

Blastomycosis is a pulmonary disease caused by inhaling spores of the dimorphic fungal genus Blastomyces. Two main species have been identified: B. dermatitidis and B. gilchristii. Occasionally, the fungi spread hematogenously, causing extrapulmonary disease. Symptoms result from pneumonia or from dissemination to multiple organs, most commonly the skin. Diagnosis is primarily clinical, by chest radiography, or both and is confirmed by laboratory identification of the fungi. For mild to moderate infections that do not involve the central nervous system and do not require hospitalization, itraconazole is the recommended treatment. For severe infections, treatment is initiated with a lipid formulation of amphotericin B. After clinical improvement, patients can be transitioned to itraconazole.
Blastomycosis is a rare disease. In one report from the United States, 240 cases of blastomycosis were reported in 2019, and hospitalization rates were high (65%) (1). It predominantly affects adults and is characterized by a marked male predominance, accounting for approximately 70% of cases. This predominance may likely reflect selective occupational and/or recreational exposures (in males) to moist soil and decaying vegetation, which are the primary reservoirs. A seasonal variation has been observed, with a slight increase in cases during winter months.
Blastomyces grows as a mold at ambient temperature in soil enriched with animal excreta and in moist, decaying, acidic organic material, often near rivers.
In North America, the endemic area for blastomycosis includes:
Ohio and Mississippi River Valleys (extending into the middle Atlantic and southeastern states)
Northern Midwest
Upstate New York (Mohawk River Valley)
Southern Canada
Rarely, the infection occurs in the Middle East and Africa.
Immunocompetent people can contract this infection. Although blastomycosis may be more common and more severe in immunocompromised patients than in immunocompetent patients, it is a less common opportunistic infection overall than histoplasmosis or coccidioidomycosis.
Two main species have been identified: B. dermatitidis and B. gilchristii. Although these species are morphologically indistinguishable, they are genetically distinct species. Both species cause similar clinical disease.
In the lungs, inhaled spores convert into large (15 to 20 micrometers), invasive yeasts, which form characteristic broad-based buds. Infection may remain confined to the lungs or disseminate hematogenously. Hematogenous dissemination can cause focal infection in numerous organs, including the skin, prostate, epididymides, testes, seminal vesicles, kidneys, vertebrae, ends of long bones, subcutaneous tissues, central nervous system, oral or nasal mucosa, thyroid, lymph nodes, and bone marrow.
(See also Overview of Fungal Infections.)
General reference
1. Smith DJ, Williams SL; Endemic Mycoses State Partners Group, Benedict KM, Jackson BR, Toda M. Surveillance for Coccidioidomycosis, Histoplasmosis, and Blastomycosis - United States, 2019. MMWR Surveill Summ. 2022;71(7):1-14. Published 2022 Aug 19. doi:10.15585/mmwr.ss7107a1
Symptoms and Signs of Blastomycosis
Pulmonary blastomycosis
Pulmonary blastomycosis may be asymptomatic or cause an acute, self-limited disease that often goes unrecognized. It can also begin insidiously and develop into a chronic, progressive infection. Pleural effusion occurs occasionally.
Symptoms include a productive or dry hacking cough, chest pain, dyspnea, fever, chills, and drenching sweats. Some patients have rapidly progressive infections, and acute respiratory distress syndrome may develop.
The nonspecific clinical presentation and radiologic findings of pulmonary blastomycosis can mimic bacterial pneumonia, causing diagnostic delays and the potential for inappropriate or delayed treatment.
Extrapulmonary disseminated blastomycosis
In extrapulmonary disseminated blastomycosis, symptoms depend on the organ involved.
Skin lesions are the most common site of dissemination; they may be single or multiple and may occur with or without clinically apparent pulmonary involvement. Papules or papulopustules usually appear on exposed surfaces and spread slowly. Painless, small abscesses develop on the advancing borders. Irregular, wartlike papillae may form on surfaces. Sometimes bullae develop. As lesions enlarge, the centers heal, forming atrophic scars. When fully developed, an individual lesion appears as an elevated verrucous patch, usually ≥ 2 cm wide with an abruptly sloping, purplish red, abscess-studded border. Ulceration may occur if bacterial superinfection is present.
Hematogenous dissemination can cause focal infection in numerous organs, including the skin, prostate, epididymides, testes, seminal vesicles, kidneys, vertebrae, ends of long bones, subcutaneous tissues, central nervous system, oral or nasal mucosa, thyroid, lymph nodes, and bone marrow.


This image shows a raised, crusted, irregularly bordered ulcerative skin lesion with small microabscesses at the periphery of the lesion.
This image shows a raised, crusted, irregularly bordered ulcerative skin lesion with small microabscesses at the periph
© Springer Science+Business Media


Extrapulmonary blastomycosis may affect the skin. Skin lesions manifest as papules, pustules, or bullae. This photo shows a bullous skin lesion.
Extrapulmonary blastomycosis may affect the skin. Skin lesions manifest as papules, pustules, or bullae. This photo sho
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


Extrapulmonary blastomycosis may affect the skin. Skin lesions may develop wartlike papillae or a verrucous appearance. This photo shows a verrucous skin lesion.
Extrapulmonary blastomycosis may affect the skin. Skin lesions may develop wartlike papillae or a verrucous appearance.
Image courtesy of www.doctorfungus.org © 2005.
This image shows a raised, crusted, irregularly bordered ulcerative skin lesion with small microabscesses at the periphery of the lesion.
This image shows a raised, crusted, irregularly bordered ulcerative skin lesion with small microabscesses at the periph
© Springer Science+Business Media
Extrapulmonary blastomycosis may affect the skin. Skin lesions manifest as papules, pustules, or bullae. This photo shows a bullous skin lesion.
Extrapulmonary blastomycosis may affect the skin. Skin lesions manifest as papules, pustules, or bullae. This photo sho
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Extrapulmonary blastomycosis may affect the skin. Skin lesions may develop wartlike papillae or a verrucous appearance. This photo shows a verrucous skin lesion.
Extrapulmonary blastomycosis may affect the skin. Skin lesions may develop wartlike papillae or a verrucous appearance.
Image courtesy of www.doctorfungus.org © 2005.
If bone lesions develop, overlying areas may sometimes show signs of inflammation such as swelling, warmth, and tenderness.
Genital lesions in men most commonly cause prostatitis and epididymitis associated with painful epididymal swelling, deep perineal discomfort, or prostatic tenderness detected during rectal examination. Genital lesions in women are less common and can cause tubo-ovarian abscess, endometritis, and salpingitis.
Central nervous system involvement can manifest as brain abscess, epidural abscess, or meningitis.
Diagnosis of Blastomycosis
Chest radiograph
Fungal cultures and smear
Blastomyces urine and serum antigen
Molecular diagnostics
If blastomycosis is suspected, a chest radiograph should be taken. Focal or diffuse infiltrates may be present, sometimes as patchy bronchopneumonia fanning out from the hilum. These findings must be distinguished from other causes of pneumonia (eg, bacteria, other mycoses, tuberculosis, tumors).
Skin lesions can be mistaken for sporotrichosis, tuberculosis, or basal cell carcinoma. Genital involvement may mimic tuberculosis.

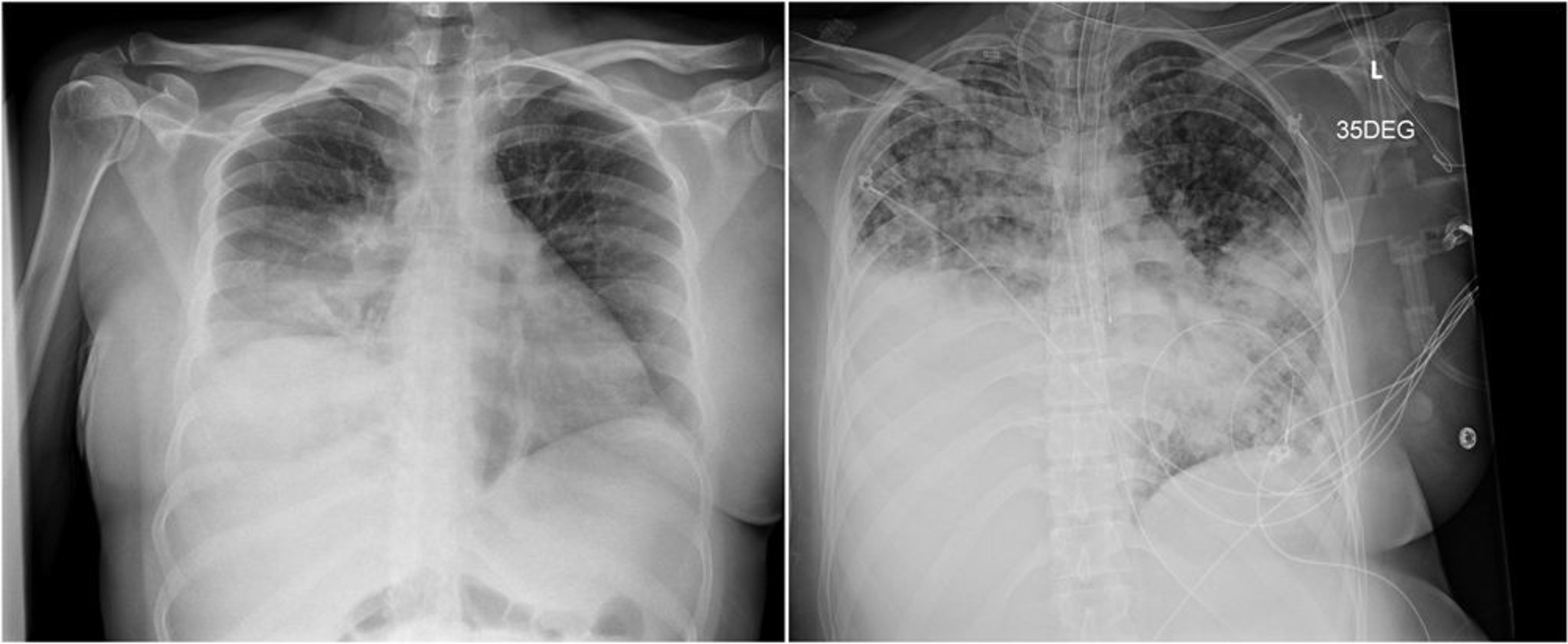
The radiograph on the left shows a right lower lobe consolidation that was mistaken for bacterial pneumonia.
The radiograph on the right, taken 3 weeks later, shows disease progression with patchy bilateral airspace opacities and dense consolidation in the right lower lung.
Images courtesy of Paschalis Vergidis, MD, MSc.
The diagnosis can be established by cultures of infected material or by direct microscopic visualization of the organism in cytologic or histopathologic specimens (1). Because culturing Blastomyces can pose a severe biohazard to laboratory personnel, the laboratory should be notified of the suspected diagnosis. The organism’s characteristic appearance, seen during microscopic examination of tissues or sputum, is also frequently diagnostic.
Serologic testing is not sensitive but is useful if positive (2).
A urine and serum antigen test is useful, but cross-reactivity with Histoplasma is high.
Molecular diagnostic tests (eg, polymerase chain reaction [PCR]) can aid the diagnosis.
Diagnosis references
1. Chapman SW, Dismukes WE, Proia LA, et al. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(12):1801-1812. doi:10.1086/588300
2. Martynowicz MA, Prakash UB. Pulmonary blastomycosis: an appraisal of diagnostic techniques. Chest. 2002;121(3):768-773. doi:10.1378/chest.121.3.768
Treatment of Blastomycosis
For mild to moderate disease (including cutaneous disease), itraconazole
For severe, life-threatening infection, liposomal amphotericin B
Treatment of blastomycosis depends on the severity of the infection.
For mild to moderate disease that does not involve the central nervous system and does not require hospitalization, oral itraconazole for 6 to 12 months is used (that does not involve the central nervous system and does not require hospitalization, oral itraconazole for 6 to 12 months is used (1). Although generally less effective, high-dose fluconazole may be tried in ). Although generally less effective, high-dose fluconazole may be tried initraconazole-intolerant patients with mild disease.
For mild to moderate cutaneous disease, itraconazole is recommended.
For severe, life-threatening infections, IV amphotericin B (liposomal) is usually effective (IV amphotericin B (liposomal) is usually effective (1). It is administered once a day for 1 to 2 weeks or until improvement is noted.
Therapy is changed to oral itraconazole once patients improve.Therapy is changed to oral itraconazole once patients improve.
Patients with central nervous system blastomycosis, pregnant patients, and immunocompromised patients should be treated with IV liposomal amphotericin B using the same dose schedule as for life-threatening infection.
Voriconazole, isavuconazonium, and posaconazole are active against Voriconazole, isavuconazonium, and posaconazole are active againstBlastomyces species, but clinical data are limited, and the role of these medications has not yet been defined.
The prognosis for cutaneous blastomycosis is generally favorable with appropriate antifungal therapy. Untreated blastomycosis is usually slowly progressive and in rare cases, can be ultimately fatal.
Treatment reference
1. Chapman SW, Dismukes WE, Proia LA, et al: Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis 46(12):1801-1812, 2008. doi: 10.1086/588300
Key Points
Inhaling spores of the dimorphic fungus Blastomyces can cause pulmonary disease and, less commonly, disseminated infection (particularly to the skin).
In North America, blastomycosis is endemic in the regions around the Great Lakes and the Ohio and Mississippi River Valleys (extending into the middle Atlantic and southeastern states).
The diagnosis is based on cultures of infected material; serologic testing is not very sensitive but helpful if positive.
For mild to moderate disease, use itraconazole.For mild to moderate disease, use itraconazole.
For severe disease, use liposomal amphotericin B.For severe disease, use liposomal amphotericin B.





