



Pemphigus foliaceus is an autoimmune blistering disorder in which lack of adhesion in the superficial epidermis results in cutaneous erosions. Diagnosis is by skin biopsy and direct immunofluorescence. Treatment depends on disease severity and includes topical or systemic corticosteroids. Other immunosuppressive therapies may be needed.
Bullae are elevated, fluid-filled blisters ≥ 10 mm in diameter.
Pemphigus foliaceus usually occurs in middle-aged patients, affecting men and women in equal numbers. An endemic form of pemphigus foliaceus, fogo selvagem, occurs in younger adults and children, particularly in South America. Pemphigus foliaceus may occur after use of penicillamine, nifedipine, or captopril.
Pemphigus erythematosus, a form of pemphigus foliaceus localized to the cheeks, has immunologic features of pemphigus vulgaris and systemic lupus erythematosus (IgG and C3 deposition on keratinocyte surfaces and basement membrane zone with circulating antinuclear antibodies); however, patients rarely are diagnosed with both diseases concurrently.
Pemphigus foliaceus is mediated by IgG autoantibody against desmoglein 1 (Dsg1), a transmembrane glycoprotein cadherin important to cell–cell adhesion and signaling between keratinocytes (1; see figure Skin Cleavage Levels in Pemphigus and Bullous Pemphigoid).
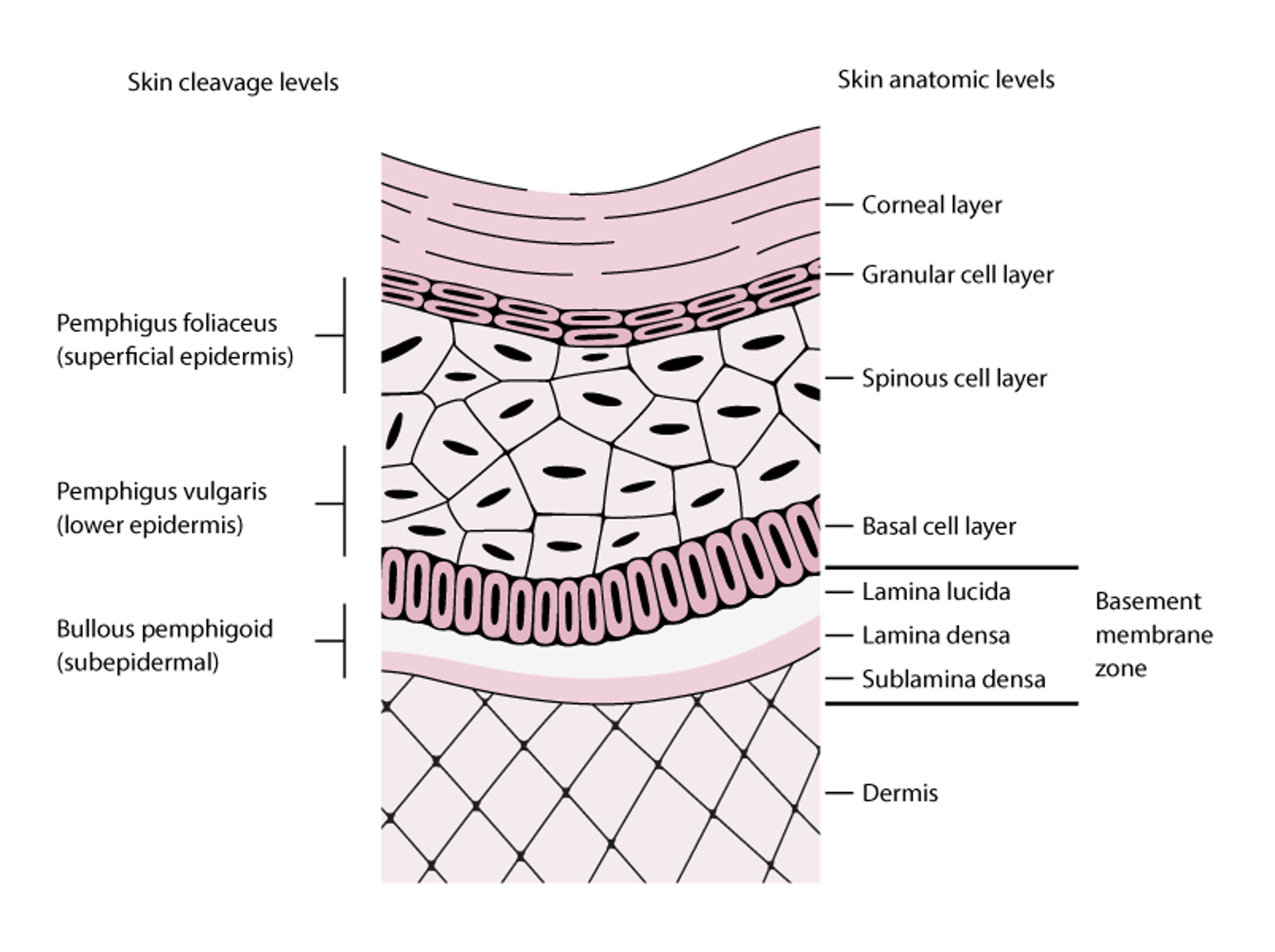
Skin Cleavage Levels in Pemphigus and Bullous Pemphigoid
Pemphigus foliaceus blisters form in the superficial layers of the epidermis. Pemphigus vulgaris blisters can form at any epidermal level but typically form in the lower aspects of the epidermis. Bullous pemphigoid blisters form subepidermally (lamina lucida of the basement membrane zone). In this figure, the basement membrane zone is disproportionately enlarged to display its layers. |

General reference
1. Russo I, De Siena FP, Saponeri A, et al: Evaluation of anti-desmoglein-1 and anti-desmoglein-3 autoantibody titers in pemphigus patients at the time of the initial diagnosis and after clinical remission. Medicine (Baltimore) 96(46):e8801, 2017. doi: 10.1097/MD.0000000000008801
Symptoms and Signs of Pemphigus Foliaceus
The primary lesion is a flaccid vesicle or bulla, but due to the superficial location of the epidermal split, lesions tend to rupture, so intact bullae or vesicles are rarely evident on examination. Instead, well-demarcated, scattered, crusted, erythematous lesions are common on the face, scalp, and upper trunk. Mucosal involvement is rare. Skin lesions can burn and cause pain, but patients are typically not severely ill. Pemphigus erythematosus tends to affect the malar cheeks.


This photo shows scaled, crusted, superficial lesions resulting from pemphigus foliaceus.


This photo shows well-demarcated, scattered, crusted, erythematous lesions of pemphigus foliaceus.
Diagnosis of Pemphigus Foliaceus
Skin biopsy and immunofluorescence
Diagnosis of pemphigus foliaceus is by biopsy of a lesion and adjacent (perilesional) unaffected skin that shows IgG autoantibodies against the keratinocyte cell surface via direct immunofluorescence. Autoantibodies to desmoglein 1 can be detected in serum via direct immunofluorescence, indirect immunofluorescence, and enzyme-linked immunosorbent assay (ELISA). Sensitivity of ELISA is > 95% (1).
Diagnosis reference
1. Joly P, Horvath B, Patsatsi Α, et al: Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol 34(9):1900-1913,2020. doi: 10.1111/jdv.16752
Treatment of Pemphigus Foliaceus
Corticosteroids, topical or systemic
If the disease is localized and not severe, high-potency topical corticosteroids are typically effective (1). More widespread or severe cases require systemic corticosteroids plus, at times, other immunosuppressive therapies, such as rituximab, plasma exchange, methotrexate, mycophenolate mofetil, or azathioprine. Topical calcineurin inhibitors have also been used.
Limited studies suggest that addition of a combination of tetracycline 500 mg orally 4 times a day or doxycycline 100 mg orally twice a day and nicotinamide 500 mg orally 3 times a day may be effective in some people.
Treatment reference
1. Joly P, Horvath B, Patsatsi Α, et al: Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol 34(9):1900-1913,2020. doi: 10.1111/jdv.16752
Key Points
Pemphigus foliaceus is an autoimmune disorder that causes flaccid bullous skin lesions.
Diagnose using skin biopsy and direct immunofluorescence.
Treat with topical or systemic corticosteroids.
Drug Information for the Topic





