



Atrioventricular (AV) septal defect consists of an ostium primum type atrial septal defect and a common AV valve, with or without an associated inlet (AV septal type) ventricular septal defect (VSD). These defects result from maldevelopment of the endocardial cushions. Patients with no VSD component or a small VSD and good AV valve function may be asymptomatic. If there is a large VSD component or significant AV valve regurgitation, patients often have signs of heart failure, including dyspnea with feeding, poor growth, tachypnea, and diaphoresis. Heart murmurs, tachypnea, tachycardia, and hepatomegaly are common. Diagnosis is by echocardiography. Treatment is surgical repair for all but the smallest defects.
(See also Overview of Congenital Cardiovascular Anomalies, Atrial Septal Defect, and Ventricular Septal Defect.)
Atrioventricular (AV) septal defect accounts for about 5% of congenital heart anomalies. In the past, this anomaly has been called by different names, such as AV canal defect or endocardial cushion defect. "AV septal defect" has generally been accepted as the preferred designation because the AV septum (septal structure separating the left ventricle from the right atrium) is absent in all forms of this malformation.
An AV septal defect may be
Complete, with a large (nonrestrictive) inlet ventricular septal defect
Transitional, with a small or moderate-sized (restrictive) ventricular septal defect
Partial, with no ventricular septal defect
The majority of patients with the complete form have Down syndrome. AV septal defect is also common among patients with heterotaxy syndromes. Heterotaxy refers to developmental abnormalities of "sidedness" of the thoracic and abdominal organs. Right or left isomerism is usually present. Right isomerism is associated with bilateral right atrial appendages, bilateral right bronchi, tri-lobed lungs, and asplenia. Conversely, left isomerism is associated with bilateral left atrial appendages, bilateral left bronchi, bi-lobed lungs, and polysplenia. Some form of complex congenital heart disease is almost always present in Down syndrome.
Complete AV septal defect
A complete atrioventricular septal defect, also called a complete common AV canal defect (see figure ), consists of a
Large ostium primum atrial septal defect (ASD) in the anteroinferior aspect of the septum
Contiguous nonrestrictive inlet ventricular septal defect
Common AV valve orifice
A complete AV septal defect is a single large central defect in the septation of the heart. A left-to-right shunt occurs at the atrial and ventricular levels and is often large. AV valve regurgitation may be significant, sometimes causing a direct left ventricle-to-right atrial shunt. These abnormalities result in enlargement of all 4 cardiac chambers. Large defects result in direct transmission of the systemic left ventricular pressure to the right ventricle and pulmonary arteries. Hemodynamic findings are similar to those of a large ventricular septal defect (VSD).
If a complete AV septal defect is unrepaired, over time the increase in pulmonary blood flow, pulmonary artery pressure, and pulmonary vascular resistance may lead to reversal of shunt direction with cyanosis and Eisenmenger syndrome.
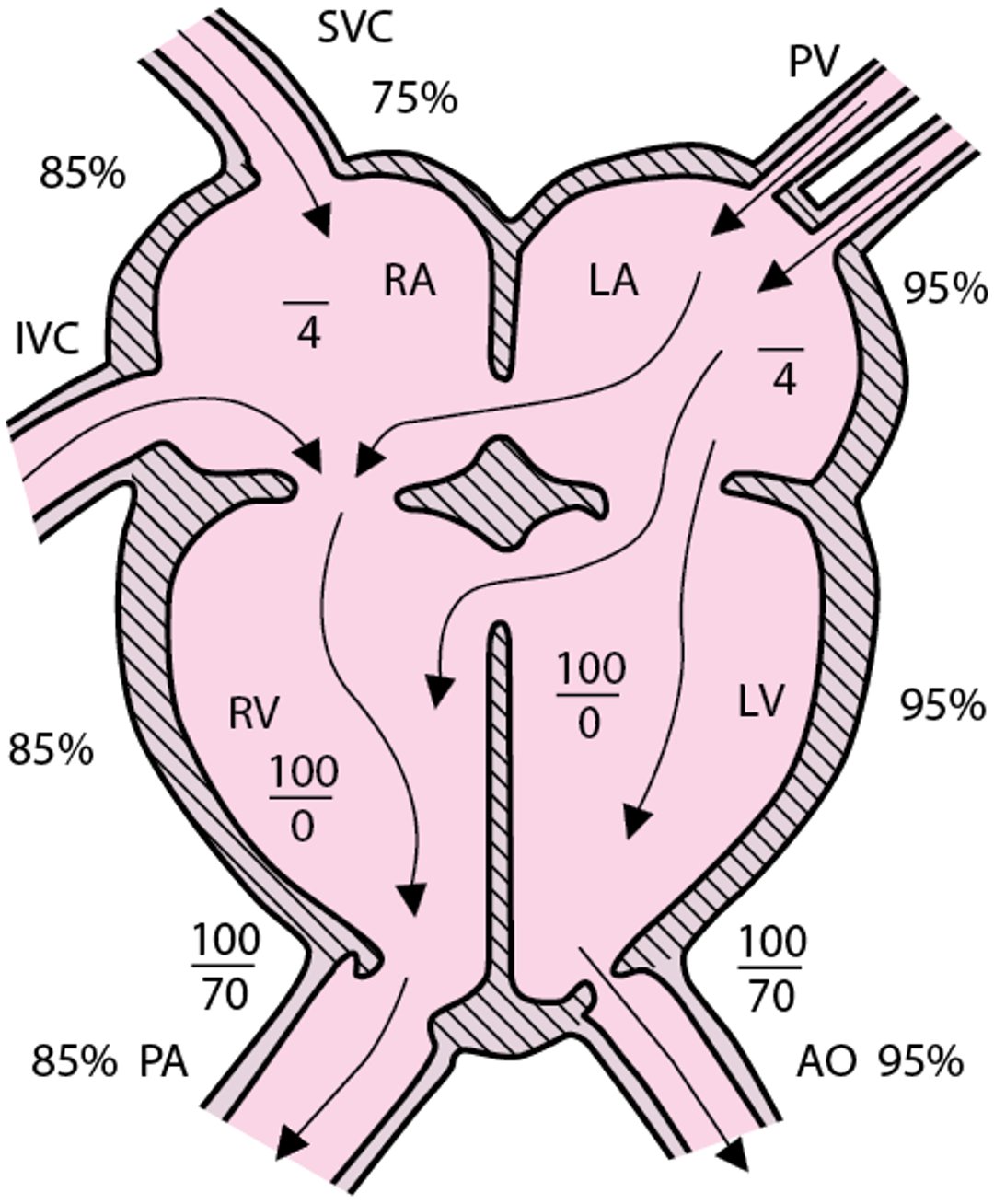
Atrioventricular septal defect (complete form)
Pulmonary blood flow, all chamber volumes, and often pulmonary vascular resistance are increased. Atrial pressures are mean pressures. AO = aorta; IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PV = pulmonary veins; RA = right atrium; RV = right ventricle; SVC = superior vena cava. |

Transitional AV septal defect
A transitional atrioventricular septal defect, also called a transitional AV canal defect, consists of
An ostium primum atrial septal defect
A restrictive inlet ventricular septal defect, which may be small or moderate in size
A common AV valve, which may or may not be partitioned into a left and right orifice
In a transitional AV septal defect, the shunt at the atrial level is usually large. The shunt at the ventricular level is smaller than in complete AV septal defect, and right ventricular pressure is lower than left ventricular pressure. The hemodynamics depend largely on the size of the VSD and whether there is significant AV valve regurgitation.
Partial AV septal defect
A partial AV septal defect consists of
An ostium primum atrial septal defect
Partitioning of the common AV valve into 2 separate AV orifices, resulting in a so-called cleft in the mitral valve (left AV orifice)
The ventricular septum is intact. Hemodynamic abnormalities are similar to those of ostium secundum ASD (eg, left-to-right shunt at the atrial level, enlarged right heart chambers, increased pulmonary blood flow) with the additional finding of variable degrees of AV valve regurgitation.
Unbalanced AV septal defect
In a subset of patients, the common AV valve is positioned more over one ventricle than the other. This condition, referred to as unbalanced AV septal defect, results in one ventricle receiving more blood flow and becoming dominant (larger) and the other ventricle being underdeveloped.
Symptoms and Signs of Atrioventricular Septal Defect
Complete atrioventricular septal defect with a large left-to-right shunt causes signs of heart failure (eg, tachypnea, dyspnea during feeding, poor weight gain, diaphoresis) by age 4 to 6 weeks. Pulmonary vascular obstructive disease (Eisenmenger syndrome) is usually a late complication but may occur earlier, especially in children with Down syndrome.
Partial AV septal defects do not usually cause symptoms during childhood as long as left AV valve regurgitation is mild or absent. However, symptoms (eg, exercise intolerance, fatigue, palpitations) may develop during adolescence or early adulthood. Infants with moderate or severe left AV valve regurgitation often have signs of heart failure.
Patients with transitional AV septal defects may have signs of heart failure if the ventricular septal defect is moderately restrictive with high flow or may be asymptomatic if the ventricular septal defect is highly restrictive (small).
Physical examination in children with complete AV septal defects shows an active precordium due to volume and pressure overload of the right ventricle; a single, loud second heart sound (S2) due to pulmonary hypertension; a grade 2 to 3/6 systolic murmur due to increased flow across the pulmonary outflow tract; and sometimes a diastolic murmur at the apex and low left sternal border related to increased flow across the AV valves (see table ). In patients with persistent elevation of pulmonary vascular resistance, especially those with Down syndrome, there may be no murmur, but a loud single S2 will be present.
Most children with a partial defect have examination findings similar to patients with a secundum ASD, wide splitting of the S2 and a midsystolic (eg, ejection systolic) murmur audible at the upper left sternal border. A mid-diastolic murmur may be present at the lower left sternal border when the atrial shunt is large. A cleft in the left AV valve results in a blowing apical systolic murmur of mitral regurgitation.
Diagnosis of Atrioventricular Septal Defect
Chest x-ray and ECG
Echocardiography
Diagnosis of atrioventricular septal defects is suggested by clinical examination, supported by chest x-ray and ECG, and established by 2-dimensional echocardiography with color flow and Doppler studies.
Chest x-ray shows cardiomegaly with right atrial enlargement, biventricular enlargement, a prominent main pulmonary artery segment, and increased pulmonary vascular markings.
ECG shows a superiorly directed QRS axis (eg, left axis deviation or northwest axis), frequent first-degree AV block, left or right ventricular hypertrophy or both, and occasional right atrial enlargement and right bundle branch block.
Two-dimensional echocardiography with color flow and Doppler studies establishes the diagnosis and can provide important anatomic and hemodynamic information. Cardiac catheterization is not usually necessary unless hemodynamics must be further characterized before surgical repair (eg,, to assess pulmonary vascular resistance in a patient presenting at an older age).
Treatment of Atrioventricular Septal Defect
Surgical repair
For heart failure, medical therapy (eg, diuretics, digoxin, angiotensin-converting enzyme inhibitors) before surgery
Complete atrioventricular septal defect should be repaired by age 2 to 4 months because most infants have heart failure and failure to thrive. Even if infants are growing well without significant symptoms, repair should be done before 6 months to prevent development of pulmonary vascular disease, especially in infants with Down syndrome.
In patients with 2 adequately sized ventricles and no additional defects, the large central defect (combination of the primum ASD and inlet VSD) is closed and the common AV valve is reconstructed into 2 separate valves. Surgical mortality rate is 3 to 4% (1).
Surgical complications include complete heart block (3%), residual ventricular septal defect, and/or left AV valve regurgitation. Less common residual abnormalities include right AV valve regurgitation, left or right AV valve stenosis, or subaortic stenosis.
Pulmonary artery banding may be used as a palliative procedure to delay the timing of open heart repair, particularly in preterm infants or those with associated abnormalities that make complete repair at an early age or low body weight higher risk.
For asymptomatic patients with a partial defect, elective surgery is done at age 1 to 3 years. Surgical mortality rate is very low.
The subset of patients with unbalanced AV septal defect, associated with either a hypoplastic right ventricle or hypoplastic left ventricle, generally are not amenable to a 2-ventricle repair and require operative staging toward a single ventricle circulation, ultimately with a Fontan procedure.
For patients with large shunts and heart failure, diuretics, digoxin, and angiotensin-converting enzyme (ACE) inhibitors may help to manage symptoms before surgery.
Endocarditis prophylaxis is not needed preoperatively and is required only for the first 6 months after repair or if there is a residual defect adjacent to a surgical patch.
Treatment reference
1. Spector LG, Menk JS, Knight JH, et al: Trends in Long-Term Mortality After Congenital Heart Surgery. J Am Coll Cardiol 71(21):2434-2446, 2018. doi:10.1016/j.jacc.2018.03.491
Key Points
An atrioventricular (AV) septal defect may be complete, transitional, or partial; the majority of patients with the complete form have Down syndrome.
A complete AV septal defect involves a large ostium primum atrial septal defect (ASD), a ventricular septal defect (VSD), and a common AV valve (often with significant regurgitation), all resulting in a large left-to-right shunt at both atrial and ventricular levels and enlargement of all 4 cardiac chambers.
A partial AV septal defect also involves an ASD, but the common AV valve is partitioned into 2 separate AV orifices and there is no VSD, resulting in enlargement of the right heart chambers because of a large atrial shunt but no ventricular shunt.
A transitional AV septal defect involves an ostium primum ASD, a common AV valve, and a small- or moderate-size VSD.
Complete AV septal defect with a large left-to-right shunt causes signs of heart failure by age 4 to 6 weeks.
Symptoms in partial AV septal defects vary with the degree of mitral regurgitation; if mild or absent, symptoms may develop during adolescence or early adulthood, but infants with moderate or severe mitral regurgitation often have manifestations of heart failure.
Symptoms in transitional AV septal defect fall on a spectrum, depending on the size of the VSD.
Defects are repaired surgically between age 2 to 4 months or 1 to 3 years, depending on the specific defect and severity of symptoms.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers
Drug Information for the Topic





