proteinuria secondary to IgA nephropathy that has not improved with ACE inhibitors or ARBs. In a pre-specified subgroup analysis of patients with IgA nephropathy, SGLT2 inhibitors (which improve outcomes in patients with proteinuria due to diabetic kidney disease) reduced the risk of chronic kidney disease progression (2).
Corticosteroids and immunosuppressants in IgA nephropathy
For patients at high risk of disease progression (ie, proteinuria ≥ 1 g/day, an estimated glomerular filtration rate [eGFR] of 20 to 120 mL/minute per 1.73 m2 after at least 3 months of supportive therapy), corticosteroids have been shown to slow the rate of progression to kidney failure (3). Higher-dose corticosteroid regimens are associated with more serious adverse events (eg, infection requiring hospitalization).
There is no consensus among experts regarding the optimal corticosteroid regimen other than it be at least 6 months in duration (4).
Because of the risk of adverse effects, corticosteroids should probably be reserved for patients with any of the following:
Worsening or persistent proteinuria (> 1 g/day), especially if in the nephrotic range despite maximal ACE inhibitor or ARB therapy
Increasing serum creatinine level
Combinations of IV corticosteroids and cyclophosphamide plus oral prednisone are used for severe disease, such as proliferative or crescentic (rapidly progressive) nephropathy. Evidence for mycophenolate mofetil is conflicting; it should not be used as first-line treatment. None of these medications, however, prevents recurrence in transplant patients. Immunosuppressive therapy should also be avoided in patients with advanced fibrotic kidney disease, which is not reversible.Combinations of IV corticosteroids and cyclophosphamide plus oral prednisone are used for severe disease, such as proliferative or crescentic (rapidly progressive) nephropathy. Evidence for mycophenolate mofetil is conflicting; it should not be used as first-line treatment. None of these medications, however, prevents recurrence in transplant patients. Immunosuppressive therapy should also be avoided in patients with advanced fibrotic kidney disease, which is not reversible.
Other treatments
Although other interventions have been tried to lower IgA overproduction and to inhibit mesangial proliferation, data supporting any of these are limited or absent, and none can be recommended for routine treatment. These interventions include elimination of gluten, dairy products, eggs, and meat from the diet; tonsillectomy; and IV immune globulin for 3 months followed by intramuscular immune globulin for 6 months. All theoretically reduce IgA production. Heparin, dipyridamole, and statins are just a few examples of in vitro mesangial cell inhibitors.Although other interventions have been tried to lower IgA overproduction and to inhibit mesangial proliferation, data supporting any of these are limited or absent, and none can be recommended for routine treatment. These interventions include elimination of gluten, dairy products, eggs, and meat from the diet; tonsillectomy; and IV immune globulin for 3 months followed by intramuscular immune globulin for 6 months. All theoretically reduce IgA production. Heparin, dipyridamole, and statins are just a few examples of in vitro mesangial cell inhibitors.
For patients who progress to kidney failure, kidney transplantation is preferred over dialysis because of improved long-term disease-free survival. The condition recurs in approximately 30% of graft recipients (5).
Treatment references
1. Rovin BH, Barratt J, Heerspink HJL, et al: Efficacy and safety of sparsentan versus irbesartan in patients with IgA nephropathy (PROTECT): 2-year results from a randomised, active-controlled, phase 3 trial. Lancet 402(10417):2077-2090, 2023. doi:10.1016/S0140-6736(23)02302-4
2. Wheeler DC, Toto RD, Stefánsson BV, et al: A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy. : A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy.Kidney Int 100(1):215-224, 2021. doi: 10.1016/j.kint.2021.03.033
3. Lv J, Wong MG, Hladunewich MA, et al: Effect of oral methylprednisolone on decline in kidney function or kidney failure in patients with IgA nephropathy: The TESTING randomized clinical trial. JAMA 327(19):1888-1898, 2022. doi: 10.1001/jama.2022.5368
4. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int 100(4S):S1-S276, 2021. doi:10.1016/j.kint.2021.05.021
5. Jäger C, Stampf S, Molyneux K, et al: Recurrence of IgA nephropathy after kidney transplantation: Experience from the Swiss transplant cohort study. BMC Nephrol 23(1):178, 2022. doi: 10.1186/s12882-022-02802-x
Prognosis for IgA Nephropathy
IgA nephropathy has a heterogeneous disease course but usually progresses slowly; chronic kidney disease may develop. Patients who are not hypertensive at presentation may develop hypertension. Progression to kidney failure is variable, occurring in 5 to 60% of patients after 10 years (1). When IgA nephropathy is diagnosed in childhood, prognosis is usually good. However, persistent hematuria invariably leads to hypertension, proteinuria, and chronic kidney disease. Risk factors for progressive deterioration in kidney function include the following:
Proteinuria > 1 g/day
Elevated serum creatinine level
Uncontrolled hypertension
Persistent microscopic hematuria
Extensive fibrotic changes in the glomerulus or interstitium
Crescents on biopsy
Prognosis reference
1. Barbour SJ, Coppo R, Zhang H, et al. Evaluating a New International Risk-Prediction Tool in IgA Nephropathy [published correction appears in JAMA Intern Med. 2019 Jul 1;179(7):1007. doi: 10.1001/jamainternmed.2019.2030]. JAMA Intern Med 2019;179(7):942-952. doi:10.1001/jamainternmed.2019.0600
Key Points
Immunoglobulin A (IgA) nephropathy is the most common cause of glomerulonephritis worldwide and is common among young adults in Asian and European countries.
Consider the diagnosis in patients with unexplained signs of glomerulonephritis, particularly when it occurs within 2 days of a febrile mucosal illness or with flank pain.
Treat patients who have creatinine > 1.2 mg/dL (106.08 micromol/L) or proteinuria > 300 mg/day with angiotensin converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs), and subsequently a sodium-glucose cotransporter 2 (SGLT2) inhibitor or a dual endothelin angiotensin receptor antagonist (for patients at risk of rapid disease progression) if proteinuria persists.
Reserve corticosteroids for patients with worsening kidney function or proteinuria (> 1 g/day) despite treatment with an ACE inhibitor or ARB plus an SGLT2 inhibitor, or a dual endothelin angiotensin receptor antagonist.
Treat patients who have proliferative injury or rapidly progressive glomerulonephritis with corticosteroids and cyclophosphamide.Treat patients who have proliferative injury or rapidly progressive glomerulonephritis with corticosteroids and cyclophosphamide.





