

Bundle branch block is partial or complete interruption of impulse conduction in a bundle branch; fascicular block is similar interruption in a hemifascicle of the left bundle. The disorders often coexist. There are usually no symptoms, but presence of either suggests a heart disorder. Diagnosis is by electrocardiography. No specific treatment is indicated.
(See also Overview of Arrhythmias.)
Conduction blocks (see figure ) can be caused by many heart disorders, including intrinsic degeneration without another associated heart disorder.
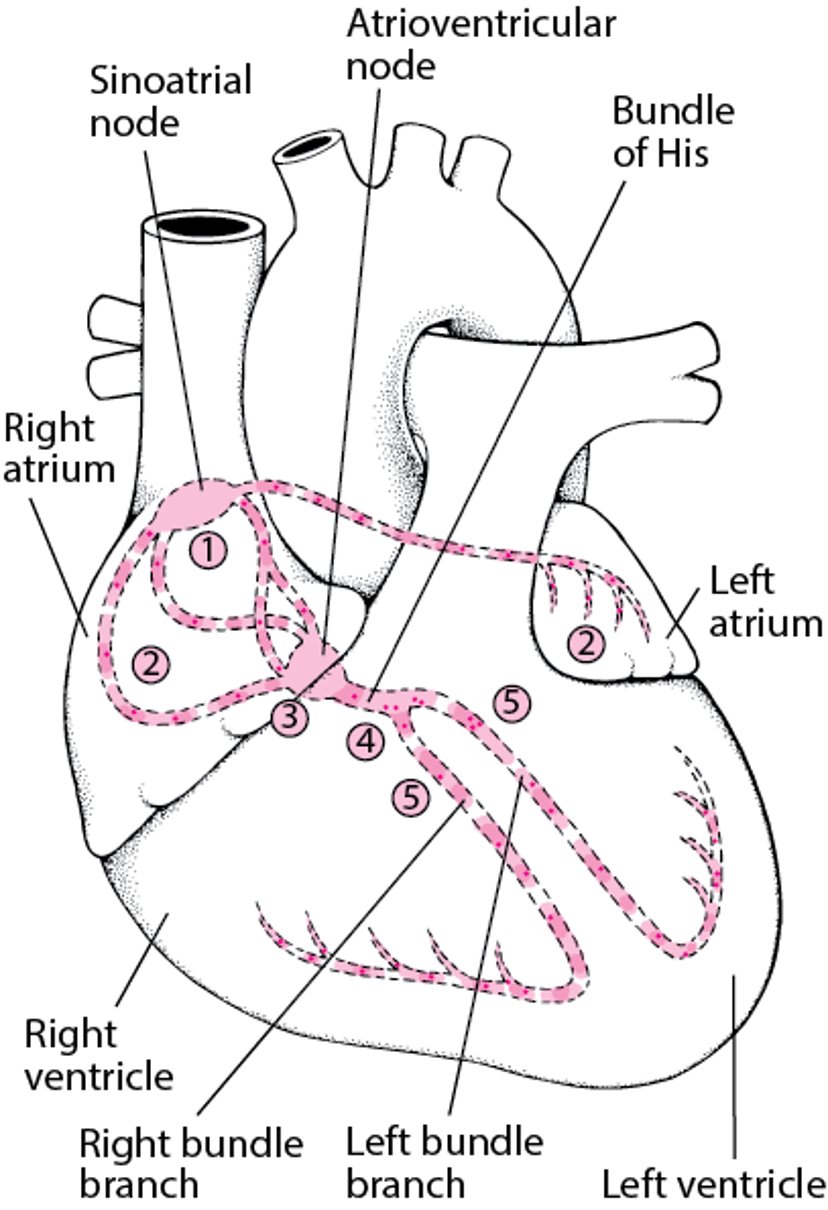
Electrical Pathway Through the Heart
The sinoatrial (sinus) node (1) initiates an electrical impulse that flows through the right and left atria (2), making them contract. When the electrical impulse reaches the atrioventricular node (3), it is delayed slightly. The impulse then travels down the bundle of His (4), which divides into the right bundle branch for the right ventricle (5) and the left bundle branch for the left ventricle (5). The impulse then spreads through the ventricles, making them contract. |

In adults, the 2 ventricles are normally activated simultaneously such that the QRS duration is ≤ 0.11 second. When the ventricles are activated sequentially, the QRS duration is > 0.12 seconds. A wide QRS can result from activation of one ventricle early as in a rhythm originating in a ventricle (a ventricular rhythm or a ventricular paced rhythm) or as in ventricular pre-excitation (see figure ) or from activating one ventricle late as in right or left bundle branch block.
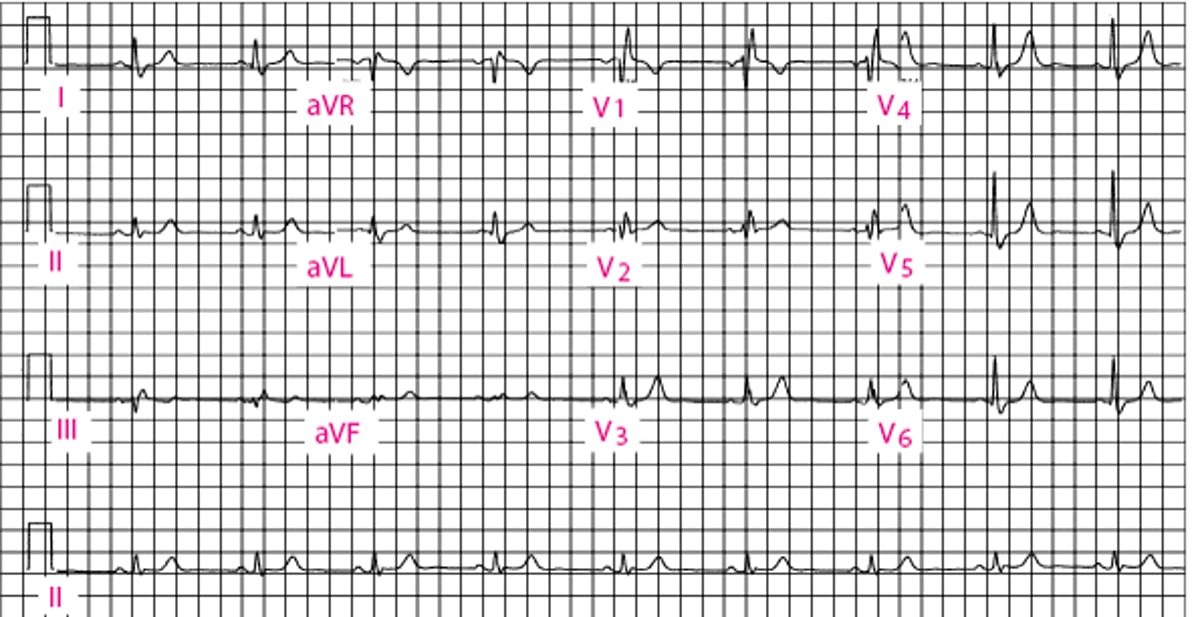
Right bundle branch block (RBBB—see figure ) criteria on the ECG in adults (1) are as follows:
A QRS duration ≥ 0.12 second
rsr', rsR' or rSR' QRS pattern in leads V1 or V2
Delayed right ventricular activation time shown by a QRS onset to peak of last R wave time of > 0.05 second in lead V1
Normal left ventricular activation time shown by a QRS onset to peak of last R wave time of < 0.045 second in leads V5 and V6
S duration greater than R duration or S duration > 0.04 second in leads I and V6
RBBB produces secondary repolarization changes consisting of ST depression and T wave inversion particularly in V1. Incomplete right bundle branch block (also called right ventricular conduction delay) has the same ECG criteria as RBBB with a QRS duration > 0.11 second but < 0.12 second. When lead V1 shows a qR pattern while the other criteria for RBBB are met, RBBB and septal myocardial infarction (or other septal damage) are diagnosed.
RBBB can occur in people with no evidence of heart disease (2). It may also occur with anterior myocardial infarction, indicating substantial myocardial injury. Transient RBBB may occur after pulmonary embolism and indicates significant right ventricular dysfunction. The presence of RBBB should prompt a search for underlying cardiac pathology (2), but often none is found. Although RBBB distorts the QRS complex, it does not significantly interfere with ECG criteria of past myocardial infarction.
In the absence of evidence of a heart disorder or more advanced interventricular conduction disturbance, RBBB does not appear to indicate a higher risk of future cardiovascular events. Also, isolated RBBB produces no symptoms. Thus, isolated RBBB requires no specific therapy (3).
Right Bundle Branch Block

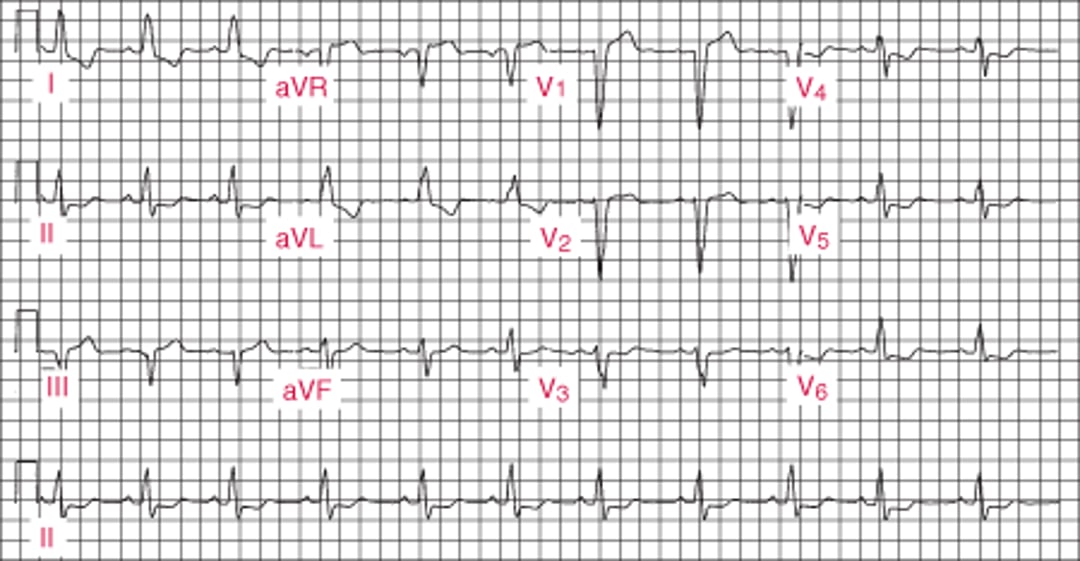
Left bundle branch block (LBBB—see figure ) criteria on the ECG in adults are (1)
A QRS duration ≥ 0.12 second
Broad notched or slurred R wave and absent Q waves in leads I, aVL, V5 and V6
Delayed left ventricular activation time shown by a QRS onset to peak of last R wave time of > 0.06 second in lead V5 and V6
Normal right ventricular activation time shown by a QRS onset to peak of last R wave time of < 0.035 second in lead V1
LBBB produces secondary repolarization changes consisting of ST and T wave deviation in the opposite direction of the QRS complex. Incomplete left bundle branch block (also called left ventricular conduction delay) has the same ECG criteria as LBBB with a QRS duration > 0.11 second but < 0.12 second. When lead aVL shows a significant q wave while the other criteria for LBBB are met, LBBB and septal myocardial infarction (or other septal damage) are diagnosed. Otherwise, LBBB precludes use of the usual ECG criteria of past myocardial infarction.
LBBB is associated with a structural heart disorder more often than is RBBB and, in contrast to RBBB, LBBB is associated with a higher risk of future cardiac events and mortality. It may also occur with anterior myocardial infarction, indicating substantial myocardial injury. The presence of LBBB should prompt a search for underlying cardiac pathology, which is present more often than in patients with RBBB (3).
Isolated LBBB rarely produces symptoms but may produce interventricular mechanical dyssynchrony that reduces the efficiency of left ventricular systolic function and may contribute to heart failure, particularly in association with other heart disorders that reduce left ventricular systolic function. Resynchronization pacing therapy is then of benefit (4).
Left Bundle Branch Block


Fascicular block involves the anterior or posterior fascicle of the left bundle branch. Interruption of the left anterior fascicle causes left anterior hemiblock characterized by (1)
Modest QRS prolongation (< 0.12 second)
A frontal plane QRS axis more negative than −45° (left axis deviation)
A qR pattern in lead aVL
Delayed left anterolateral ventricular activation time shown by a QRS onset to peak of last R wave time of > 0.045 second in lead aVL
Interruption of the left posterior fascicle causes left posterior hemiblock characterized by (1)
Modest QRS prolongation (< 0.12 second)
A frontal plane QRS axis more positive than +120°
An rS pattern in lead aVL
A qR pattern in leads II and aVF
The associations between hemiblocks and a structural heart disorder are the same as for LBBB. Isolated left posterior hemiblock is rare. Isolated left anterior hemiblock is more common and does not appear to be independently associated with an increased risk of future cardiac events or mortality.
Hemiblocks may coexist with other conduction disturbances: RBBB and left anterior or posterior hemiblock (bifascicular block); and RBBB, left anterior or posterior hemiblock, and first-degree atrioventricular (AV) block (sometimes incorrectly called trifascicular block; incorrectly because first-degree block is usually AV nodal in origin).
Trifascicular block refers to RBBB with alternating left anterior and left posterior hemiblock or alternating LBBB and RBBB. Presence of bifascicular or trifascicular block after myocardial infarction implies extensive cardiac damage.
Bifascicular blocks require no direct treatment unless intermittent second- or third-degree AV block is present. True trifascicular blocks require immediate, then permanent pacing (3).
Nonspecific intraventricular conduction defects are diagnosed when the QRS complex is prolonged (> 0.12 second), but the QRS pattern is not typical of LBBB or RBBB (1). The conduction delay may occur beyond the Purkinje fibers and result from slow cell-to-cell myocyte conduction. Risk of subsequent cardiac events and mortality with nonspecific intraventricular conduction defect is similar to that of a LBBB. Accordingly, evaluation for an underlying structural heart disorder is indicated. Isolated intraventricular conduction delay produces no symptoms. No specific treatment is indicated (3).
References
1. Surawicz B, Childers R, Deal BJ, et al: AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol 53(11):976–981, 2009. doi: 10.1016/j.jacc.2008.12.013
2. MacLachlan H, Antonakaki A, Bhatia R, et al: Prevalence and Clinical Significance of Electrocardiographic Complete Right Bundle Branch Block in Young Individuals. Eur J Prev Cardiol 2024 Feb 27:zwae082, 2024. doi: 10.1093/eurjpc/zwae082
3. Kusumoto FM, Schoenfeld MH, Barrett C, et al: 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 16(9):e128–e226, 2019. doi: 10.1016/j.hrthm.2018.10.037
4. Wells G, Parkash R, Healey JS, et al: Cardiac resynchronization therapy: a meta-analysis of randomized controlled trials. CMAJ 183(4):421–429, 2011. doi: 10.1503/cmaj.101685





