



The glenoid labrum usually tears as a result of a specific trauma, such as a fall onto an outstretched arm. Tears can also result from chronic overhead movement, as occurs in pitching. A glenoid labral tear causes pain during motion. Treatment is with physical therapy and sometimes surgery.
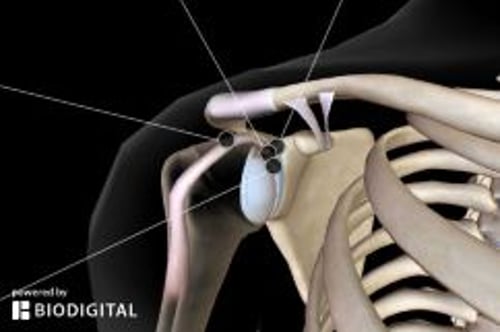
The shoulder (unlike the hip or elbow) is an inherently unstable joint; it has been likened to a golf ball sitting on a tee. To enhance structural stability, the glenoid (anatomically, a very shallow socket) is deepened by the labrum, which is a rubbery, fibrocartilaginous material attached around the rim of the glenoid. This structure can tear during athletics, especially during throwing sports, or as a result of blunt trauma when falling and landing on an outstretched upper extremity.
Symptoms and Signs of Glenoid Labral Tear
A glenoid labral tear results in deep shoulder pain during motion, especially when pitching a baseball. This discomfort may be accompanied by a painful clicking or clunking sensation and a feeling of catching in the shoulder.
Diagnosis of Glenoid Labral Tear
History and physical examination
Usually MR arthrography
A thorough physical examination of the shoulder and neck should be performed initially, but referral to a specialist is frequently needed because more sophisticated diagnostic tests (eg, MR arthrography) are often the only way to definitively identify the pathology (1). A superior labral tear from anterior to posterior (SLAP) and a Bankart tear (anterior) are the most common types of glenoid labral tears.
Diagnosis reference
1. Liu F, Cheng X, Dong J, et al. Imaging modality for measuring the presence and extent of the labral lesions of the shoulder: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2019;20(1):487. Published 2019 Oct 27. doi:10.1186/s12891-019-2876-6
Treatment of Glenoid Labral Tear
Physical therapy
Sometimes surgery
Physical therapy to strengthen the rotator cuff muscles as well as the surrounding shoulder musculature is the initial treatment. If symptoms do not subside with physical therapy, and the diagnosis has been confirmed by contrast-enhanced MRI, surgical debridement or repair is the treatment of choice (1). Surgery is usually performed arthroscopically.

1. Lie on stomach with involved arm hanging off edge of bed with thumb pointed out away from body.
2. Keep elbow straig
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on uninvolved side with pillow between arm and body of the involved side.
2. Bend involved elbow to 90°.
3. Prep
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm down off edge of table and thumb pointed out away from body.
2. Retract and depress
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm out to the side, off edge of bed and elbow bent to 90°.
2. Forearm should be off ed
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Begin with arm at side, keep elbow straight and thumb up.
2. Move arm forward in position approximately 30° to be i
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Hold weight in hand on involved side.
2. Slightly bend hips and knees and support upper body with other hand placed
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.


1. Lie on stomach with involved arm hanging off edge of bed with thumb pointed out away from body.
2. Keep elbow straight and extend arm to trunk level while squeezing the scapula down and back.
3. Return to starting position.
4. Perform 3 sets of 10 repetitions.
5. Add light weight as tolerated.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on uninvolved side with pillow between arm and body of the involved side.
2. Bend involved elbow to 90°.
3. Prepare the scapula by retracting and depressing (squeezing toward spine and downward).
4. Move forearm up by rotating at the shoulder, so the back of the hand is up toward the ceiling.
5. Slowly return to start position and repeat.
6. Perform 3 sets of 10 repetitions, 1 time a day.
7. Add light weight as tolerated.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm down off edge of table and thumb pointed out away from body.
2. Retract and depress the scapula (squeeze toward spine and downward).
3. Lift arm upward to shoulder level.
4. Lower arm toward the floor and repeat.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Do not let shoulder blade move when lifting arm.
b. Keep thumb facing up toward the ceiling.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Lie on stomach with involved arm out to the side, off edge of bed and elbow bent to 90°.
2. Forearm should be off edge of bed with thumb toward the body.
3. Retract and depress the scapula (squeeze toward spine and downward).
4. Rotate forearm upward.
5. Return to start position and repeat.
6. Perform 3 sets of 10 repetitions, 1 time a day.
7. Special Instructions
a. Do not let shoulder blade move when lifting forearm.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Begin with arm at side, keep elbow straight and thumb up.
2. Move arm forward in position approximately 30° to be in the place of the scapula or scaption.
3. In this position raise arm up staying in a pain-free range.
4. Return to starting position.
5. Perform 3 sets of 10 repetition, 1 time a day.
6. Add light weight as tolerated.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3. Grasp band in involved hand, with elbow bent to 90° and thumb up.
4. Externally rotate arm, then slowly return to start position.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Start with least resistance band.
b. Keep arm at side and elbow flexed at 90°.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Place band to secure object at waist level.
2. Place pillow or towel roll between elbow and body on involved side.
3. Grasp band with involved hand, with elbow bent to 90° and thumb up.
4. Internally rotate arm (pull hand inward across body), then slowly return to start position.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Start with least resistance band.
b. Keep arm at side and elbow flexed at 90°.
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.

1. Hold weight in hand on involved side.
2. Slightly bend hips and knees and support upper body with other hand placed on table or bed.
3. Bend elbow to 90° and extend shoulder to raise elbow to shoulder height by retracting (squeezing) the scapula.
4. Return to start position.
5. Perform 3 sets of 10 repetitions, 1 time a day.
6. Special Instructions
a. Start with 1 to 2 pound (0.5 to 1 kg) weight (ie, a soup can).
Courtesy of Tomah Memorial Hospital, Department of Physical Therapy, Tomah, WI; Elizabeth C.K. Bender, MSPT, ATC, CSCS; and Whitney Gnewikow, DPT, ATC.
Treatment reference
1. Ernat JJ, Yheulon CG, Shaha JS. Arthroscopic Repair of 270- and 360-Degree Glenoid Labrum Tears: A Systematic Review. Arthroscopy. 2020;36(1):307-317. doi:10.1016/j.arthro.2019.07.027





