

Esophageal rupture may be iatrogenic during endoscopic procedures or other instrumentation or may be spontaneous (Boerhaave syndrome). Patients are seriously ill, with symptoms of mediastinitis. Diagnosis is by esophagography with a water-soluble contrast agent. Immediate surgical repair and drainage are required.
Endoscopic procedures are the primary cause of esophageal rupture, but spontaneous rupture may occur, typically related to vomiting, retching, or swallowing a large food bolus.
Spontaneous rupture is especially likely in patients who have untreated eosinophilic esophagitis together with acute food impaction.
The most common site of rupture is the distal esophagus on the left side. Acid and other stomach contents cause a fulminant mediastinitis and shock. Pneumomediastinum is common. Pleural effusion may also occur.
Symptoms and Signs of Esophageal Rupture
Symptoms of esophageal rupture include chest and abdominal pain, fever, vomiting, hematemesis, and shock.
Subcutaneous emphysema is palpable in some patients.
Mediastinal crunch (Hamman sign), a crackling sound synchronous with the heartbeat, may be present.
Diagnosis of Esophageal Rupture
CT esophagoscopy (water-soluble oral contrast CT)
Esophagography with water-soluble contrast
Sometimes endoscopy
Sometimes chest and abdominal radiographs
Sometimes blood tests

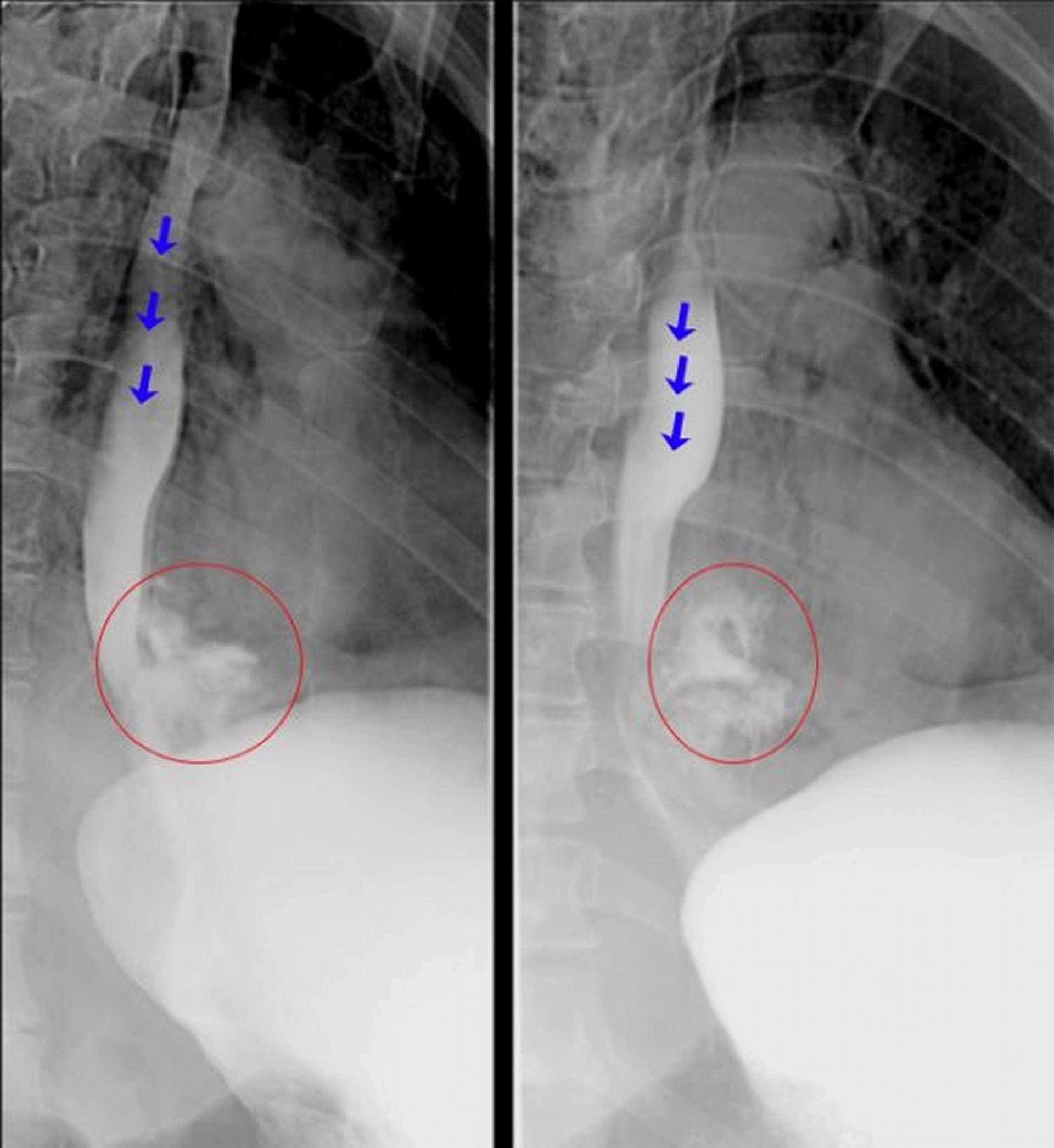
These fluoroscopic esophagograms show frank extravasation of contrast material from the distal esophagus consistent with an esophageal perforation. The blue arrows highlight contrast material within the lumen of esophagus. The red circles highlight contrast material that has extravasated out of the esophagus.
© Springer Science+Business Media
Chest and abdominal radiographs showing mediastinal air, pleural effusion, or mediastinal widening suggest the diagnosis.
CT esophagography (CT with water-soluble oral contrast) is the diagnostic test of choice due to sensitivity, speed, and safety relative to fluoroscopy (1, 2). Contrast esophagogram is an alternative. These contrast-based tests are performed using a water-soluble contrast agent, which avoids potential mediastinal irritation from barium. Endoscopy is sometimes used in equivocal cases, but it may miss a small perforation and carries the risk of enlarging the perforation.
Blood tests may include a blood count, to evaluate for blood loss (anemia) or sepsis; inflammatory markers; or markers of hepatic, renal, and other end-organ function when sepsis or septic shock is suspected.
Diagnosis references
1. Chirica M, Kelly MD, Siboni S, et al. Esophageal emergencies: WSES guidelines. World J Emerg Surg. 2019;14:26. doi:10.1186/s13017-019-0245-2
2. Salehpoor A, Thompson W. Imaging of esophageal perforation including in the postoperative patient: a contemporary review. Abdom Radiol (NY). Published online July 28, 2025. doi:10.1007/s00261-025-05142-0
Treatment of Esophageal Rupture
Endoscopic stenting or surgical repair
Sometimes nonoperative management
Pending surgical repair or endoscopic stent placement, patients should receive broad-spectrum antibiotics (eg, gentamicin plus metronidazole or piperacillin/tazobactam) and fluid resuscitation as needed for shock. Pending surgical repair or endoscopic stent placement, patients should receive broad-spectrum antibiotics (eg, gentamicin plus metronidazole or piperacillin/tazobactam) and fluid resuscitation as needed for shock.
Endoscopic repair techniques include stenting, clipping, and vacuum therapy (1, 2). These techniques are used for patients with iatrogenic perforations during endoscopy, in those in whom endoscopy was the diagnostic modality, or to repair esophageal leaks after surgical repair.
Surgery may be chosen as the initial repair technique for severe or complicated perforations, or when endoscopic techniques are unsuccessful (1, 2).
Nonoperative (conservative) management may be chosen for a subset of patients (early diagnosis, contained cervical or thoracic perforation, no esophageal disease, no sepsis, and availability of follow-up and intervention) (1).
Even with treatment, mortality is high (19 to 28%) (3, 4, 5).
Treatment references
1. Chirica M, Kelly MD, Siboni S, et al. Esophageal emergencies: WSES guidelines. World J Emerg Surg. 2019;14:26. doi:10.1186/s13017-019-0245-2
2. Lee JH, Kedia P, Stavropoulos SN, Carr-Locke D. AGA Clinical Practice Update on Endoscopic Management of Perforations in Gastrointestinal Tract: Expert Review. Clin Gastroenterol Hepatol. 2021;19(11):2252-2261.e2. doi:10.1016/j.cgh.2021.06.045
3. Edholm D, Andersson RE, Frankel A. Esophageal perforations - a population-based nationwide study in Sweden with survival analysis. Scand J Gastroenterol. 2022;57(9):1018-1023. doi:10.1080/00365521.2022.2060051
4. Owen RP, Chidambaram S, Griffiths EA, et al. Multicenter, Prospective Cohort Study of Oesophageal Injuries and Related Clinical Outcomes (MUSOIC study). Ann Surg. 2023;278(6):910-917. doi:10.1097/SLA.0000000000005889
5. Veziant J, Boudis F, Lenne X, et al. Outcomes Associated With Esophageal Perforation Management: Results From a French Nationwide Population-based Cohort Study. Ann Surg. 2023;278(5):709-716. doi:10.1097/SLA.0000000000006048
Drug Information for the Topic





