

A ventricular septal defect (VSD) is an opening in the interventricular septum, causing a shunt between ventricles. Large defects result in a significant left-to-right shunt and cause dyspnea with feeding and poor growth during infancy. A loud, harsh, holosystolic murmur at the lower left sternal border is common. Recurrent respiratory infections and heart failure may develop. Diagnosis is by echocardiography. Defects may close spontaneously during infancy or require surgical repair.
(See also Overview of Congenital Cardiovascular Anomalies.)
Ventricular septal defect (see figure ) is the 2nd most common congenital heart anomaly after bicuspid aortic valve, accounting for 20% of all defects. It can occur alone or with other congenital anomalies (eg, tetralogy of Fallot, complete atrioventricular septal defects, transposition of the great arteries).
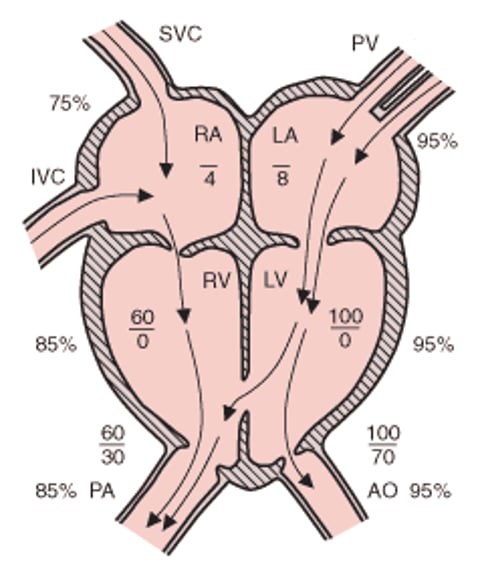
Ventricular septal defect
Pulmonary blood flow and LA and LV volumes are increased. Atrial pressures are mean pressures. RV pressure and O2 saturation are variably elevated, positively related to defect size. AO = aorta; IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PV = pulmonary veins; RA = right atrium; RV = right ventricle; SVC = superior vena cava. |

Classification
Most ventricular septal defects are classified by location:
Perimembranous (also called conoventricular)
Trabecular muscular
Subpulmonary outlet (supracristal, conoseptal, doubly committed subarterial)
Inlet (atrioventricular septal type, atrioventricular canal type)
Perimembranous defects (70 to 80%) are defects in the membranous septum adjacent to the tricuspid valve and they extend into a variable amount of surrounding muscular tissue; the most common type of this defect occurs immediately below the aortic valve.
Trabecular muscular defects (5 to 20%) are completely surrounded by muscular tissue and may occur anywhere in the septum.
Subpulmonary outlet defects (5 to 7% in the United States; about 30% in Far Eastern countries) occur in the ventricular septum immediately under the pulmonary valve. These defects are often referred to as supracristal, conoseptal, or doubly committed subarterial defects and are frequently associated with aortic leaflet prolapse into the defect, causing aortic regurgitation.
Inlet defects (5 to 8%) are bordered superiorly by the tricuspid annulus and are located posterior to the membranous septum. These defects are sometimes referred to as atrioventricular septal-type defects.
Malalignment type ventricular septal defects are characterized by displacement of the conal or outlet septum. When the conal septum is malaligned anteriorly, it protrudes into the right ventricular outflow tract often resulting in obstruction, as occurs in tetralogy of Fallot. When the conal septum is malaligned posteriorly, there may be left ventricular outflow tract obstruction. These VSDs occur in the same location as perimembranous VSDs but represent an important subset with different physiology related to this outflow tract obstruction.
Pathophysiology of VSD
The magnitude of the shunt depends on defect size and downstream resistance (ie, pulmonary outflow tract obstruction and pulmonary vascular resistance).
In nonrestrictive ventricular septal defects, pressure equalizes between the right and left ventricles and there is a large left-to-right shunt. Assuming there is no pulmonic stenosis, severe pulmonary hypertension is present because systemic LV pressure is directly transmitted to the right ventricle and pulmonary artery. Initially, there is a large left-to-right shunt with volume overload of the left and right ventricles. Over time, the large shunt causes elevated pulmonary artery vascular resistance with increased right ventricular pressure overload and right ventricular hypertrophy. Ultimately, the increased pulmonary vascular resistance causes shunt direction to reverse (from the right to the left ventricle), leading to Eisenmenger syndrome.
Restrictive ventricular septal defects, which are smaller defects, limit the flow of blood and the transmission of high pressure to the right heart. Small VSDs result in a relatively small left-to-right shunt, and pulmonary artery pressure is normal or minimally elevated. Heart failure, pulmonary hypertension, and Eisenmenger syndrome do not develop.
Moderate VSDs result in a moderately large left-to-right shunt, but normal or only mild-to-moderate pulmonary hypertension. The clinical manifestations may be minimal, or some degree of heart failure symptoms may be present because of the pulmonary overcirculation.

Symptoms and Signs of VSD
Symptoms depend on defect size and magnitude of the left-to-right shunt. Children with a small ventricular septal defect are typically asymptomatic and grow and develop normally. In children with a larger defect, symptoms of heart failure (eg, respiratory distress, poor weight gain, fatigue after feeding) appear at age 4 to 6 weeks when pulmonary vascular resistance falls. Frequent lower respiratory tract infections may occur. Eventually, over years, untreated patients may develop symptoms of Eisenmenger syndrome.
Auscultatory findings vary with the size of the defect. Small VSDs typically produce murmurs ranging from a grade 1 to 2/6 high-pitched, short systolic murmur (due to tiny defects that actually close during late systole) to a grade 3 to 4/6 holosystolic murmur (with or without thrill) at the lower left sternal border; this murmur is usually audible within the first few days of life (see table ). The precordium is not hyperactive, and the second heart sound (S2) is normally split and has normal intensity.
Moderate VSDs produce a holosystolic murmur that is present by age 2 to 3 weeks; S2 is usually narrowly split with an accentuated pulmonary component. An apical diastolic rumble (due to increased flow through the mitral valve) and findings of heart failure (eg, tachypnea, dyspnea with feeding, failure to thrive, gallop, crackles, hepatomegaly) may be present. In moderate, high-flow VSDs, the murmur is often very loud and accompanied by a thrill (grade 4 or 5 murmur). With large defects allowing equalization of left ventricular and right ventricular pressures, the systolic murmur is often attenuated.

Diagnosis of VSD
Chest x-ray and ECG
Echocardiography
Diagnosis of ventricular septal defect is suggested by clinical examination, supported by chest x-ray and ECG, and established by echocardiography.
If the VSD is large, chest x-ray shows cardiomegaly and increased pulmonary vascular markings. ECG shows right ventricular hypertrophy or combined ventricular hypertrophy and, occasionally, left atrial enlargement. ECG and chest x-ray are typically normal if the VSD is small.
Two-dimensional echocardiography with color flow and Doppler studies establishes the diagnosis and can provide important anatomic and hemodynamic information, including the defect’s location and size and right ventricular pressure. Cardiac catheterization is not necessary for diagnosis but may be used to evaluate the degree of pulmonary hypertension and pulmonary overcirculation and assess pulmonary vascular resistance.
Treatment of VSD
For heart failure, medical therapy (eg, diuretics, digoxin, angiotensin-converting enzyme [ACE] inhibitors)For heart failure, medical therapy (eg, diuretics, digoxin, angiotensin-converting enzyme [ACE] inhibitors)
Sometimes surgical repair
Small ventricular septal defects (< 5 mm), particularly muscular septal defects, often close spontaneously during the first few years of life. A small defect that remains open does not require medical or surgical therapy. Larger defects are less likely to close spontaneously.
Diuretics, digoxin, and ACE inhibitors may be useful to control symptoms of Diuretics, digoxin, and ACE inhibitors may be useful to control symptoms ofheart failure before cardiac surgery or to temporize in infants with moderate VSDs that seem likely to close spontaneously over time. If infants do not respond to medical treatment or have poor growth, surgical repair is often recommended during the first few months of life.
Even in asymptomatic children, large VSDs with pulmonary hypertension should be repaired, usually within the first year of life, to prevent later complications, particularly persistent pulmonary hypertension and pulmonary vascular disease leading to Eisenmenger syndrome. Children who are healthy without any symptoms or elevated pulmonary artery pressure, but have a persistent shunt large enough to result in left ventricular volume overload, should have their defects closed by 3 to 4 years of age to prevent late complications.
The surgical mortality rate is < 2%. Surgical complications may include residual ventricular shunt and/or complete heart block.
Transcatheter closure of some defects may be possible but is rarely considered a preferable option.
Endocarditis prophylaxis is not needed preoperatively and is required only for the first 6 months after repair or if there is a residual defect adjacent to a surgical patch.
Key Points
A ventricular septal defect (VSD) is an opening in the interventricular septum, causing a left-to-right shunt.
Over time, large left-to-right shunts cause pulmonary artery hypertension, elevated pulmonary artery vascular resistance, right ventricular pressure overload, and right ventricular hypertrophy and ultimately cause shunt direction to reverse, leading to Eisenmenger syndrome.
Larger defects cause symptoms of heart failure by age 4 to 6 weeks.
Typically, a grade 3 to 4/6 holosystolic murmur at the lower left sternal border is audible shortly after birth.
Infants who do not respond to medical treatment of heart failure or have poor growth should have surgical repair during the first few months of life; even asymptomatic children with large VSDs should have repair during the first year of life.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers





