

Several distinct congenital or acquired syndromes involve abnormal mucosal or submucosal blood vessels in the gastrointestinal tract. These vessels may cause recurrent bleeding, which is rarely massive. Diagnosis is by endoscopy and sometimes angiography. Treatment is endoscopic hemostasis; occasionally, angiographic embolization or surgical resection may be needed.
Vascular ectasias (angiodysplasias, arteriovenous malformations) are dilated, tortuous vessels that typically develop in the cecum and ascending colon. They occur mainly in people > age 60 and are the most common cause of lower gastrointestinal (GI) bleeding in that age group (1). They are thought to be degenerative and do not occur in association with other vascular abnormalities. Most patients have 2 or 3 lesions, which are typically 0.5 to 1.0 cm, bright red, flat or slightly raised, and covered by very thin epithelium.
Vascular ectasias also occur in association with a number of systemic diseases (eg, renal failure, aortic stenosis, cirrhosis, CREST syndrome [calcinosis cutis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, telangiectasias]) and after radiation to the bowel.


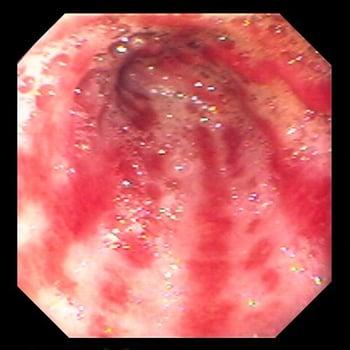
This photo shows vascular ectasia in the bowel wall.
Gastric antral vascular ectasia (watermelon stomach or GAVE) consists of large dilated veins running linearly along the stomach, creating a striped appearance suggestive of a watermelon. The condition occurs mainly in older adults and is of unknown etiology, although it has been strongly associated with cirrhosis (2, 3).
Gastric antral vascular ectasias (GAVEs) are large, dilated veins running linearly along the stomach in a pattern resembling a watermelon.
Hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome) is an autosomal dominant disorder that causes multiple vascular lesions in various parts of the body, including the entire GI tract. GI bleeding rarely occurs before age 50 (4).
Dieulafoy lesion is an abnormally large artery that penetrates the gut wall, occasionally eroding through the mucosa and causing massive bleeding. It occurs mainly in the proximal stomach.
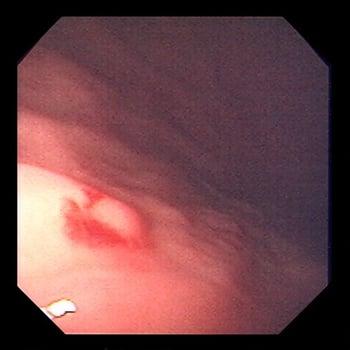
Dieulafoy lesion is a large artery that penetrates the gastric wall. It is significant because it can erode through the mucosa and cause massive hemorrhage.
Arteriovenous malformations and hemangiomas, both congenital disorders of blood vessels, can occur in the GI tract but are rare.
References
1. Bermont A, Abu-Freha N, Cohen DL, Abu-Kaf H, Abu Juma A, Abu Galion F, Aminov R, Shirin H. Epidemiology and risk factors for angiodysplasias of the upper and lower gastrointestinal tract: A large population-based study. Dig Liver Dis. 2025 Jan;57(1):220-224. doi: 10.1016/j.dld.2024.07.037
2. Thomas A, Koch D, Marsteller W, Lewin D, Reuben A. An Analysis of the Clinical, Laboratory, and Histological Features of Striped, Punctate, and Nodular Gastric Antral Vascular Ectasia. Dig Dis Sci. 2018 Apr;63(4):966-973. doi: 10.1007/s10620-018-4965-z
3. Selinger CP, Ang YS. Gastric antral vascular ectasia (GAVE): an update on clinical presentation, pathophysiology and treatment. Digestion. 2008;77(2):131-7. doi: 10.1159/000124339
4. McDonald J, Stevenson DA. Hereditary Hemorrhagic Telangiectasia. 2000 Jun 26 [updated 2021 Nov 24]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025.
Symptoms and Signs of Vascular GI Lesions
Vascular lesions are painless.
Patients often present with heme-positive stools or modest amounts of bright red blood from the rectum. Bleeding is often intermittent, sometimes with long periods between episodes. Patients with upper GI lesions may present with melena.
Major bleeding is unusual except in patients who have bleeding resulting from a Dieulafoy lesion.
Diagnosis of Vascular GI Lesions
Endoscopy
Vascular lesions are most commonly diagnosed endoscopically.
If routine endoscopy is nondiagnostic, small-bowel endoscopy, capsule endoscopy, intraoperative endoscopy, or visceral angiography may be required.
Technetium-99m–labeled red blood cell scans are less specific but may help localize the lesion enough to facilitate endoscopy or angiography.
Treatment of Vascular GI Lesions
Endoscopic coagulation
Endoscopic coagulation (with heater probe, laser, argon plasma, or bipolar electrocoagulation) is effective for many vascular lesions. Vascular ectasias are treated with endoscopic coagulation if they are thought to be the cause of bleeding. Endoscopic clips may be applied to some lesions. Vascular lesions often recur, although there is some evidence that somatostatin analogs such as octreotide may reduce transfusions and endoscopic procedures needed (Endoscopic coagulation (with heater probe, laser, argon plasma, or bipolar electrocoagulation) is effective for many vascular lesions. Vascular ectasias are treated with endoscopic coagulation if they are thought to be the cause of bleeding. Endoscopic clips may be applied to some lesions. Vascular lesions often recur, although there is some evidence that somatostatin analogs such as octreotide may reduce transfusions and endoscopic procedures needed (1, 2).
The risk of rebleeding after endoscopic intervention for vascular lesions has been estimated at approximately one-third of patients (1). Mild recurrent bleeding can be treated simply with chronic iron therapy.
More significant bleeding that is unresponsive to endoscopic measures may require angiographic embolization or surgical resection. The risk of rebleeding is lower than after endoscopic intervention (3).
Treatment references
1. Sengupta N, Feuerstein JD, Jairath V, et al. Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline. Am J Gastroenterol. 2023;118(2):208-231. doi:10.14309/ajg.0000000000002130.
2. Becq A, Sidhu R, Goltstein LCMJ, Dray X. Recent advances in the treatment of refractory gastrointestinal angiodysplasia. United European Gastroenterol J. 2024;12(8):1128-1135. doi:10.1002/ueg2.12648
3. Omori J, Kaise M, Nagata N, Aoki T, et al. Characteristics, outcomes, and risk factors of surgery for acute lower gastrointestinal bleeding: nationwide cohort study of 10,342 hematochezia cases. J Gastroenterol. 2024 Jan;59(1):24-33. doi: 10.1007/s00535-023-02057-9.
Key Points
A variety of inherited and acquired vascular abnormalities can cause mild to moderate GI bleeding (usually lower).
Preferred treatment is endoscopy with coagulation of lesions.





