

Atherosclerosis is a condition where fatty deposits build up in the walls of medium-sized and large arteries (atheromas or atherosclerotic plaques), leading to reduced or blocked blood flow. This can affect the heart, brain, kidneys, limbs, and other parts of the body. Atherosclerosis of the arteries that supply blood to the heart causes coronary artery disease, which is the world's leading cause of death.
Atherosclerosis is caused by repeated injury to the walls of arteries. Many factors contribute to this damage, including high blood pressure, smoking, diabetes, and high cholesterol.
The first sign may be pain or cramping when the tissues don't get enough oxygen.
To prevent atherosclerosis, people need to quit smoking, eat healthy foods, exercise regularly, and maintain control of their blood pressure, cholesterol, and diabetes. Medication may be necessary in some people.


Causes of Atherosclerosis
The development of atherosclerosis is complicated, but the primary event seems to be repeated, slight injury to the inner lining of arteries (endothelium), through various mechanisms. These mechanisms include:
Physical stress from disrupted blood flow (especially where arteries branch, particularly in people who have high blood pressure)
Inflammation-related stress involving the immune system (such as smoking), or from infections with certain types of bacteria or viruses
Chemical abnormalities in the bloodstream (such as high cholesterol or high blood sugar as occurs in diabetes mellitus)
See Risk Factors for Atherosclerosis for more information on specific causes.
Plaque formation

This photo shows an atherosclerotic plaque (atheroma; see arrow) visible in an artery.
BSIP VEM/SCIENCE PHOTO LIBRARY
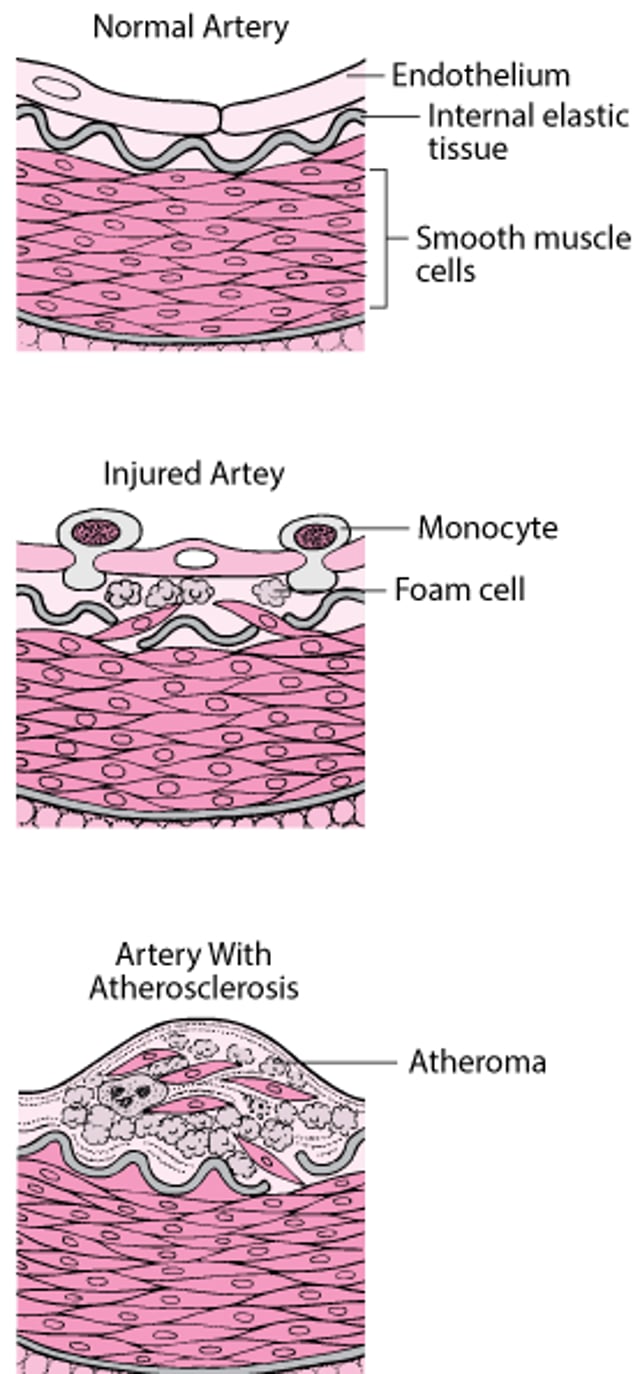
Atherosclerosis begins when the injured artery wall creates chemical signals that cause certain types of white blood cells (monocytes and T cells) to attach to the wall of the artery. These cells move into the wall of the artery and transform into foam cells, which collect cholesterol and other fatty materials. Foam cells trigger growth of other cells such as smooth muscle cells in the artery wall. In time, these foam cells accumulate. They form patchy deposits (atheromas, also called plaques) covered with a fibrous cap in the lining of the artery wall. With time, calcium accumulates in the plaques. Plaques may be scattered throughout medium-sized and large arteries, but they usually start where the arteries branch.
How Atherosclerosis Develops
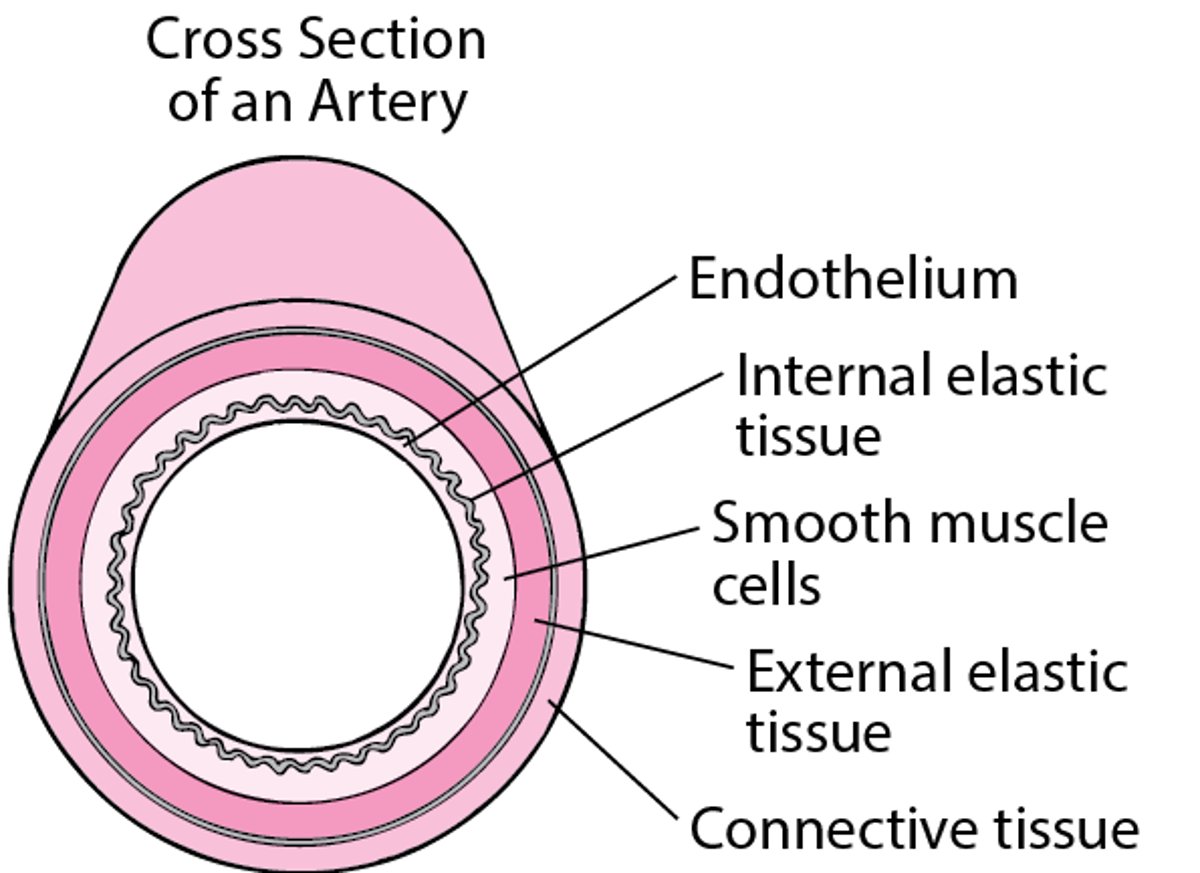
The wall of an artery is composed of several layers. The lining or inner layer (endothelium) is usually smooth and unbroken. Atherosclerosis begins when the lining is injured or diseased. Then certain white blood cells called monocytes and T cells are activated and move out of the bloodstream and through the lining of an artery into the artery’s wall. Inside the lining, they are transformed into foam cells, which are cells that collect fatty materials, mainly cholesterol. In time, smooth muscle cells move from the middle layer into the lining of the artery’s wall and multiply there. Connective and elastic tissue materials also accumulate there, as may cell debris, cholesterol crystals, and calcium. This accumulation of fat-laden cells, smooth muscle cells, and other materials forms a patchy deposit called an atheroma or atherosclerotic plaque. This plaque is covered by a fibrous cap. As they grow, some plaques thicken the artery’s wall and bulge into the channel of the artery. These plaques may narrow or block an artery, reducing or stopping blood flow. Other plaques do not block the artery very much but the fibrous cap may split open, releasing the material inside the plaque and triggering a blood clot that suddenly blocks the artery. | |


Plaque rupture
Plaques can grow inside the artery, making it narrower. When atherosclerosis narrows an artery, tissues supplied by the artery may not receive enough blood and oxygen. Plaques also can grow into the wall of the artery, where they do not block blood flow. Both kinds of plaques can split open (rupture), exposing the material within to the blood and leading to blood clot formation. These blood clots can suddenly block all blood flow through the artery, which is the main cause of a heart attack or stroke. Sometimes these blood clots or pieces of the plaque can break off, travel through the bloodstream, and block an artery elsewhere in the body.
Risk Factors for Atherosclerosis
(See also Prevention of coronary artery disease.)
Risk factors that cannot be modified include:
Older age
Male sex (though atherosclerosis is increasingly more recognized in women)
Family history: Having a close male relative who had a stroke or heart attack before age 55 years or having a close female relative who had a stroke or heart attack before age 65 years
South Asian ancestry
Risk factors that can be modified include:
Factors related to lifestyle
Tobacco smoking
Physical inactivity
Diets high in salt, certain kinds of fats, and sugar; diets low in fruits and vegetables
Chronic stress, anger and hostility, depression, and anxiety
Heavy alcohol intake
Abnormal cholesterol levels
Other diseases affecting the heart, kidneys, and metabolism
Diabetes or prediabetes (a precursor of diabetes involving abnormal blood sugar or resistance to the action of insulin in the body)
High blood pressure
Obesity
Chronic kidney disease
Inflammation
High C-reactive protein level (a protein associated with inflammation)
Autoimmune or inflammatory diseases, such as rheumatoid arthritis, systemic lupus erythematosus, psoriasis, vasculitis
Some cancer-like mutations in blood-forming stem cells
Infections
HIV
Chlamydia pneumoniae
Cytomegalovirus
Helicobacter pylori
Periodontal disease
Severe acute respiratory syndrome coronavirus-2 (COVID-19)
Influenza (flu)
Respiratory syncytial virus (RSV)
Abnormal cholesterol levels
A high level of LDL (low density lipoprotein) cholesterol is an important modifiable risk factor. A diet that is high in saturated fats (see Types of Fat) causes LDL cholesterol levels to increase in susceptible people. Cholesterol levels also increase as people age and are normally higher in men than in women, although levels increase in women after menopause. Several hereditary disorders result in high levels of cholesterol or other fats. People with these hereditary disorders can have extremely high levels of LDL cholesterol and (if untreated) die of coronary artery disease at an early age.
Measurement of apolipoprotein B (ApoB) in the blood. ApoB, the protein component of LDL, is also helpful in estimating risk of atherosclerosis. ApoB is responsible for transporting cholesterol in the blood, leading to more plaque in the arteries.
Not all high cholesterol levels increase the risk of atherosclerosis. A higher level of HDL (high density lipoprotein, also called "good cholesterol") decreases the risk of atherosclerosis.
Lipoprotein(a) is another cholesterol-containing particle that also contributes to heart attacks and strokes.
High triglyceride levels also slightly increase the risk of atherosclerosis.
The table provides levels of total cholesterol, LDL cholesterol, and HDL cholesterol that help reduce the risk of developing atherosclerosis.
Diseases affecting the heart, kidneys, and metabolism (cardiovascular-kidney-metabolic syndrome)
Uncontrolled high blood pressure is a risk factor for atherosclerosis, as well as for events such as heart attack and stroke that are caused by atherosclerosis. The risk of cardiovascular disease starts increasing when blood pressure levels are above 115/75 mm Hg.
People who have diabetes mellitus tend to develop disease that affects small arteries, such as those in the eyes, nerves, and kidneys, leading to vision loss, nerve damage, and chronic kidney disease. People with diabetes also tend to develop atherosclerosis in large arteries.
Obesity, particularly abdominal (truncal) obesity, increases the risk of coronary artery disease. Abdominal obesity increases the risk of other risk factors for atherosclerosis: high blood pressure, type 2 diabetes, and high cholesterol levels.
Inflammation
Inflammation is a normal response to injury or infection. But when inflammation is prolonged, it damages blood vessels, increasing the risk of atherosclerosis. Conditions that contribute to long-term inflammation are therefore risk factors for atherosclerosis.
Elevated levels of C-reactive protein (CRP) are an indication of inflammation and are associated with an increased risk of cardiovascular events.
Autoimmune diseases, such as rheumatoid arthritis, systemic lupus erythematosus, and Addison disease, are also associated with an increased risk of developing atherosclerosis.
Clonal hematopoiesis of indeterminate potential (CHIP) is a condition in which genetic mutations in blood cells occur in people who do not have other blood cell abnormalities. Affected people have nearly twice the risk of developing coronary artery disease or having a heart attack at a young age.
Infections
Infection may also play a role in the development of atherosclerosis. Individuals with human immunodeficiency virus (HIV) infection are at increased risk for developing myocardial infarction and other atherosclerotic complications for several reasons. Individuals with HIV infection are more likely to have traditional risk factors for atherosclerosis such as male sex, higher cholesterol levels, high blood pressure, diabetes, and smoking. The HIV virus also directly affects the cells of the blood vessels and influences how the body processes cholesterol.
Other infections such as Chlamydia pneumoniae, cytomegalovirus, Helicobacter pylori, COVID-19, those associated with periodontal disease, and others may cause damage to lining of blood vessels, increasing the risk of atherosclerosis.
Lifestyle factors
One of the most important modifiable risk factors is smoking. Using other forms of tobacco, such as snuff and chewing tobacco, or even exposure to secondhand smoke also increases risk. A smoker‘s risk of developing some forms of atherosclerosis such as coronary artery disease is directly related to the amount of tobacco smoked daily. Tobacco use decreases the level of high-density lipoprotein (HDL) cholesterol—the “good” cholesterol—and increases the level of low-density lipoprotein (LDL) cholesterol. Smoking increases the level of carbon monoxide in the blood, which may increase the risk of injury to the lining of the artery‘s wall. Tobacco use causes arteries already narrowed by atherosclerosis to constrict, further decreasing the amount of blood reaching the tissues. In addition, tobacco use increases the blood's tendency to clot (by making platelets stickier), so that it increases the risk of peripheral artery disease (atherosclerosis affecting arteries other than those that supply the heart and brain), coronary artery disease, stroke, and blockage of an arterial graft placed during coronary artery bypass surgery or surgery to bypass a blocked artery elsewhere in the body.
Other factors related to lifestyle that increase the risk of atherosclerosis include physical inactivity, diets low in fruits and vegetables and high in sugar, salt, and saturated fats, and chronic stress or hostility. Alcohol consumption is also a risk factor, with studies now showing that there is no level of alcohol consumption that does not increase risk (in contrast to older studies that showed a protective effect of low levels of alcohol consumption).
Did You Know...
|
Other risk factors
Many conditions increase the likelihood of a blood clot developing, especially at the site of an atherosclerotic plaque.
Atherosclerosis may also result from radiation therapy–induced injury to the inner walls of blood vessels, for example after a person receives chest radiation therapy for cancer. Chemotherapy given for cancer may also cause damage to the heart. In some cases, heart damage from chemotherapy may not become apparent for years after cancer treatment.
Women who have early menopause have a higher risk of developing heart disease. There is some evidence that young women with pregnancy related complications, including preeclampsia, have a higher risk of developing atherosclerosis.
Symptoms of Atherosclerosis
Symptoms depend on:
Where the affected artery is located
Whether the affected artery is gradually narrowed or suddenly blocked
Symptoms of gradual narrowing
The first symptom of a narrowed artery may be pain or cramps at times when blood flow cannot keep up with the tissues’ need for oxygen. For instance, during exercise, a person may feel chest pain or discomfort because the oxygen supply to the heart is inadequate. This chest pain (angina) may go away within minutes after the person stops exertion. While walking, a person may feel leg cramps (intermittent claudication) because the oxygen supply to the leg muscles is inadequate. If the arteries supplying one or both kidneys become narrowed, kidney failure or dangerously high blood pressure can result.
Symptoms of sudden artery blockage
If the arteries supplying the heart (coronary arteries) are blocked suddenly, a heart attack can result. The most common symptom of a heart attack is chest pain; however, people may also have shortness of breath, nausea, vomiting, sweating, palpitations, or even sudden death. Blockage in the arteries supplying the brain can cause a stroke, which may cause numbness, weakness, confusion, or difficulty speaking. Blockage of the arteries in the legs can cause severe pain, coldness, numbness or discoloration of a toe, foot, or leg.
Diagnosis of Atherosclerosis
Blood tests to look for risk factors for atherosclerosis
Imaging tests (such as computed tomography [CT], magnetic resonance imaging [MRI], ultrasound) to look for plaques or blocked arteries
How atherosclerosis is diagnosed depends on whether the person is having symptoms.
People with symptoms
People who have symptoms that suggest a blocked artery have tests to look for the location and extent of the blockage. Different tests are used depending on what organ seems to be involved. For example, if doctors suspect blockage of an artery in the heart, they typically do electrocardiography (ECG), blood tests for markers of heart injury (cardiac biomarkers), and sometimes a stress test or heart catheterization.
People with atherosclerotic arteries in one organ often have atherosclerosis in other arteries. Therefore, when doctors find atherosclerotic blockage in one artery, for example in the leg, they may do tests to look for blockage in other arteries, such as those in the heart.
Doctors also test for certain risk factors in people who have an atherosclerotic blockage. For example, they measure the levels of glucose, cholesterol, and triglycerides in the blood. Doctors can also do these tests as part of the routine yearly examination in adults.

People without symptoms (screening)
In children without significant risk factors, recommended obesity screening begins at age 2 to 6 years, blood pressure screening at age 3 years, and lipid screening at age 9 to11 years.
In people who have some risk factors for atherosclerosis but no symptoms, doctors usually do blood tests to measure the levels of glucose, cholesterol, and triglycerides in the blood. Doctors usually also do these tests as part of the routine yearly examination in adults.
Some doctors recommend using CT to detect hardened (calcified) plaque in the coronary arteries, and to measure the amount of calcium in the arteries supplying the heart. The result of this test is called the calcium score .
Prevention and Treatment of Atherosclerosis
Lifestyle changes to reduce risk of atherosclerosis, its complications, or death
Sometimes medication, catheter-based procedures, or surgery
To help prevent atherosclerosis, people need to:
Eat a healthy diet
Lower LDL cholesterol levels (treat high cholesterol, sometimes with medications such as a statin)
Lower blood glucose levels (treat diabetes)
Sometimes, take medications such as a statin even without the presence of high cholesterol
People who are actively smoking or using tobacco should stop—regardless of how long they have been smoking. The benefits of quitting tobacco use begin immediately and increase with time. A combination of nicotine-replacement therapy or other medication with counseling can help.
Making healthy dietary changes can help decrease the risk of atherosclerosis. These changes include:
Increase how much fruit, vegetables, legumes (beans), nuts, whole grains, and fish are eaten.
Eat less saturated and trans fats (for example, butter, fats in red meat and fried foods, coconut and palm oil), replacing them with healthier fats (for example, olive oil, fish oil, avocados, nuts)
Reduce salt intake
Reduce simple sugars, refined carbohydrates, sweetened beverages, and processed meats
Limit alcohol consumption
Some specific recommendations include:
Fiber intake: 30 to 45 grams per day, preferably from whole grains
Fruit consumption: At least 200 grams per day (≥ 2 to 3 servings)
Vegetable consumption: At least 200 grams per day (≥ 2 to 3 servings)
Nuts: 30 grams of unsalted nuts per day
Red meat consumption: Reduction to less than 350 to 500 grams per week
Fish consumption: 1 to 2 times per week.
Fat is an essential part of the diet. The notion that eating less fat is important to a healthy diet is only partly true because the type of fat also matters. Fats may be soft (or liquid) or firm at room temperature. Soft fats, such as oils and some margarines, tend to be higher in polyunsaturated and monounsaturated fats. Hard fats, such as butter and shortening, tend to be higher in saturated and trans fats. Saturated and trans fats are more likely to cause atherosclerosis. Thus, whenever possible, people should limit the amount of saturated and trans fats in their diet and choose foods with monounsaturated or polyunsaturated fats instead. Saturated and trans fats are found in red meat, many fast food items, full-fat dairy products (such as cheese, butter, and cream), and hard (stick) margarines. Monounsaturated fats are found in canola and olive oil, soft margarines with no trans fat, nuts, and olives. Polyunsaturated fats are found in fatty fish and certain nuts, seeds, and oils.
Physical inactivity increases the risk of developing coronary artery disease, and regular exercise even to a moderate degree reduces this risk and decreases the risk of death. Exercise in combination with dietary changes can also help modify other risk factors for atherosclerosis—by lowering blood pressure and cholesterol levels, by helping with weight loss, and decreasing insulin resistance.
People who have high blood pressure should lower their blood pressure with lifestyle changes (including sodium reduction) and medication. People who have diabetes must maintain strict control of their blood sugar. Even in people without diabetes, reducing sugar consumption can lower the risk of atherosclerosis.
Even a small amount of alcohol consumption is associated with increased atherosclerotic disease risk, challenging the belief that low or moderate levels of alcohol consumption can protect against heart disease. For those who continue to drink alcohol, consumption should be limited to less than about 1 drink daily for women and 2 drinks daily for men and binge drinking should be avoided.
People at high risk for atherosclerosis might need medications. Helpful medications include those that lower cholesterol (statins, ezetimibe, evolocumab, and alirocumab), and in some cases, aspirin or other medications that keep platelets from sticking together and forming blood clots in blood vessels. Statins can cause muscle pain and weakness and people may need to be monitored for these and other side effects. People at high risk for atherosclerosis might need medications. Helpful medications include those that lower cholesterol (statins, ezetimibe, evolocumab, and alirocumab), and in some cases, aspirin or other medications that keep platelets from sticking together and forming blood clots in blood vessels. Statins can cause muscle pain and weakness and people may need to be monitored for these and other side effects.Aspirin and other platelet-targeting medications can cause bleeding. Some medications used to treat high blood pressure and some medications used to treat diabetes also help reduce risk of atherosclerosis.
Treatment of atherosclerosis symptoms and complications
When atherosclerosis becomes severe enough to cause symptoms or complications, the complications themselves must be treated.
Sometimes when plaques are blocking an artery, they need to be treated with catheter-based procedures (or surgery with opening up the blood vessel to restore blood flow). During catheterization a placement of a stent, a tiny mesh tube may be needed to keep it open and ensure proper blood flow. Doctors may perform coronary artery bypass grafting surgery in which they take a healthy blood vessel from another part of the body (such as the legs or arm) and use it to create a new path around a blocked artery inthe heart to improve blood flow.


