



Chronic cholecystitis is long-standing gallbladder inflammation almost always due to gallstones. Treatment is with cholecystectomy.
(See also Overview of Biliary Function.)
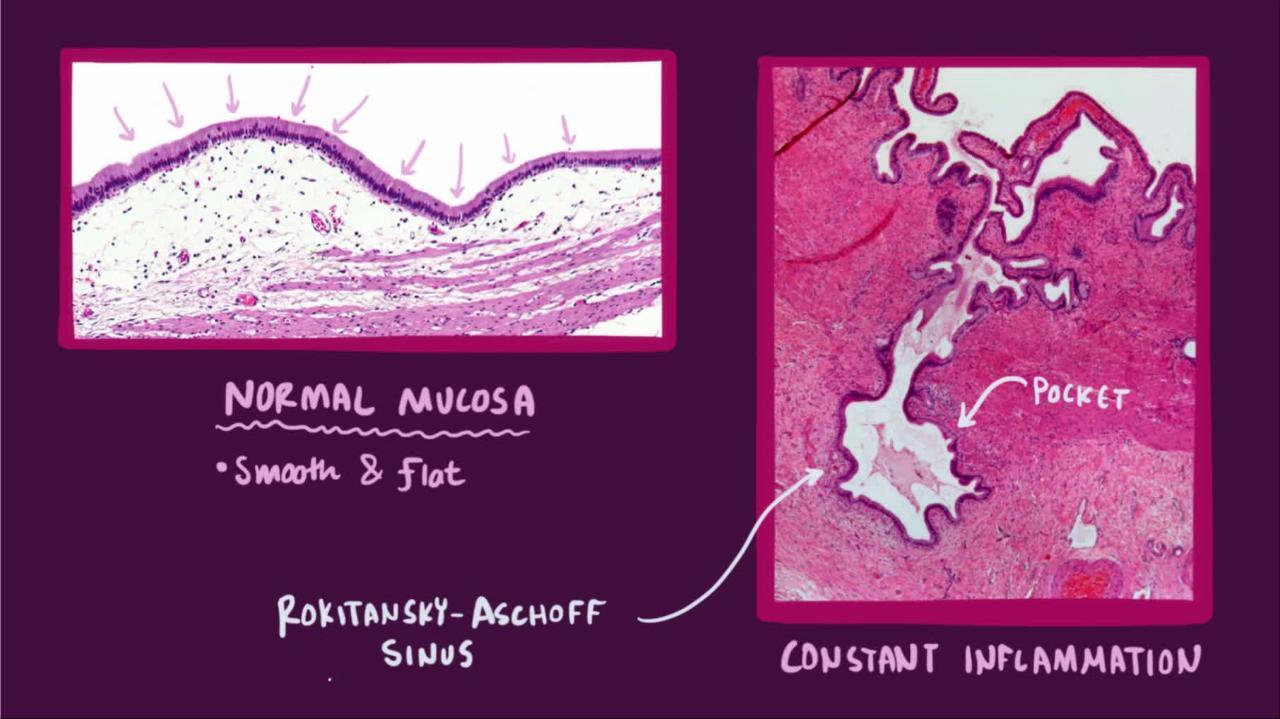
Chronic cholecystitis almost always results from gallstones and prior episodes of acute cholecystitis (even if mild). Damage ranges from a modest infiltrate of chronic inflammatory cells to a fibrotic, shrunken gallbladder. Extensive calcification due to fibrosis is called porcelain gallbladder.

Symptoms and Signs of Chronic Cholecystitis
Gallstones intermittently obstruct the cystic duct and so cause recurrent biliary colic. Such episodes of pain are not necessarily accompanied by overt gallbladder inflammation and acute cholecystitis; the extent of inflammation does not correlate with the intensity or frequency of biliary colic. Upper abdominal tenderness may be present, but usually fever is not. Fever suggests acute cholecystitis. Once episodes begin, they are likely to recur.
Diagnosis of Chronic Cholecystitis
Ultrasound
Sometimes cholescintigraphy
Laboratory testing
Chronic cholecystitis is suspected in patients with recurrent biliary colic plus gallstones. Ultrasound or another imaging test usually shows gallstones and sometimes a shrunken, fibrotic gallbladder. The diagnosis is made in patients with a history of recurrent biliary colic and ultrasonographic evidence of gallstones.
Cholescintigraphy may show nonvisualization of the gallbladder but is less accurate.
Laboratory tests may show cholestasis, and a complete blood count or acute phase reactants (eg, C-reactive protein, erythrocyte sedimentation rate) may suggest inflammation, or infection when present.
Treatment of Chronic Cholecystitis
Sometimes laparoscopic cholecystectomy
Laparoscopic cholecystectomy is generally performed for persistent biliary symptoms due to chronic cholecystitis, although evidence of benefit of a surgical versus a conservative approach is mixed (1).
Chronic cholecystitis, in particular the calcified "porcelain" gallbladder, is associated with an increased risk of gallbladder carcinoma, but the use of cholecystectomy as a prophylactic procedure for this condition is controversial (2, 3).
Treatment references
1. Brazzelli M, Cruickshank M, Kilonzo M, et al. Clinical effectiveness and cost-effectiveness of cholecystectomy compared with observation/conservative management for preventing recurrent symptoms and complications in adults presenting with uncomplicated symptomatic gallstones or cholecystitis: a systematic review and economic evaluation. Health Technol Assess. 2014;18(55):1-vi. doi:10.3310/hta18550
2. Chen GL, Akmal Y, DiFronzo AL, et al. Porcelain Gallbladder: No Longer an Indication for Prophylactic Cholecystectomy. Am Surg. 2015;81(10):936-940.
3. DesJardins H, Duy L, Scheirey C, et al. Porcelain Gallbladder: Is Observation a Safe Option in Select Populations?. J Am Coll Surg. 2018;226(6):1064-1069. doi:10.1016/j.jamcollsurg.2017.11.026





