



Laryngitis is inflammation of the larynx, usually the result of a virus or vocal overuse. The result is acute change in the voice, with decreased volume and dysphonia. Diagnosis is based on clinical findings. Laryngoscopy is required for symptoms persisting > 2 weeks. Viral laryngitis is self-limited. Other infectious or irritating causes may require specific treatment.
Laryngitis may be acute (usually resolving within 1 week, sometimes up to 3 weeks) or chronic (>3 weeks) (1). The most common cause of acute laryngitis is viral upper respiratory infection. Bacterial or fungal infections are less common but can occur as a secondary infection following viral illness.
Coughing-induced laryngitis may also occur in bronchitis, pneumonia, influenza, pertussis, measles, and diphtheria. Excessive use of the voice (especially with loud speaking or singing), allergic reactions, gastroesophageal reflux, bulimia, or inhalation of irritating substances (eg, cigarette smoke or certain aerosolized medications) can cause acute or chronic laryngitis. More rarely, medications can induce potentially life-threatening laryngeal edema, such as angiotensin-converting enzyme (ACE) inhibitor–induced angioedema of the airway (2). Smoking and exposure to other heated fumes can cause Reinke edema, a watery swelling of the vocal folds.
References
1. Dworkin JP. Laryngitis: types, causes, and treatments. Otolaryngol Clin North Am. 2008;41(2):419-ix. doi:10.1016/j.otc.2007.11.011
2. Wilkerson RG, Winters ME. Angiotensin-Converting Enzyme Inhibitor-Induced Angioedema. Immunol Allergy Clin North Am. 2023;43(3):513-532. doi:10.1016/j.iac.2022.10.013
Symptoms and Signs of Laryngitis
The most prominent symptom of laryngitis is usually
A persistent change of voice
Volume may be decreased; some patients have aphonia (no sound production). Dysphonia, a sensation of tickling, rawness, and a constant urge to clear the throat may occur. Symptoms vary with the severity of the inflammation.
Dysphagia and throat pain may occur in more severe infections, along with systemic symptoms like fever and malaise. Laryngeal edema, although rare, may occur and cause stridor and dyspnea.

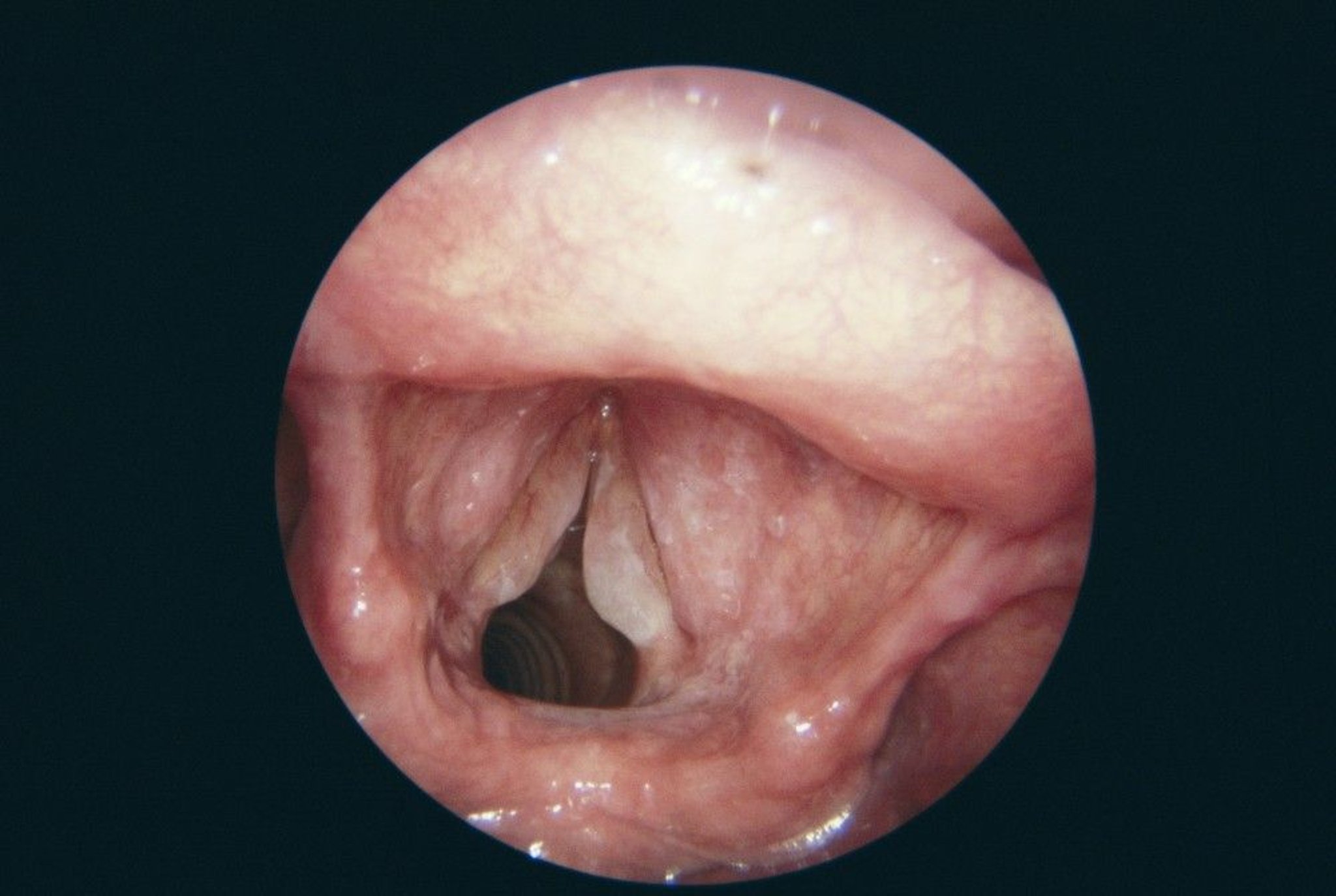
In this endoscopic view of the inflamed larynx of a patient suffering from laryngitis, the vocal folds (v-shaped, lower left) are swollen.
CNRI/SCIENCE PHOTO LIBRARY
Diagnosis of Laryngitis
Primarily history and physical examination
Sometimes indirect or direct flexible laryngoscopy
The diagnosis of laryngitis is usually based on the presenting symptoms.
Indirect or direct flexible laryngoscopy is recommended for symptoms persisting > 2 weeks (1); findings in laryngitis may include mild to marked erythema of the mucous membrane, which may also be edematous. With reflux, there is swelling of the inner lining of the larynx and redness of the arytenoids. With chronic irritation (eg, due to tobacco use), leukoplakia can develop. It is not recommended that clinicians routinely prescribe glucocorticoids to patients with dysphonia prior to visualization of the larynx.
A pseudomembrane may form in the pharynx or larynx as a sequela of infection; its presence should raise suspicion for diphtheria (2).

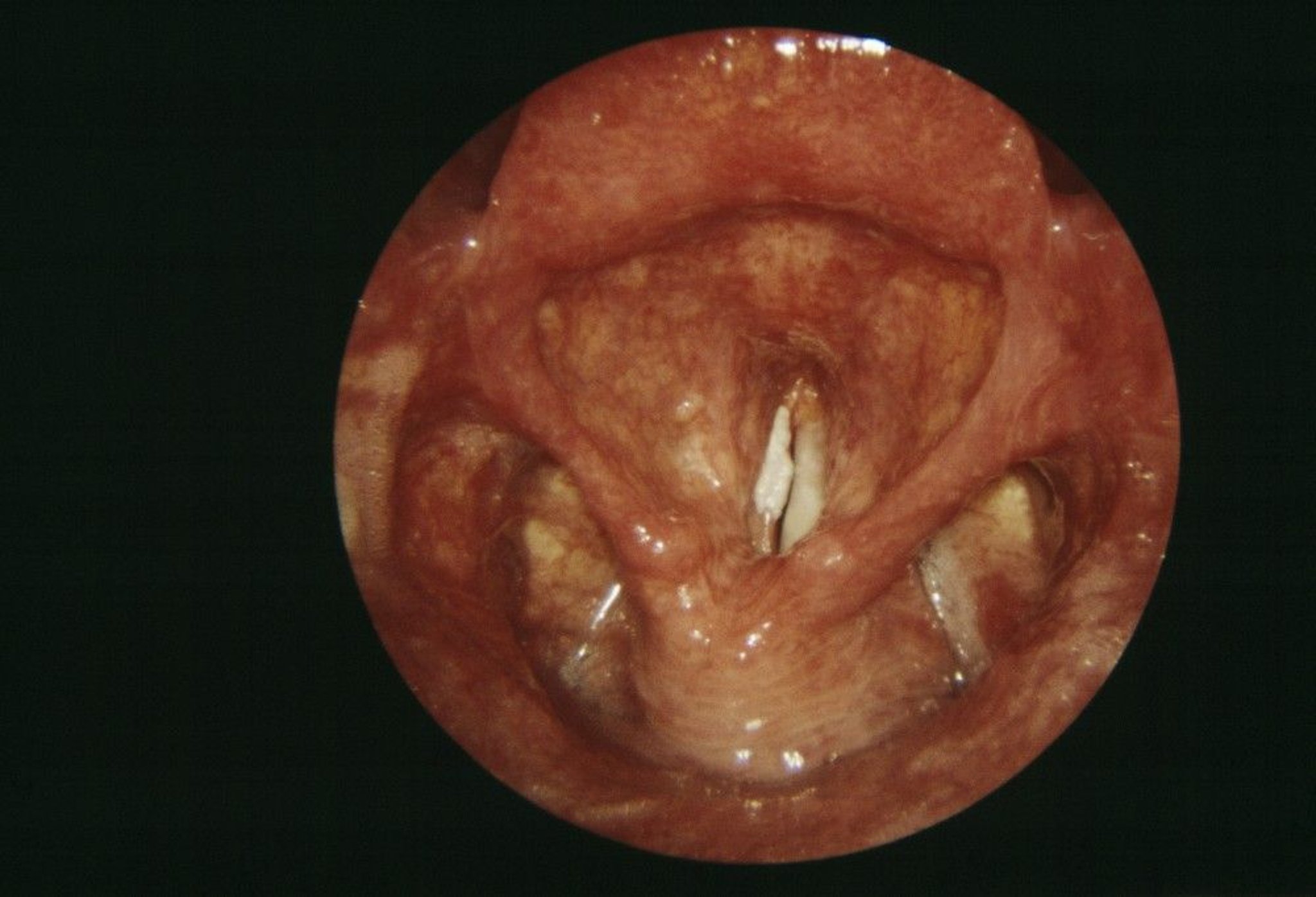
This endoscope view of the larynx of a patient shows leukoplakia (keratosis, white, center) of the vocal folds due to laryngitis. Leukoplakia is a thickening of the body tissues that develops in response to chronic irritation.
CNRI/SCIENCE PHOTO LIBRARY
Diagnosis references
1. Stachler RJ, Francis DO, Schwartz SR, et al. Clinical Practice Guideline: Hoarseness (Dysphonia) (Update) [published correction appears in Otolaryngol Head Neck Surg. 2018 Aug;159(2):403. doi: 10.1177/0194599818766900.]. Otolaryngol Head Neck Surg. 2018;158(1_suppl):S1-S42. doi:10.1177/0194599817751030
2. Dworkin JP. Laryngitis: types, causes, and treatments. Otolaryngol Clin North Am. 2008;41(2):419-ix. doi:10.1016/j.otc.2007.11.011
Treatment of Laryngitis
Symptomatic treatment (eg, cough suppressants, voice rest, hydration, steam inhalations)
Cough suppressants, voice rest, hydration, and steam inhalations relieve symptoms and promote resolution of acute laryngitis. Smoking cessation and treatment of acute or chronic bronchitis may relieve laryngitis.
Depending on the presumed cause, specific treatments to control gastroesophageal reflux or drug-induced laryngitis may be beneficial.
No specific treatment is available for viral laryngitis. Antibiotics or antifungals do not appear to be effective in improving objective clinical outcomes when administered for acute laryngitis, unless a bacterial or fungal etiology is suspected (1).
Treatment reference
1. Reveiz L, Cardona AF. Antibiotics for acute laryngitis in adults. Cochrane Database Syst Rev. 2015;2015(5):CD004783. Published 2015 May 23. doi:10.1002/14651858.CD004783.pub5





