

Tuberous sclerosis complex is a genetic disorder in which tumors (usually hamartomas) develop in multiple organs. Diagnosis requires specific clinical criteria and imaging of the affected organ. Treatment is generally symptomatic, and mTOR inhibitors (sirolimus or everolimus) are added for certain disease manifestations. Patients must be monitored regularly to evaluate for complications.Tuberous sclerosis complex is a genetic disorder in which tumors (usually hamartomas) develop in multiple organs. Diagnosis requires specific clinical criteria and imaging of the affected organ. Treatment is generally symptomatic, and mTOR inhibitors (sirolimus or everolimus) are added for certain disease manifestations. Patients must be monitored regularly to evaluate for complications.
Tuberous sclerosis complex (TSC) is a neurocutaneous syndrome that is estimated to occur in 1 of 6,000 to 10,000 live births (1). Approximately 85% of cases involve mutations in the TSC1 gene (9q34), which controls the production of hamartin, or in the TSC2 gene (16p13.3), which controls the production of tuberin. In one-third of all cases, TSC is inherited in an autosomal dominant manner (ie, if either parent has the disorder, children have a 50% risk of having it) (2). However, de novo mutations account for two-thirds of cases.
Tuberin and hamartin form a complex that is known to inhibit the mammalian target of rapamycin (mTOR) pathway, which is a central regulator of cell growth and proliferation (3). Loss of function in either the TSC1 or TSC2 gene leads to constitutive mTOR activation, resulting in abnormal cellular growth, differentiation, and migration as well as defects in protein and lipid synthesis (4). Ultimately, this cascade of events results in the formation of benign tumors (hamartomas) in multiple organs at different ages (5):
Brain
Heart
Eyes
Kidneys
Lungs
Skin
Central nervous system (CNS) tubers interrupt neural circuits, causing developmental delay and cognitive impairment and may cause seizures, including infantile spasms. Sometimes the tubers grow and obstruct the flow of cerebrospinal fluid from the lateral ventricles, causing unilateral hydrocephalus. Sometimes tubers undergo malignant transformation into gliomas, particularly subependymal giant cell astrocytomas (SEGAs).
Cardiac rhabdomyomas may develop prenatally, sometimes causing heart failure in neonates. These rhabdomyomas usually disappear over time and usually do not cause symptoms later in childhood or in adulthood.
Kidney tumors (angiolipomas) may develop in adults, and polycystic kidney disease may develop at any age. Kidney disease may cause hypertension.
Pulmonary lesions, such as lymphangioleiomyomatoses, may develop, particularly in adolescent girls.
General references
1. Northrup H, Aronow ME, Bebin EM, et al. Updated International Tuberous Sclerosis Complex Diagnostic Criteria and Surveillance and Management Recommendations. Pediatr Neurol. 2021;123:50-66. doi:10.1016/j.pediatrneurol.2021.07.011
2. Northrup H, Koenig MK, Pearson DA, Au KS. Tuberous Sclerosis Complex. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, eds. GeneReviews®. Seattle (WA): University of Washington, Seattle; July 13, 1999.
3. Salussolia CL, Klonowska K, Kwiatkowski DJ, Sahin M. Genetic Etiologies, Diagnosis, and Treatment of Tuberous Sclerosis Complex. Annu Rev Genomics Hum Genet. 2019;20:217-240. doi:10.1146/annurev-genom-083118-015354
4. Henske EP, Jóźwiak S, Kingswood JC, Sampson JR, Thiele EA. Tuberous sclerosis complex. Nat Rev Dis Primers. 2016;2:16035. Published 2016 May 26. doi:10.1038/nrdp.2016.35
5. Curatolo P, Specchio N, Aronica E. Advances in the genetics and neuropathology of tuberous sclerosis complex: edging closer to targeted therapy. Lancet Neurol. 2022;21(9):843-856. doi:10.1016/S1474-4422(22)00213-7
Symptoms and Signs of TSC
Manifestations vary greatly in severity. Skin lesions are typically present.
Infants with CNS lesions may present with a type of seizure called infantile spasms. Affected children may also have other types of seizures, intellectual disability, autism spectrum disorder, learning disorders, or behavioral problems.
Retinal achromic patches as well as retinal hamartomas are common.
Pitting of the enamel in permanent teeth is common.
Skin findings include:
Initially pale, ash leaf–shaped macules: Present in > 90% of patients and develop during infancy or early childhood (1)
"Confetti" skin lesions: Areas of skin containing many minute hypopigmented macules, are less common than ash-leaf macules
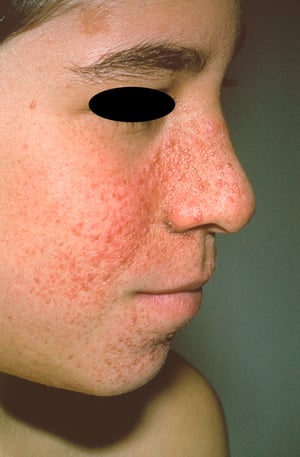
Angiofibromas of the face (adenoma sebaceum): Develop during later childhood
Fibrous cephalic plaques on the scalp, head, face, and neck: In approximately 30% of patients (2)
Congenital shagreen patches (raised lesions with a texture resembling an orange peel, usually on the back)
Subcutaneous nodules
Café-au-lait spots
Subungual and periungual fibromas (Koenen tumors): Can develop any time during childhood or early adulthood


Ash-leaf macules are depigmented areas that are very common among patients with tuberous sclerosis complex. The areas are 1 to 3 cm in length and may be more easily seen under ultraviolet light (Wood light).
Ash-leaf macules are depigmented areas that are very common among patients with tuberous sclerosis complex. The areas a
By permission of the publisher. From Puduvalli V: Atlas of Cancer. Edited by M Markman and R Gilbert. Philadelphia, Current Medicine, 2002.


This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
DR M.A. ANSARY/SCIENCE PHOTO LIBRARY

This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
Photo courtesy of Karen McKoy, MD.


Koenen tumors are periungual and subungual fibromas (reddish to flesh-colored papules emerging from nail folds) in patients with tuberous sclerosis complex.
Koenen tumors are periungual and subungual fibromas (reddish to flesh-colored papules emerging from nail folds) in pati
© Springer Science+Business Media
Ash-leaf macules are depigmented areas that are very common among patients with tuberous sclerosis complex. The areas are 1 to 3 cm in length and may be more easily seen under ultraviolet light (Wood light).
Ash-leaf macules are depigmented areas that are very common among patients with tuberous sclerosis complex. The areas a
By permission of the publisher. From Puduvalli V: Atlas of Cancer. Edited by M Markman and R Gilbert. Philadelphia, Current Medicine, 2002.
This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
DR M.A. ANSARY/SCIENCE PHOTO LIBRARY
This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
This photo shows angiofibromas (adenoma sebaceum) on the face of a patient with tuberous sclerosis complex.
Photo courtesy of Karen McKoy, MD.
Koenen tumors are periungual and subungual fibromas (reddish to flesh-colored papules emerging from nail folds) in patients with tuberous sclerosis complex.
Koenen tumors are periungual and subungual fibromas (reddish to flesh-colored papules emerging from nail folds) in pati
© Springer Science+Business Media
Symptoms and signs reference
1. Northrup H, Koenig MK, Pearson DA, Au KS. Tuberous Sclerosis Complex. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, eds. GeneReviews®. Seattle (WA): University of Washington, Seattle; July 13, 1999.
2. Kirk CW, Donnelly DE, Hardy R, Shepherd CW, Morrison PJ. Natural history of a fibrous cephalic plaque and sustained eight decade follow-up in an 80 year old with tuberous sclerosis complex type 2. Ulster Med J. 2020;89(1):14-16.
Diagnosis of TSC
Clinical criteria
Identification of the skin lesions
Imaging of affected organs
Molecular genetic testing
The International Tuberous Sclerosis Complex Consensus Group has defined major and minor criteria for making a definite or possible diagnosis of TSC (1) (see table ).
A definite diagnosis of TSC by these criteria requires either of the following:
The identification of either a TSC1 or TSC2 pathogenic (or likely pathogenic) variant by molecular genetic testing
Two major features or 1 major feature with 2 minor features
A possible diagnosis of TSC by these criteria requires the following:
Either 1 major feature or ≥ 2 minor features
International Tuberous Sclerosis Complex (TSC) Diagnostic Criteria
Criterion | Comments |
|---|---|
Major features* | |
Hypomelanotic macules (ash-leaf macules or "confetti" lesions) | ≥ 3, at least 5 mm in diameter |
Angiofibromas (adenoma sebaceum) or fibrous cephalic plaque | ≥ 3 angiofibromas or ≥ 1 fibrous cephalic plaque |
Subungual/periungual fibromas | ≥ 2 |
Shagreen patch | — |
Multiple retinal hamartomas | — |
Multiple cortical tubers and/or radial migration lines | — |
Subependymal nodules | ≥ 2 |
— | |
Cardiac rhabdomyoma | — |
— | |
Angiomyolipomas† | ≥ 2 |
Minor features* | |
“Confetti” skin lesions | Areas of stippled hypopigmentation, typically on the extremities |
Pitting of dental enamel | ≥ 3 |
Intraoral fibromas | ≥ 2 |
Retinal achromic patch | — |
Multiple renal cysts | — |
Nonrenal hamartomas | — |
Sclerotic bone lesions | — |
* A definite diagnosis of TSC requires either of the following:
A possible diagnosis of TSC requires the following:
| |
† A combination of the 2 major clinical features lymphangioleiomyomatosis and angiomyolipomas without other features does not meet the criteria for a definite diagnosis. | |
Data from Northrup H, Aronow ME, Bebin EM, et al: Updated international tuberous sclerosis complex diagnostic criteria and surveillance and management recommendations. Pediatr Neurol 123:50-66, 2021. doi: 10.1016/j.pediatrneurol.2021.07.011 2013 | |
Physical examination is performed to check for typical skin lesions. Retinal examination via funduscopy should be done to check for retinal achromic patches and hamartomas.
TSC may be suspected when a fetal ultrasound detects cardiac rhabdomyomas or when infantile spasms occur.
Cardiac or cranial manifestations may be visible on routine prenatal ultrasound. MRI or ultrasound of the affected organs is necessary for confirmation. Baseline EEG (awake and asleep) is needed to exclude infantile spasms and may show interictal hypsarrhythmia.
Specific genetic testing (ie, sequence analysis, gene-targeted deletion/duplication analysis of TSC1 and TSC2) is available (2).
Diagnosis references
1. Northrup H, Aronow ME, Bebin EM, et al. Updated international tuberous sclerosis complex diagnostic criteria and surveillance and management recommendations. Pediatr Neurol. 2021;123:50-66. doi:10.1016/j.pediatrneurol.2021.07.011
2. Northrup H, Koenig MK, Pearson DA, Au KS. Tuberous Sclerosis Complex. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, eds. GeneReviews®. Seattle (WA): University of Washington, Seattle; July 13, 1999.
Treatment of TSC
Symptomatic treatment
Sirolimus or everolimus for certain disease features
The treatment of TSC is both symptomatic and specific:
For seizures: Antiseizure medications (especially vigabatrin for For seizures: Antiseizure medications (especially vigabatrin forinfantile spasms) or sometimes epilepsy surgery
For skin lesions: Dermabrasion or laser techniques, topical sirolimusFor skin lesions: Dermabrasion or laser techniques, topical sirolimus
For neurobehavioral problems: Behavior management techniques or medications
For hypertension caused by renal problems: Antihypertensives or surgery to remove growing tumors
For developmental delays: Special schooling or occupational therapy
For CNS tubers, refractory seizures, and renal angiomyolipomas: mTOR inhibitors (everolimus or sirolimus)For CNS tubers, refractory seizures, and renal angiomyolipomas: mTOR inhibitors (everolimus or sirolimus)
mTOR inhibitors such as oral sirolimus and its derivative, everolimus, may be used to prevent and treat subependymal giant cell astrocytomas (SEGAs) and other manifestations of TSC such as TSC-associated partial-onset seizures, TSC-associated facial angiofibromas, renal angiomyolipomas, and pulmonary lymphangioleiomyomatosis (1). Topical sirolimus may be helpful for facial angiofibromas (2). Studies using these medications for these and other complications of TSC are ongoing. The main adverse effect of these medications is stomatitis (3).
Genetic counseling is indicated for adolescents and adults of childbearing age.
Screening for complications
All patients should be screened regularly to detect complications of TSC early. Typically, the following is done:
MRI of the head to check for intracranial complications (eg, SEGAs) at least every 3 years
Renal ultrasound or MRI of the abdomen to check for kidney tumors every 3 years in school-aged children and every 1 to 2 years for life in affected adults
In women ≥ 18 years, screening for exertional dyspnea and shortness of breath annually and high-resolution CT every 5 to 10 years to screen for lymphangioleiomyomatosis
Neuropsychologic testing periodically and behavioral screening in children to help plan for support at school and behavioral interventions
Echocardiogram at least every 3 years for asymptomatic children and adolescents with cardiac rhabdomyomas (monitoring must be continued until cardiac rhabdomyomas have regressed)
Clinical monitoring is also important and sometimes prompts more frequent testing. The development of headaches, loss of skills, or new types of seizures that may be caused by malignant transformation or growth of CNS tubers is considered an indication for neuroimaging.
Treatment references
1. Sasongko TH, Kademane K, Chai Soon Hou S, Jocelyn TXY, Zabidi-Hussin Z. Rapamycin and rapalogs for tuberous sclerosis complex. Cochrane Database Syst Rev. 2023;7(7):CD011272. Published 2023 Jul 11. doi:10.1002/14651858.CD011272.pub3
2. Darling T. Topical sirolimus to treat tuberous sclerosis complex (TSC). JAMA Dermatol. 2018;154(7):761–762. doi:10.1001/jamadermatol.2018.0465
3. Liu M, Ye J, You X. An updated meta-analysis of effectiveness and safety of mTOR inhibitors in the management of tuberous sclerosis complex patients. Childs Nerv Syst. 2024;40(3):823-829. doi:10.1007/s00381-023-06200-y
Prognosis for TSC
The prognosis for TSC depends on symptom severity. Infants with mild symptoms generally do well and live long, productive lives; infants with severe symptoms often have severe disabilities.
Regardless of severity, most children show continued developmental progress.
Key Points
Tuberous sclerosis complex is a genetic disorder in which tumors (usually hamartomas) develop in multiple organs at different ages.
Manifestations vary greatly; skin lesions are typically present (eg, café-au-lait spots, shagreen patches, ash-leaf macules).
Diagnose using clinical criteria, identification of characteristic skin lesions, imaging of affected organs, and molecular genetic testing.
Treat symptomatically and specifically for the multiple complications.
Consider everolimus or sirolimus for seizures, malignant tumors, and some of the benign tumors. Consider everolimus or sirolimus for seizures, malignant tumors, and some of the benign tumors.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.





