



Precocious puberty is onset of sexual maturation before the average age. Diagnosis is by comparison with population standards, radiographs of the left hand and wrist to assess skeletal maturation and check for accelerated bone growth, and measurement of serum levels of gonadotropins and gonadal and adrenal steroids, depending on examination findings and the potential source of hormonal activation. Treatment depends on the cause.
In girls, the first pubertal milestone is typically breast development (thelarche), followed soon after by appearance of pubic hair (pubarche) and axillary hair and later by the first menstrual period (menarche), which traditionally occurs 2 to 3 years after thelarche.
Puberty—When Female Sexual Characteristics Develop
Bars indicate normal ranges. |


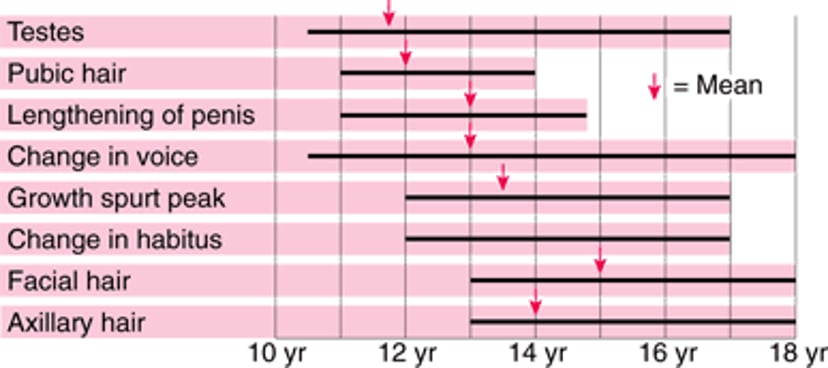
In boys, the first pubertal milestone is typically testicular growth (usually ≥ 4 mL, sometimes 3 mL), followed by penile growth and the appearance of pubic and axillary hair.


This photo shows an orchidometer, which is a tool used to measure testicular growth.
Светлана Назарова/stock.adobe.com
Puberty—When Male Sexual Characteristics Develop
Bars indicate normal ranges. No mean is available for change in habitus. |

Normal puberty starts with activation of the hypothalamic-pituitary-adrenal axis, leading to an increase in adrenal androgen production (eg, dehydroepiandrosterone sulfate [DHEA-S]) called adrenarche. Adrenarche for both girls and boys leads to the development of pubic hair and axillary hair (pubarche), body hair, body odor, and acne.
In girls, gonadarche includes breast development (thelarche), change in body habitus, growth of the uterus, and eventually menarche. In boys, gonadarche includes testicular enlargement and phallic growth.
Although gonadarche and adrenarche may have overlapping signs, they are regulated independently. Pubarche may occur before gonadarche in a minority of children as part of normal pubertal development. (For more information on normal sexual differentiation and pubertal development in females, see Puberty, and in males, see Sexual Differentiation, Adrenarche, and Puberty).
The definition of precocious puberty has traditionally been sexual maturation beginning before age 8 in girls or age 9 in boys. However, the current definition depends on reliable population standards for onset of puberty (ie, when pubertal milestones occur); because onset is occurring earlier in the United States, especially in females, these traditional standards are being reevaluated (1, 2). Breast development is increasingly occurring at younger ages. This trend is mirroring the obesity epidemic, with a higher body mass index (> 85th percentile) associated with earlier thelarche. Despite the earlier age of thelarche, the age of menarche has not lowered as drastically, with a mean decrease of only 5 to 6 months over 50 to 70 years, with most of that decrease in the past 30 years (3, 4).
Race and ethnicity have been considered as risk factors for early puberty (5), but concerns have arisen regarding the validity of this approach, both because race is a social construct without biologic or genetic basis, and because race may be a proxy for other variables (eg, obesity, environmental exposures, psychological stress, social determinants of health) (6).
General references
1. Eckert-Lind C, Busch AS, Petersen JH, et al. Worldwide Secular Trends in Age at Pubertal Onset Assessed by Breast Development Among Girls: A Systematic Review and Meta-analysis. JAMA Pediatr. 2020;174(4):e195881. doi:10.1001/jamapediatrics.2019.5881
2. Herman-Giddens ME, Steffes J, Harris D, et al. Secondary sexual characteristics in boys: data from the Pediatric Research in Office Settings Network. Pediatrics. 2012;130(5):e1058-e1068. doi:10.1542/peds.2011-3291
3. Finer LB, Philbin JM. Trends in ages at key reproductive transitions in the United States, 1951-2010. Womens Health Issues. 2014;24(3):e271-e279. doi:10.1016/j.whi.2014.02.002
4. Wang Z, Asokan G, Onnela JP, et al. Menarche and Time to Cycle Regularity Among Individuals Born Between 1950 and 2005 in the US. JAMA Netw Open. 2024;7(5):e2412854. Published 2024 May 1. doi:10.1001/jamanetworkopen.2024.12854
5. Biro FM, Galvez MP, Greenspan LC, et al. Pubertal assessment method and baseline characteristics in a mixed longitudinal study of girls. Pediatrics. 2010;126(3):e583-e590. doi:10.1542/peds.2009-3079
6. Osinubi AA, Lewis-de Los Angeles CP, Poitevien P, Topor LS. Are Black Girls Exhibiting Puberty Earlier? Examining Implications of Race-Based Guidelines. Pediatrics. 2022;150(2):e2021055595. doi:10.1542/peds.2021-055595
Classification of Precocious Puberty
Precocious puberty can be divided into 2 types:
Gonadotropin-releasing hormone (GnRH)–dependent (central precocious puberty)
GnRH-independent (peripheral sex hormone effects)
GnRH-dependent precocious puberty is more common overall and more frequent in girls (1). In GnRH-dependent precocious puberty, the hypothalamic-pituitary axis is activated, resulting in enlargement and maturation of the gonads, development of secondary sexual characteristics, and oogenesis or spermatogenesis.
GnRH-independent precocious puberty is much less common. Secondary sexual characteristics result from high circulating levels of estrogens or androgens, without activation of the hypothalamic-pituitary axis.
Precocious puberty may also be classified by whether gonadarche or adrenarche occurs.
Incomplete or unsustained pubertal development is common, most often as isolated premature thelarche or adrenarche. Girls with premature thelarche typically display breast development during the first 2 years of life, but this change is not accompanied by pubertal hormone levels, menarche, advanced bone age on radiograph, androgen effects, or growth acceleration. Isolated premature adrenarche is likewise not associated with progressive pubertal development.
Children with premature adrenarche may have signs of adrenal androgen production (eg, pubic hair, acne, body odor) that progress slowly usually without acceleration of linear growth. Premature adrenarche may be associated with later development of polyendocrine metabolic ovarian syndrome in adolescence (2).
Classification references
1. Cheuiche AV, da Silveira LG, de Paula LCP, Lucena IRS, Silveiro SP. Diagnosis and management of precocious sexual maturation: an updated review. Eur J Pediatr. 2021;180(10):3073-3087. doi:10.1007/s00431-021-04022-1
2. Rosenfield RL. Normal and Premature Adrenarche. Endocr Rev. 2021;42(6):783-814. doi:10.1210/endrev/bnab009
Etiology of Precocious Puberty
GnRH-dependent precocious puberty
In most affected girls, a specific cause cannot be identified (1). In the absence of specific symptoms or signs of central nervous system disease, the probability of an intracranial anomaly depends on younger age of onset of puberty (< 6 years in girls) and sex of the child (more common among boys) (2).
Overall, affected boys are more likely to have identifiable cranial pathology than girls (13% vs 2% in a study of 205 children) (3). Such lesions include intracranial tumors, especially of the hypothalamus or pineal gland region, including hamartomas, gliomas, germinomas, and adenomas. These lesions are uncommon and often accompanied by central nervous system symptoms (eg, visual changes, severe headaches).
Neurofibromatosis and a few other rare disorders have also been linked to precocious puberty. Several genetic syndromes are also associated with precocious puberty, including Russell-Silver syndrome.
GnRH-dependent precocious puberty can also arise from iatrogenic causes (eg, surgery, radiation, or chemotherapy for cancer).
A family history of GnRH-dependent precocious puberty is another risk factor (4). Mutations have been identified in several genes to date (eg, MKRN3, DLK1, KISS1), but monogenic causes are rare (1). The increasing incidence of GnRH-dependent precocious puberty suggests a strong role of environmental factors (eg, increased rates of obesity and adiposity, endocrine disrupting chemicals).
GnRH-independent precocious puberty
The etiology of GnRH-independent precocious puberty depends on the predominant sex hormone effect (estrogenic or androgenic), and physical changes are often markedly discordant from normal pubertal development.
Estrogenic effects are most commonly caused by follicular ovarian cysts; other causes include granulosa-theca cell tumors and McCune-Albright syndrome (a triad of follicular cysts, polyostotic fibrous dysplasia, and café-au-lait macules).
Adrenal enzyme defects, specifically 21-hydroxylase deficiency congenital adrenal hyperplasia, are the most common pathologic form of androgen excess in children of either sex (5, 6).
Additional causes of GnRH-independent precocious puberty in boys include familial male gonadotropin-independent precocity (due to an activating mutation of the gene for luteinizing hormone [LH] receptors), testosterone-producing testicular tumors, rarely ectopic beta-human chorionic gonadotropin (beta-hCG) production from certain tumors, which activates LH receptors in testes, and occasionally McCune-Albright syndrome. Unintentional exogenous exposure to transdermal testosterone used by adults can also be an overlooked cause of gonadotropin-independent precocity.
Etiology references
1. Cheuiche AV, da Silveira LG, de Paula LCP, Lucena IRS, Silveiro SP. Diagnosis and management of precocious sexual maturation: an updated review. Eur J Pediatr. 2021;180(10):3073-3087. doi:10.1007/s00431-021-04022-1
2. Zevin EL, Eugster EA. Central precocious puberty: a review of diagnosis, treatment, and outcomes. Lancet Child Adolesc Health. 2023;7(12):886-896. doi:10.1016/S2352-4642(23)00237-7
3. Hansen AB, Renault CH, Wøjdemann D, et al. Neuroimaging in 205 consecutive Children Diagnosed with Central Precocious Puberty in Denmark. Pediatr Res. 2023;93(1):125-130. doi: 10.1038/s41390-022-02047-2
4. Tinano FR, Canton APM, Montenegro LR, et al. Clinical and Genetic Characterization of Familial Central Precocious Puberty. J Clin Endocrinol Metab. 2023;108(7):1758-1767. doi:10.1210/clinem/dgac763
5. Esquivel-Zuniga MR, Kirschner CK, McCartney CR, Burt Solorzano CM. Non-PCOS Hyperandrogenic Disorders in Adolescents. Semin Reprod Med. 2022;40(1-02):42-52. doi:10.1055/s-0041-1742259
6. Idkowiak J, Elhassan YS, Mannion P, et al. Causes, patterns and severity of androgen excess in 487 consecutively recruited pre- and post-pubertal children. Eur J Endocrinol. 2019;180(3):213-221. doi:10.1530/EJE-18-0854
Symptoms and Signs of Precocious Puberty
Physical changes of GnRH-dependent precocious puberty are typically those of normal puberty for a child of that sex, with the exception of age of onset.
In girls, breasts develop, and pubic hair, axillary hair, or both appear. Girls may begin to menstruate. The timing of menstruation occurs 2 to 3 years after breast development. Timing of adrenarche does not impact menstruation.
In boys, facial, axillary, and pubic hair appears and the penis grows, with or without enlargement of testes, depending on the etiology.
Body odor, acne, and behavior changes may develop in either sex.
Pubertal growth spurt is seen in both sexes (with early-mid puberty in females, mid-late puberty in males), but premature closure of the epiphyses results in short adult stature. Ovarian or testicular enlargement occurs in precocious puberty but is absent in isolated premature adrenarche.
Children with precocious puberty may be at increased risk for bullying and psychiatric disorders (including depression, anxiety, attention deficit disorder, eating disorders, and others) (1, 2, 3).
In GnRH-independent precocious puberty, physical changes are often markedly discordant from normal pubertal development and depend on the predominant sex steroid effect (androgenic or estrogenic).
Symptoms and signs references
1. Dinkelbach L, Grasemann C, Kiewert C, Leikeim L, Schmidt B, Hirtz R. Central Precocious Puberty and Psychiatric Disorders. JAMA Netw Open. 2025;8(6):e2516679. doi:10.1001/jamanetworkopen.2025.16679
2. Hueg TK, Lim YH, Holmboe SA, Micali N, Juul A. Precocious Puberty and Risk of Psychiatric Disorders: A Nationwide Cohort Study Using Prospective Registry Data. J Clin Endocrinol Metab. 2026;111(4):e1088-e1096. doi:10.1210/clinem/dgaf567
3. Su Q, Chen Z, Li R, Elgar FJ, Liu Z, Lian Q. Association Between Early Menarche and School Bullying. J Adolesc Health. 2018;63(2):213-218. doi:10.1016/j.jadohealth.2018.02.008
Diagnosis of Precocious Puberty
Bone age radiographs
Serum hormone measurement
Possibly brain MRI or pelvic ultrasound
Diagnosis of precocious puberty is clinical. Radiographs of the left hand and wrist are performed to check for accelerated skeletal maturation as a result of sex hormone effect. Unless history and examination suggest an anomaly, no further evaluation is required for children with pubertal milestones that are within 1 year of population standards. Girls and boys with isolated premature adrenarche and girls with premature thelarche also do not require further evaluation as long as radiographs confirm that skeletal maturation is not accelerated.
Hormonal testing
When further evaluation is necessary, blood tests should be chosen according to the features present.
For patients with suspected GnRH-dependent precocious puberty based on evidence of gonadal changes (eg, thelarche or testicular enlargement), luteinizing hormone (LH) should be measured along with sex-specific gonadal steroid (estradiol in females, testosterone in males). LH levels should be measured using high-sensitivity assays designed for pediatric patients, preferably in the morning. Measurement of morning LH levels is the best initial biochemical test for the diagnosis of GnRH-dependent precocious puberty, with values > 0.2 to 0.3 mIU/L (> 0.2 to 0.3 units/L) considered pubertal (1), depending on the assay. This measurement can differentiate between GnRH-dependent precocious puberty and GnRH-independent causes of precocious puberty. It can also help to determine whether patients with equivocal examination findings (eg, differentiation of true breast tissue from lipomastia in female with elevated body mass index [BMI]) are in central precocious puberty.
A GnRH stimulation test using the GnRH agonist leuprolide may be considered to confirm suspected GnRH-dependent precocious puberty when initial LH levels are inconclusive in children with clinically progressive puberty. GnRH stimulation tests can be performed because a GnRH agonist has an initial stimulatory effect on gonadotropins. To assess its initial stimulatory effect on gonadotropins, leuprolide acetate is given subcutaneously, and LH, follicle-stimulating hormone (FSH), testosterone (only in boys), and estradiol (only in girls) are measured at 0, 1, and 2 hours. At 24 hours after administration of leuprolide, estradiol level may be measured to improve sensitivity of the testing strategy and is considered pubertal if > 50 pg/mL [> 184 pmol/L]) (2). Post-leuprolide 24-hour testosterone levels may be measured in males, but no consensus exists on what constitutes a pubertal level (eg, one study reported > 25 ng/dL (0.87 nmol/L) as pubertal) (3).
In GnRH-dependent precocious puberty, gonadotropin responses are pubertal, with stimulated LH levels > 5.00 mIU/L (> 5 units/L) (1). In GnRH-independent precocious puberty, gonadotropin responses to leuprolide are prepubertal, and a peripheral cause of precocious puberty should be considered.
For patients who have mainly androgen effects, the most useful initial tests include measurements of total testosterone, DHEA-S, 17-hydroxyprogesterone, and pediatric LH.
For patients who have only estrogen effects, the most useful screens for girls include ultrasensitive LH and estradiol. Although precocious puberty with primarily estrogen effects is rare for boys, diagnostic testing should include LH, beta-human chorionic gonadotropin, and estradiol in such cases.
Estradiol and total testosterone levels are the sex hormone measurements of choice. However, estradiol and testosterone levels must be interpreted with caution. While higher levels are often found in precocious puberty, low or prepubertal levels do not exclude the diagnosis as these assays may not be sufficiently sensitive to identify precocious puberty.
FSH levels have more limited usefulness in differentiating children with GnRH-dependent precocious puberty from children with nonprogressive variants.
Imaging
MRI of the brain may be performed to exclude intracranial anomalies in females < 6 years of age, in males with GnRH-dependent precocious puberty, or in any child with GnRH-dependent precocious puberty who has central symptoms (eg, headaches, visual changes). Routine MRI scanning is not necessary in asymptomatic females from ages 6 to 8 years with GnRH-dependent precocious puberty given lower rates of intracranial lesions (up to 3%) from ages 6 to 8 years of age compared to females < 6 years of age (prevalence 25%) (4).
In patients with GnRH-independent puberty, pelvic and adrenal ultrasound may be useful if ovarian, testicular, or adrenal steroid levels are elevated. G
Other testing
Genetic testing may be considered in familial cases of GnRH-dependent precocious puberty (5).
Diagnosis references
1. Bangalore Krishna K, Fuqua JS, et al: Use of Gonadotropin-Releasing Hormone Analogs in Children: Update by an International Consortium. Horm Res Paediatr. 2019;91(6):357-372. doi: 10.1159/000501336
2. Sathasivam A, Garibaldi L, Shapiro S, et al: Leuprolide stimulation testing for the evaluation of early female sexual maturation. Clin Endocrinol (Oxf). 2010;73(3):375-381. doi: 10.1111/j.1365-2265.2010.03796.x
3. Rosenfield RL, Bordini B, Yu C. Comparison of detection of normal puberty in boys by a hormonal sleep test and a gonadotropin-releasing hormone agonist test. J Clin Endocrinol Metab. 2012;97(12):4596-4604. doi:10.1210/jc.2012-2722
4. Cantas-Orsdemir S, Garb JL, Allen HF. Prevalence of cranial MRI findings in girls with central precocious puberty: a systematic review and meta-analysis. J Pediatr Endocrinol Metab. 2018;31(7):701-710. doi:10.1515/jpem-2018-0052
5. Tinano FR, Canton APM, Montenegro LR, et al. Clinical and Genetic Characterization of Familial Central Precocious Puberty. J Clin Endocrinol Metab. 2023;108(7):1758-1767. doi:10.1210/clinem/dgac763
Treatment of Precocious Puberty
For GnRH-dependent precocious puberty, GnRH agonist therapy
For GnRH-independent precocious puberty, androgen or estrogen antagonist therapy
Rarely tumor excision
If pubertal milestones are within 1 year of population standards, reassurance and regular reexamination are sufficient. Treatment is not needed for premature adrenarche or thelarche, but regular reexamination is warranted to check for later development of precocious puberty.
GnRH-dependent precocious puberty
For GnRH-dependent precocious puberty, pituitary LH and FSH secretion can be suppressed with GnRH agonists (1). After initial transient stimulation of LH and FSH, long acting depot preparations of GnRH agonists work through complete but reversible suppression of the pituitary axis. The decision to treat with GnRH agonists depends on the age of the patient, rate of pubertal progression, height velocity, and rate of skeletal maturation on bone age radiograph. GnRH agonists may be used to preserve adult height, with younger children (girls < 7 years of age and boys < 9 years of age) with more rapid progression of pubertal changes benefiting more, and to potentially relieve psychosocial stress (data are more limited to support the potential impact of this intervention). The decision to stop treatment should be individualized and should be around the age when peers are concurrently progressing through puberty.
Treatment regimens include leuprolide acetate injections (subcutaneous or IM), triptorelin injections (IM), or histrelin implants, among others (1, 2, 3). Responses to treatment must be monitored every 3 to 6 months and medication dosages modified accordingly, usually up to age 11 years in girls and age 12 years in boys.
In girls with McCune-Albright syndrome, aromatase inhibitors, such as letrozole and anastrozole, have been used with varying success to reduce estradiol (4).
GnRH-independent precocious puberty
If GnRH-independent precocious puberty in boys is due to familial male gonadotropin-independent precocity, androgen antagonists (eg, spironolactone) combined with a third-generation aromatase inhibitor ameliorate the effects of excess androgen (4). Aromatase inhibitors have been used in the management of gonadotropin-independent precocity in McCune-Albright syndrome, but only letrozole has been shown to be effective in its treatment (4). The antifungal ketoconazole reduces testosterone in boys with familial male gonadotropin-independent precocity. Treatment of 21-hydroxylase congenital adrenal hyperplasia depends on subtype (classical vs nonclassical); individuals with poorly controlled 21-hydroxylase deficiency can also develop GnRH-dependent precocious puberty and require GnRH agonist therapy.
If GnRH-independent precocious puberty is due to a hormone-producing tumor (eg, granulosa-theca cell tumors in girls, testicular tumors in boys), the tumor should be excised. However, girls require extended follow-up to check for recurrence in the contralateral ovary (5, 6).
If GnRH-independent precocious puberty is due to exposure to cutaneous androgen products used by adults, virilization should be transient after the exposure is stopped, and testosterone levels should normalize.
Treatment references
1. Zevin EL, Eugster EA. Central precocious puberty: a review of diagnosis, treatment, and outcomes. Lancet Child Adolesc Health. 2023;7(12):886-896. doi:10.1016/S2352-4642(23)00237-7
2. Krishna KB, Fuqua JS, Rogol AD, et al. Use of gonadotropin-releasing hormone analogs in children: Update by an international consortium. Horm Res Paediatr. 2019;91(6):357-372. doi: 10.1159/000501336
3. Kilberg MJ, Vogiatzi MG. Approach to the Patient: Central Precocious Puberty. J Clin Endocrinol Metab. 2023;108(8):2115-2123. doi: 10.1210/clinem/dgad081
4. Cheuiche AV, da Silveira LG, de Paula LCP, Lucena IRS, Silveiro SP. Diagnosis and management of precocious sexual maturation: an updated review. Eur J Pediatr. 2021;180(10):3073-3087. doi:10.1007/s00431-021-04022-1
5. Aguirre RS, Eugster EA. Central precocious puberty: From genetics to treatment. Best Pract Res Clin Endocrinol Metab. 2018;32(4):343-354. doi: 10.1016/j.beem.2018.05.008
6. Latronico AC, Brito VN, Carel J-C. Causes, diagnosis, and treatment of central precocious puberty. Lancet Diabetes Endocrinol. 2016;4(3):265-274. doi: 10.1016/S2213-8587(15)00380-0
Key Points
Precocious puberty is the onset of sexual maturation before the average age based on population standards.
Most commonly, secondary sexual characteristics develop prematurely because the hypothalamic-pituitary axis is activated (GnRH-dependent, or central, precocious puberty); usually the cause is idiopathic, but sometimes the cause is a central nervous system anomaly.
Less commonly, the cause is high circulating levels of estrogens or androgens (GnRH-independent, or peripheral, precocious puberty) caused by congenital adrenal hyperplasia or various gonadal tumors.
Diagnosis of GnRH-dependent precocious puberty is made by bone age radiographs and measurement of LH and testosterone (in boys), and estradiol (in girls).
Treat GnRH-dependent precocious puberty with GnRH agonists.
Treat GnRH-independent precocious puberty based on the cause, including giving androgen or estrogen antagonists and removing tumors.
Drug Information for the Topic





