



Fascioliasis is infection with the liver flukes Fasciola hepatica or Fasciola gigantica, which is acquired by eating contaminated watercress or other aquatic plants. Clinical manifestations include abdominal pain and hepatomegaly. Diagnosis is by serology or detection of eggs in feces, duodenal aspirates, or bile specimens. Treatment is with triclabendazole or possibly nitazoxanide.
Flukes are parasitic flatworms that infect various parts of the body (eg, blood vessels, gastrointestinal tract, lungs, liver) depending on the species.
F. hepatica and F. gigantica are the sheep and cattle liver flukes (these animals are the definitive hosts); occasionally these flukes may infect camelids, deer, and buffalo (1, 2). Snails are intermediate hosts. Incidental human fascioliasis is acquired by eating watercress or other aquatic plants contaminated by sheep or cattle dung. It occurs in sheep-rearing regions of Europe (eg, France, Spain, Turkey) and the Middle East, Africa, China, and South America but is rare in the United States. The global prevalence of Fasciola infection (fascioliasis) is estimated to be between 2.4 million and 17 million people (3), with many more at risk of infection.

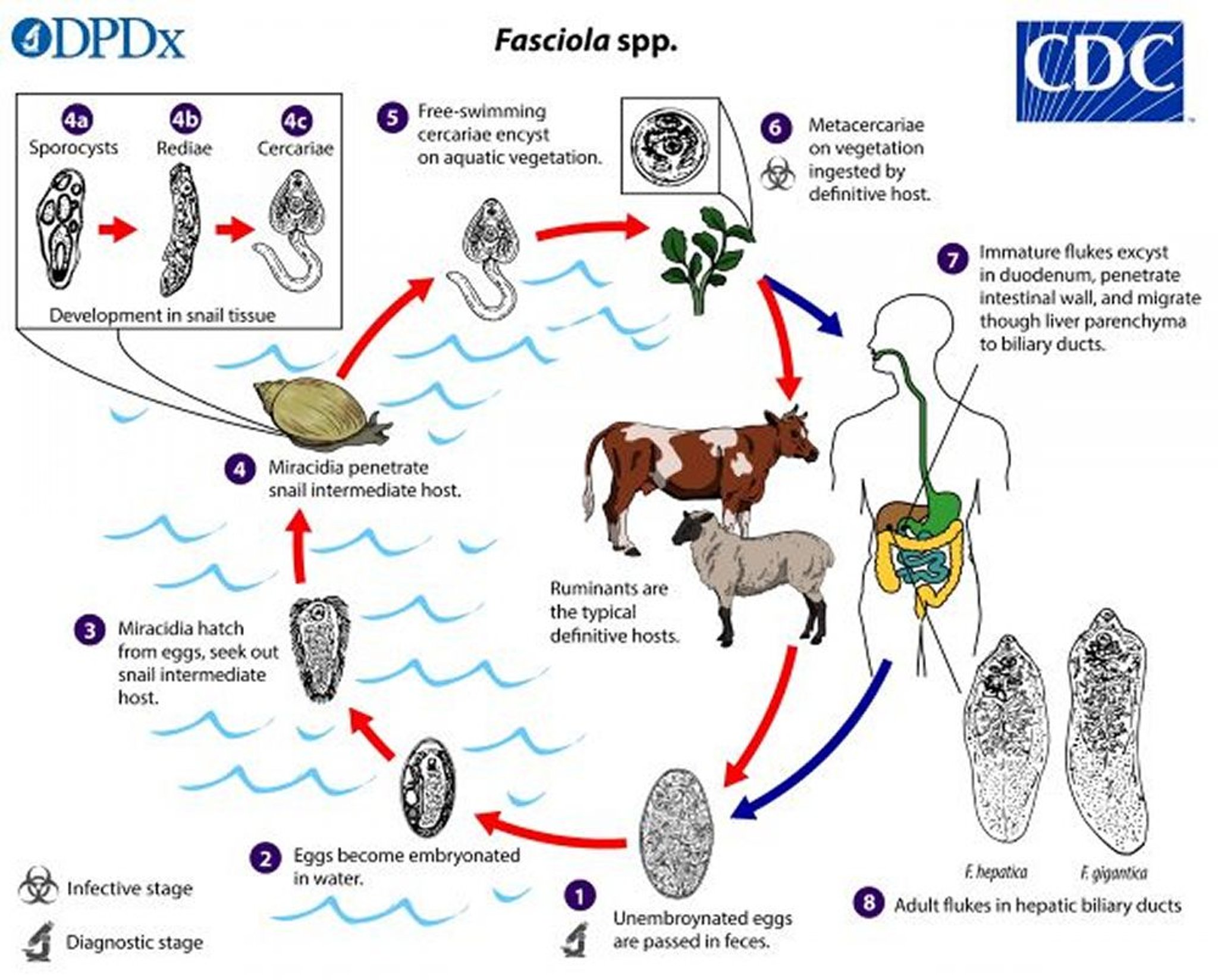
1. Unembryonated eggs are discharged into the biliary ducts and excreted in feces.
2. Eggs become embryonated in water.
3. Eggs release miracidia, which then invade a snail (intermediate host).
4. In the snail, the parasites progress through several developmental stages (sporocysts, rediae, and cercariae).
5. The cercariae are released from the snail and encyst (form cystic structures) as metacercariae on aquatic vegetation or other surfaces.
6. Fascioliasis is acquired by eating plants, especially watercress, containing metacercariae.
7. After ingestion, the metacercariae excyst (rupture out of existing cysts) in the duodenum.
8. They migrate through the intestinal wall, peritoneal cavity, and liver parenchyma into the biliary ducts, where they develop into adult flukes.
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
In acute infection, immature flukes migrate through the intestinal wall, the peritoneal cavity, the liver capsule, and the parenchyma of the liver before entering the biliary ducts where they mature to adulthood in about 3 to 4 months. The adults lay eggs, which are passed through the bile ducts into the duodenum and are then expelled in the feces.
General reference
1. World Health Organization: Neglected tropical diseases: Fascioliasis. July 28, 2020. Accessed July 11, 2025.
2. Centers for Disease Control and Prevention: Liver Flukes: About Fasciola. February 14, 2024. Accessed July 11, 2025.
3. Mas-Coma S, Valero MA, Bargues MD: Fascioliasis. Adv Exp Med Biol 2019;1154:71-103. doi:10.1007/978-3-030-18616-6_4
Symptoms and Signs of Fascioliasis
Acute fascioliasis infection can cause abdominal pain, hepatomegaly, nausea, vomiting, intermittent fever, urticaria, malaise, and weight loss due to liver damage. Eosinophilia is common.
Chronic infection may be asymptomatic or lead to intermittent abdominal pain, cholelithiasis, cholangitis, obstructive jaundice, or pancreatitis. Chronic infection begins to manifest 6 months after exposure and may last 10 years or longer.
Heavy infection can cause secondary sclerosing cholangitis and biliary cirrhosis. Ectopic lesions may occur in the intestinal wall, lungs, or other organs.
Pharyngeal fascioliasis has been reported after consumption of infected raw liver in the Middle East; this syndrome is called halzoun, which may be associated with pharyngitis and pharyngeal edema, contributing to dysphagia and dyspnea. Halzoun is not well characterized, and other pathogens have also been proposed as the etiology (1).
Symptoms and signs reference
1. Khalil G, Haddad C, Otrock ZK, et al: Halzoun, an allergic pharyngitis syndrome in Lebanon: the trematode Dicrocoelium dendriticum as an additional cause. Acta Trop 125(1):115-118, 2013. doi:10.1016/j.actatropica.2012.09.013
Diagnosis of Fascioliasis
Microscopic examination of feces or duodenal or biliary material (obtained via endoscopic examination) for eggs
Serology
Sometimes imaging (abdominal CT, MRI, endoscopic retrograde cholangiopancreatography [ERCP], or ultrasound)
Fascioliasis should be considered in patients with abdominal pain and/or hepatomegaly and a dietary history of watercress or other aquatic plant ingestion or consumption of raw vegetables exposed to contaminated water.
When fascioliasis is suspected, patients should have feces examination for eggs and a serum antibody assay. The eggs are difficult to distinguish from those of Fasciolopsis buski. Supportive findings on blood and imaging tests done for evaluation of abdominal symptoms include anemia, eosinophilia, abnormal liver tests, elevated erythrocyte sedimentation rate, and hypergammaglobulinemia, and hypodense lesions in the liver on CT scan during the acute stage of fascioliasis.
If feces examination and antibody testing are negative or equivocal but fascioliasis is still suspected (ie, based on numerous supportive findings, particularly eosinophilia), then endoscopy with duodenal and biliary aspiration should be done. Eggs and sometimes adult worms may be detected in specimens obtained during endoscopy of the duodenum and/or around the biliary duct.


Fasciola species eggs are broadly ellipsoidal and operculated (one end has a lid-like covering) and measure 130 to 150 micrometers long by 60 to 90 micrometers wide. Fasciola species eggs can be difficult to distinguish from Fasciolopsis buski eggs, but the abopercular ends (the end opposite the opercular end) of Fasciola species eggs often have a roughened or irregular area.
Fasciola species eggs are passed unembryonated in feces.
CDC/DPDx
Serology based on antibody detection assays is particularly useful in:
The early stages of infection before eggs are produced (egg production typically begins at least 3 to 4 months after exposure)
Chronic infection when egg production is sporadic or low
Loss of detectable antibodies occurs 6 to 12 months after cure.
Serological tests based on enzyme-linked immunosorbent assay (ELISA) that use Fasciola-specific antigens are available globally. In the United States, the standard method involves an enzyme immunoassay (EIA) using excretory-secretory or recombinant antigens, followed by confirmatory testing with an immunoblot assay for EIA-positive samples. The Centers for Disease Control and Prevention (CDC) has developed an immunoblot assay for fascioliasis, utilizing a recombinant F. hepatica antigen (FhSAP2), characterized by high sensitivity and specificity (1, 2). It should be noted that F. gigantica eggs are often not detected in the feces; serologic (antigen-based) tests are preferred.
In endemic areas, eggs can also be seen in feces after ingestion of infected animal livers, which are not infective for humans, resulting in a misdiagnosis of fascioliasis. Thus, patients should be asked to follow a liver-free diet for several days before their feces are examined.
Ultrasound, CT, MRI, ERCP, or cholangiography can detect biliary tract abnormalities in chronic disease.
Diagnosis references
1. Centers for Disease Control and Prevention: DPDx–Laboratory Identification of Parasites of Public Health Concern: Fascioliasis. May 2, 2019. Accessed July 1, 2025.
2. Shin SH, Hsu A, Chastain HM, et al: Development of Two FhSAP2 Recombinant-Based Assays for Immunodiagnosis of Human Chronic Fascioliasis. Am J Trop Med Hyg 2016;95(4):852-855. doi:10.4269/ajtmh.16-0253
Treatment of Fascioliasis
Triclabendazole or possibly nitazoxanide
Treatment of fascioliasis for patients ≥ 6 years of age is with 2 doses of triclabendazole given 12 hours apart, orally with food (1). Nitazoxanide orally twice a day for 7 days may be effective, but the data are limited.
Praziquantel is not recommended due to the high likelihood of treatment failure.
In some patients, extraction of adult flukes from the biliary tract by ERCP may be useful to reduce worm load and, therefore, symptoms.
Prevention involves not eating watercress or other freshwater plants in regions where F. hepatica is endemic. Family members of infected people should be evaluated for fascioliasis.
Treatment reference
1. Gandhi P, Schmitt EK, Chen CW, Samantray S, Venishetty VK, Hughes D: Triclabendazole in the treatment of human fascioliasis: a review. Trans R Soc Trop Med Hyg 2019;113(12):797-804. doi:10.1093/trstmh/trz093
Drug Information for the Topic





