



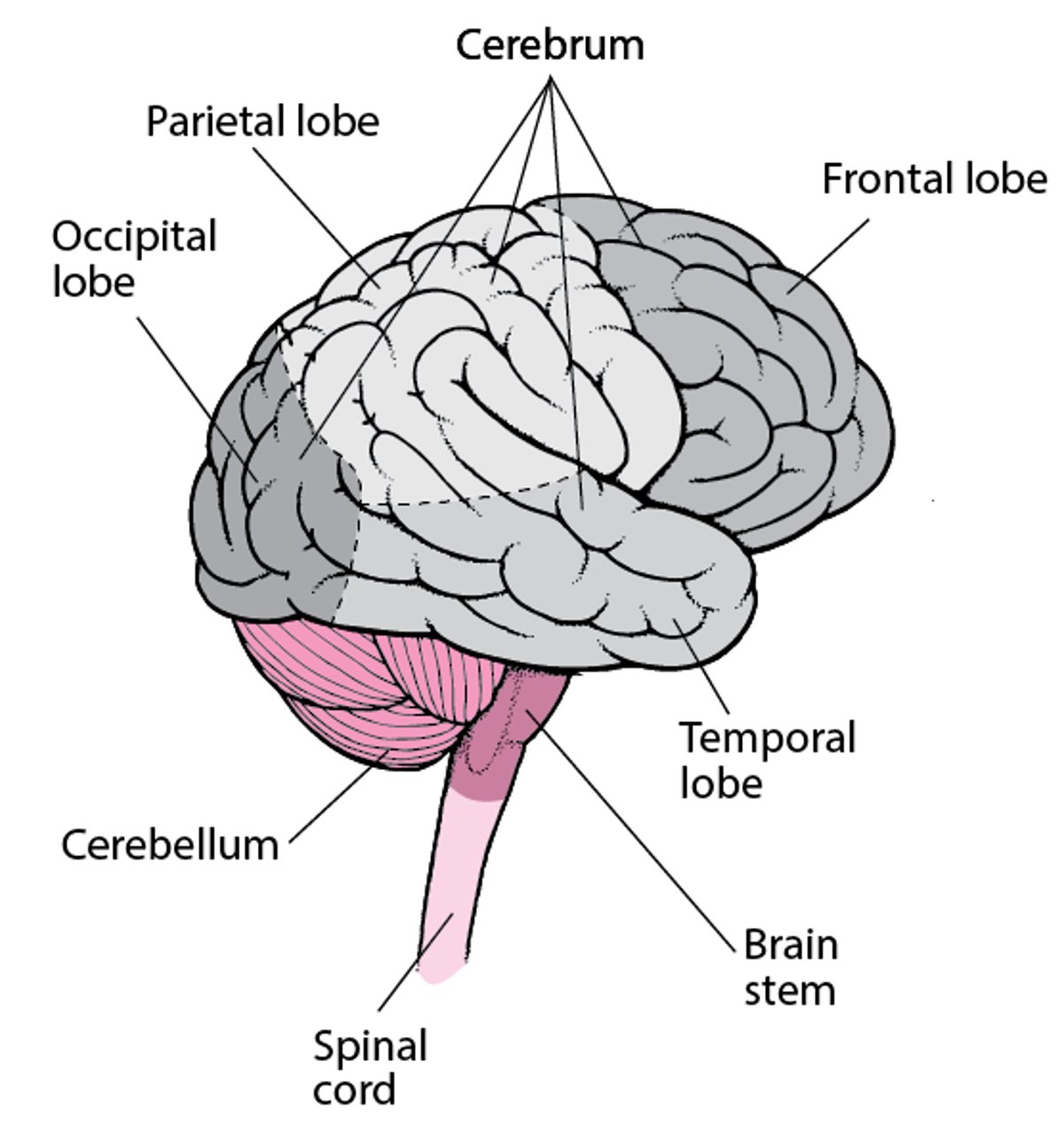
The cerebrum is divided by a longitudinal fissure into 2 hemispheres, each containing 6 discrete lobes:
The frontal, temporal, parietal, and occipital lobes cover the brain’s surface (see figure ); the insula is hidden under the Sylvian fissure. The limbic lobe (limbic system) is a C-shaped area on the most medial edge of each cerebral hemisphere; it includes some parts of the adjacent lobes.
Although specific functions are attributed to each lobe, most activities require coordination of multiple areas in both hemispheres. For example, although the occipital lobe is essential to visual processing, parts of the parietal, temporal, and frontal lobes on both sides also process complex visual stimuli.
Lobes of the Brain

Brain function is extensively lateralized. Visual, tactile, and motor activities of the left side of the body are directed predominantly by the right hemisphere and vice versa. Certain complex functions involve both hemispheres but are directed predominantly by one (cerebral dominance). For example, the left hemisphere is typically dominant for language, and the right is dominant for spatial attention.
The cerebral cortex (see figure ) contains
The primary sensory areas
The primary motor cortex
Multiple association areas, including unimodal and heteromodal association areas
Areas of the Brain


The primary sensory areas receive somesthetic, auditory, visual, and gustatory stimuli from the thalamus, which receives stimuli from specialized sensory organs and peripheral receptors. Olfactory pathways bypass the thalamus and go directly to specialized areas of the cortex. Sensory stimuli are further processed in association areas that relate to 1 or more senses.
The primary motor cortex generates volitional body movements; motor association areas help plan and execute complex motor activity.
Each unimodal association area is adjacent to its corresponding primary sensory area and processes information from that area at a higher level than the primary sensory area.
Heteromodal association areas are not restricted to any single motor or sensory function but receive convergent information from multiple sensory and motor areas of the brain. Heteromodal association areas in the frontal, temporal, and parietal lobes integrate sensory data, motor feedback, and other information with instinctual and acquired memories. This integration facilitates learning and creates thought, expression, and behavior.
Frontal lobes
The frontal lobes are anterior to the central sulcus. They are essential for planning and executing learned and purposeful behaviors; they are also the site of many inhibitory functions. There are several functionally distinct areas in the frontal lobes:
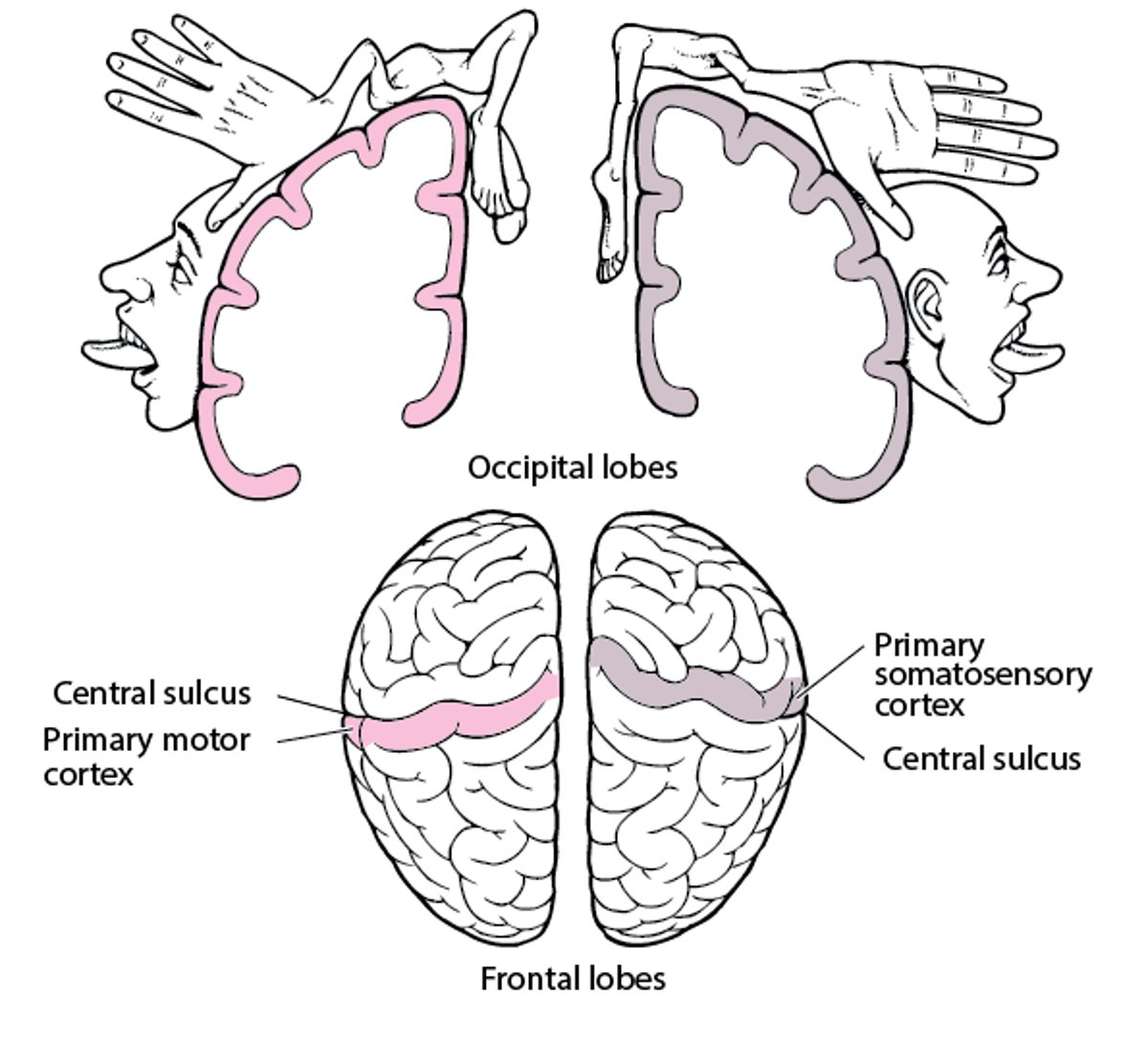
The primary motor cortex is the most posterior part of the precentral gyrus. The primary motor cortex on one side controls all moving parts on the contralateral side of the body (shown on a spatial map called a homunculus—see figure ); 90% of motor fibers from each hemisphere cross the midline in the lower brain stem and upper cervical spinal cord. Thus, damage to the motor cortex of one hemisphere causes weakness or paralysis mainly on the contralateral side of the body.
The medial frontal cortex (sometimes called the medial prefrontal area) is important in arousal and motivation. If lesions in this area are large and extend to the most anterior part of the cortex (frontal pole), patients sometimes become abulic (apathetic, inattentive, and markedly slow to respond).
The orbital frontal cortex (sometimes called the orbital prefrontal area—see figure ) helps modulate social behaviors. Patients with orbital frontal lesions can become emotionally labile, indifferent to the implications of their actions, or both. They may be alternately euphoric, facetious, vulgar, and indifferent to social nuances. Bilateral acute trauma to this area may make patients boisterously talkative, restless, and socially intrusive. The disinhibition and abnormal behaviors that can occur with aging and in many types of dementia probably result from degeneration of the frontal lobe, particularly the orbital frontal cortex.
The left posteroinferior frontal cortex (sometimes called the Broca area or posteroinferior prefrontal area—see figure ) controls expressive language function. Lesions in this area cause expressive aphasia (impaired expression of words).
The dorsolateral frontal cortex (sometimes called the dorsolateral prefrontal area) manipulates very recently acquired information—a function called working memory. Lesions in this area can impair the ability to retain information and process it in real time (eg, to spell words backwards or to alternate between letters and numbers sequentially).
Homunculus
Specific parts of the cortex control specific motor and sensory functions on the contralateral side of the body. The amount of cortical space given to a body part varies; eg, the area of the cortex that controls the hand is larger than the area that controls the shoulder. The map of these parts is called the homunculus (“little person”). |

Parietal lobes
Several areas in the parietal lobes have specific functions.
The primary somatosensory cortex, located in the postrolandic area (postcentral gyrus) in the anterior parietal lobes, integrates somesthetic stimuli for recognition and recall of form, texture, and weight. The primary somatosensory cortex on one side receives all somatosensory input from the contralateral side of the body (see figure ). Lesions in the anterior parietal lobe can cause difficulty recognizing objects by touch (astereognosis).
Areas posterolateral to the postcentral gyrus generate visual-spatial relationships and integrate these perceptions with other sensations to create awareness of trajectories of moving objects. These areas also mediate proprioception (awareness of the position of body parts in space).
Parts of the midparietal lobe of the dominant hemisphere are involved in abilities such as calculation, writing, left-right orientation, and finger recognition. Lesions in the angular gyrus can cause deficits in writing, calculating, left-right disorientation, and finger-naming (Gerstmann syndrome).
The nondominant parietal lobe integrates the contralateral side of the body with its environment, enabling people to be aware of this environmental space, and is important for abilities such as drawing. Acute injury to the nondominant parietal lobe may cause neglect of the contralateral side (usually the left), resulting in decreased awareness of that part of the body, its environment, and any associated injury to that side (anosognosia). For example, patients with large right parietal lesions may deny the existence of left-sided paralysis. Patients with smaller lesions may lose the ability to do learned motor tasks (eg, dressing, other well-learned activities)—a spatial-manual deficit called apraxia.
Temporal lobes
The temporal lobes are integral to auditory perception, receptive components of language, visual memory, declarative (factual) memory, and emotion. Patients with right temporal lobe lesions commonly lose the ability to interpret nonverbal auditory stimuli (eg, music). Left temporal lobe lesions interfere greatly with the recognition, memory, and formation of language.
Occipital lobes
The occipital lobes contain
The primary visual cortex
Visual association areas
Lesions in the primary visual cortex lead to a form of cortical blindness; in 1 form, called Anton syndrome, patients become unable to recognize objects by sight and are generally unaware of their deficits, often confabulating descriptions of what they see.
Seizures involving the occipital lobe can cause visual hallucinations, often consisting of lines or meshes of color superimposed on the contralateral visual field.
Insula
The insula integrates sensory and autonomic information from the viscera. It plays a role in certain language functions, as evidenced by aphasia in patients with some insular lesions. The insula processes aspects of pain and temperature sensation and possibly taste.
Limbic lobe
The limbic lobe (limbic system) includes structures that receive inputs from diverse areas of the brain and that participate in complicated, interrelated behaviors (eg, memory, learning, emotion). Lesions that affect the limbic system usually result in a variety of deficits.
Patients with epileptogenic foci in the medial limbic-emotional parts of the temporal lobe commonly have complex partial seizures, characterized by uncontrollable feelings and autonomic, cognitive, or emotional dysfunction. Occasionally, such patients have personality changes, characterized by humorlessness, philosophic religiosity, and obsessiveness. Patients may have olfactory hallucinations and hypergraphia (an overwhelming urge to write).
Pathophysiology of Cerebral Dysfunction
Cerebral dysfunction may be focal or global. Focal and global processes can manifest as deficits or become foci for seizure activity. These processes may also affect subcortical systems, altering arousal (eg, causing stupor or coma) or integration of thought (eg, causing delirium).
Focal dysfunction usually results from
Structural abnormalities (eg, tumors, abscesses, stroke, trauma, malformations, gliosis, demyelination)
Manifestations depend on the lesion’s location, size, and development rate. Small lesions (<2 cm) or lesions that develop very slowly may be asymptomatic. Larger lesions, rapidly developing lesions (over weeks or months rather than years), and lesions that simultaneously affect both hemispheres are more likely to become symptomatic. Focal lesions in white matter can interrupt the connectivity between brain areas and cause the disconnection syndrome (inability to do a task that requires coordinated activity of ≥ 2 brain regions, despite retention of basic functions of each region).
Global dysfunction is caused by
Toxic-metabolic disorders, including hypoxia and ischemia (commonly)
Diffuse inflammation
Vasculopathy
Major trauma
Disseminated cancer
Degenerative disorders
Global dysfunction may also result from disorders that occur in a specific area of the brain (eg, abscesses, tumors, trauma) if they increase intracranial pressure or cause herniation.
These disorders affect multiple dimensions of cerebral function.
Recovery
Recovery from brain injury depends in part on the following characteristics of the brain:
Plasticity of the remaining cerebrum
Redundancy
Plasticity (ability of an area of the brain to alter its function) of the cerebrum varies from person to person and is affected by age and general health. Plasticity is most prominent in the developing brain. For example, if the dominant hemisphere language areas are severely damaged before age 8 years, the opposite hemisphere can often assume near-normal language function. Although capacity for recovery from brain injury is considerable after the first decade of life, severe damage more often results in permanent deficits. Gross reorganization of brain function after injury in adults is uncommon, although plasticity remains operative in certain specific areas of the brain throughout life.
Redundancy refers to the ability of more than 1 area of the brain to perform the same function.
Cerebral dysfunction syndromes
Specific syndromes include
Amnesia (including transient global amnesia)
Psychiatric conditions (eg, depression, psychosis, anxiety disorders) sometimes include similar elements. Dysarthria, a neuromotor disorder, may cause symptoms similar to those of aphasia.
Diagnosis of Cerebral Dysfunction
History and physical examination
Often neuropsychological testing
Blood and CSF laboratory analysis
Imaging (eg, CT or MRI)
In general, diagnosis of cerebral dysfunction is clinical, often assisted by neuropsychological testing. This standardized testing provides information about the brain’s structural and functional integrity. It evaluates intelligence, executive function (eg, planning, abstraction, conceptualization), attention, memory, language, perception, sensorimotor functions, motivation, mood and emotion, quality of life, and personality.
Diagnosis of the cause usually requires laboratory tests (blood and sometimes analysis of cerebrospinal fluid) and brain imaging, either structural (CT, MRI) or functional (positron emission tomography [PET], single-photon emission computed tomography [SPECT], functional MRI [fMRI]).





