

Subacromial bursal injection is the process of injecting anesthetics and/or glucocorticoids in or around the subacromial bursa to help treat bursitis.
A lateral approach (described below) is commonly used and not difficult to perform at the bedside.
Subacromial bursitis, supraspinatus tendonitis, and calcific tendonitis may be indistinguishable in their clinical manifestations and response to injection therapy.
The subacromial bursa lies between bone and overlying tendons. Because it is deep, subacromial bursitis seldom causes visible swelling or erythema. However, bedside ultrasound for subacromial evaluation and needle guidance is usually unnecessary. Aspiration of fluid is not anticipated unless swelling is evident on examination or by ultrasound. A palpable effusion raises concern for infection.
(See also Bursitis.)
Indications for Injecting a Subacromial Bursa
For injections of glucocorticoid to treat inflammation
Symptoms of nonseptic bursitis are often effectively treated with rest and 10 to 14 days of nonsteroidal anti-inflammatory drugs (if not contraindicated). However, when needed, bursal injection therapy provides rapid relief, which may be beneficial for subacromial bursitis that persists or recurs despite conservative measures.
Contraindications to Injecting a Subacromial Bursa
Absolute contraindications
Overlying cellulitis or skin ulcer, bacteremia, adjacent prosthetic shoulder joint
Hypersensitivity to an injected substance
For glucocorticoid injection, possible septic bursitis
Relative contraindications
Unrecognized tendon injury: Analgesia provided by a glucocorticoid with anesthetic injection could delay accurate diagnosis and permit further damage.
Poorly controlled diabetes: Benefit of glucocorticoids is weighed against risk of short-term worsening glycemic control.
Unresponsiveness to prior glucocorticoid injections into same site (although this recommendation has not been systematically studied).
Coagulopathy is not a contraindication (1).
Complications of Injecting a Subacromial Bursa
Complications are uncommon and include:
Subcutaneous fat atrophy, skin atrophy and sinus tracts, and temporary skin depigmentation due to inadvertent subcutaneous glucocorticoid injection
Painful local reaction thought to result from a chemical synovitis in response to the crystals in the glucocorticoid solution (sometimes called a postinjection flare) occurring within a few hours of depot glucocorticoid injection and usually lasting ≤ 48 hours
Infection
In diabetic patients, hyperglycemia after a depot glucocorticoid injection
Tendon, nerve, or blood vessel damage from misdirected glucocorticoid injection due to errant needle insertion
Equipment for Injecting a Subacromial Bursa
Antiseptic solution (eg, chlorhexidine, povidone iodine, isopropyl alcohol)Antiseptic solution (eg, chlorhexidine, povidone iodine, isopropyl alcohol)
Sterile gauze and adhesive bandage
Gloves
Needle insertion site anesthesia: topical freezing spray (eg, ethyl chloride) and/or injectable 1% lidocaine without epinephrine, in a 3-mL syringeNeedle insertion site anesthesia: topical freezing spray (eg, ethyl chloride) and/or injectable 1% lidocaine without epinephrine, in a 3-mL syringe
Optional: For therapeutic injection, 1% lidocaine (without epinephrine) mixed with injectable depot glucocorticoid (eg, triamcinolone acetonide, 20 to 40 mg)Optional: For therapeutic injection, 1% lidocaine (without epinephrine) mixed with injectable depot glucocorticoid (eg, triamcinolone acetonide, 20 to 40 mg)
Hemostat, if switching of syringe while the needle remains inserted is anticipated
27-gauge (or as large as 22 gauge), 1.5-inch needle (for injection, not aspiration)
Some 3-, 5-, and 10-mL syringes
Having an assistant is helpful.
Additional Considerations for Injecting a Subacromial Bursa
For bursal injection, local anesthetic and depot glucocorticoid often are mixed in a single syringe. Adding the anesthetic helps confirm good needle placement when injection immediately relieves pain. Adding anesthetic also may decrease the risk of the glucocorticoid causing postinjection flare.
If the history or physical examination suggests possible septic bursitis (eg, marked regional warmth, erythema, distention), withhold glucocorticoid injection and consider ultrasound-guided aspiration.
Immediate analgesia after injection of local anesthetic helps confirm correct needle placement and that the subacromial bursa (or related periarthritis) is the source of pain.
Subacromial bursitis and supraspinatus tendinopathy cannot always be differentiated clinically, and the tendinopathy may be calcific, sometimes with spread to the bursa (calcific, or calcareous tendinitis).
Injection therapy can be effective for any of these disorders; however, the injection path may differ for tendinopathy.
Consider performing a shoulder radiograph before injection in patients with longstanding chronic shoulder pain or if symptoms persist to identify other possible causes of pain (eg, glenohumeral osteoarthritis, fracture).
Relevant Anatomy for Injecting a Subacromial Bursa
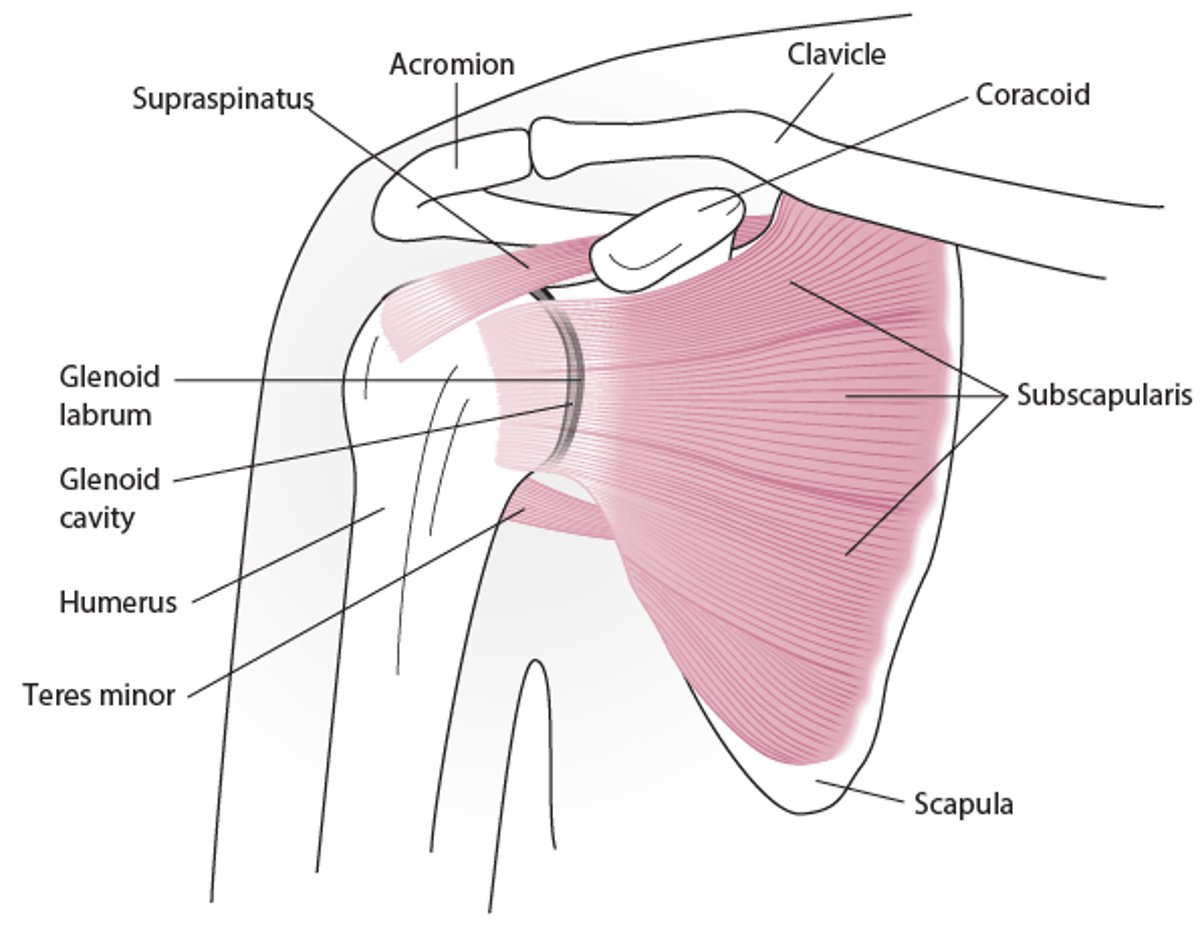
The subacromial bursa lies immediately superior and lateral to the supraspinatus tendon and inferior to the coracoacromial arch.
Injection into a tendon or muscle will meet resistance and is to be avoided; injection into a bursa (or sometimes into a tendon sheath) is desired and will not meet resistance.
Shoulder Anatomy (Anterior View)

Positioning for Injecting a Subacromial Bursa
Seat the patient with the forearm resting in the lap. The seated position allows gravity to distract the humerus and widen the subacromial space.
To avoid vasovagal episodes, avert the patient's head and orient your work area so that the patient does not see the needles.
Step-by-Step Description of Injecting a Subacromial Bursa
Prepare the site
Mark the needle entry site on the skin.
Prepare the area with antiseptic solution.
Spray freezing spray at the needle insertion site until it just blanches or inject a skin wheal of local anesthetic (≤ 1 mL).
Inject the bursa
Wear gloves (standard precautions).
Lateral needle insertion approach: Insert the needle below the lateral acromion border and above the humeral head.
Posterior needle insertion approach: Insert the needle at approximately 2 cm inferior to the posterolateral corner of the acromion and direct it anteriorly toward the coracoid process, aiming upward at a 10° angle.
If the needle encounters the acromion, retract the needle approximately 1 mm.
Gently pull back on the plunger prior to injection to exclude intravascular placement.
Slowly inject the anesthetic/glucocorticoid mixture and withdraw the needle.
If the injection meets resistance, the needle tip may be within the supraspinatus tendon. Stop injecting, partially withdraw the needle, and then re-advance it more superiorly until the injection does not meet resistance.
Pain is immediately relieved after a properly placed injection of anesthetic.
Apply an adhesive bandage or sterile dressing.
Aftercare for Injecting a Subacromial Bursa
Prescribe limited activity but do not immobilize the shoulder (to avoid a frozen shoulder, also called adhesive capsulitis).
Advise use of ice, and, if not contraindicated, oral nonsteroidal anti-inflammatory drugs (NSAIDs) until pain subsides.
Instruct the patient to return for reassessment to exclude infection if pain is continuously and progressively increasing after several hours or persists for > 48 hours, or if new pain arises after the injection.
Begin gentle range-of-motion exercises after 24 hours and increase the intensity after 2 weeks.
Warnings and Common Errors for Injecting a Subacromial Bursa
To avoid damaging tendons, do not inject glucocorticoids against resistance.
Tips and Tricks for Injecting a Subacromial Bursa
To increase opening into the subacromial space when using the lateral approach, have the patient hook their fingers around the cushion of the examination table, relax the shoulder muscles, and lean to the contralateral side.
Reference
1. Yui JC, Preskill C, Greenlund LS. Arthrocentesis and joint injection in patients receiving direct oral anticoagulants. Mayo Clin Proc 92(8):1223–1226, 2017. doi: 10.1016/j.mayocp.2017.04.007





