

Most pituitary tumors are adenomas. Symptoms include headache and endocrinopathies; endocrinopathies result when the tumor produces hormones or destroys hormone-producing tissue. Diagnosis is by MRI. Treatment includes correction of any endocrinopathy and surgery, radiation therapy, and dopaminergic agonists.
(See also Overview of Intracranial Tumors; Pituitary Lesions; and Prolactinoma.)
Most tumors of the pituitary and suprasellar region are pituitary adenomas. Rarely, pituitary tumors are carcinomas. Meningiomas, craniopharyngiomas, metastases, and dermoid cysts may also develop in the region of the sella turcica.
Adenomas may be secretory or nonsecretory. Secretory adenomas produce pituitary hormones; many secretory adenomas are < 10 mm in size (microadenomas). Secretory adenomas can be classified by histologic staining characteristics (eg, acidophilic, basophilic, chromophobe [nonstaining]). The hormone produced often correlates with these characteristics; eg, acidophilic adenomas overproduce growth hormone, and basophilic adenomas overproduce adrenocorticotropic hormone (ACTH). The hormone most commonly overproduced is prolactin.
Any tumor that grows out of the pituitary can compress optic nerve tracts, including the chiasm. Tumors may also compress or destroy pituitary or hypothalamic tissue, impairing hormone production or secretion.
Symptoms and Signs of Pituitary Tumors
Headache may result from an enlarging pituitary adenoma, even when intracranial pressure is not increased. Visual manifestations such as bitemporal hemianopia, unilateral optic atrophy, and contralateral hemianopia may develop if a tumor compresses optic nerve tracts (see figure ).
Many patients present with an endocrinopathy due to hormone deficiency or excess:
Diabetes insipidus if less vasopressin is released because the hypothalamus is compressedif less vasopressin is released because the hypothalamus is compressed
Amenorrhea and galactorrhea in women and, less commonly, erectile dysfunction and gynecomastia in men if prolactin is overproduced
Gigantism before puberty or acromegaly after puberty if growth hormone is overproduced
Cushing syndrome if ACTH is overproduced
Sometimes pituitary tumors that compress tissue throughout the anterior lobe of the pituitary reduce production of multiple pituitary hormones, causing generalized hypopituitarism.
Rarely, hemorrhage into a pituitary tumor causes pituitary apoplexy, with sudden headache, ophthalmoplegia, and visual loss.
Diagnosis of Pituitary Tumors
MRI with 1-mm slices

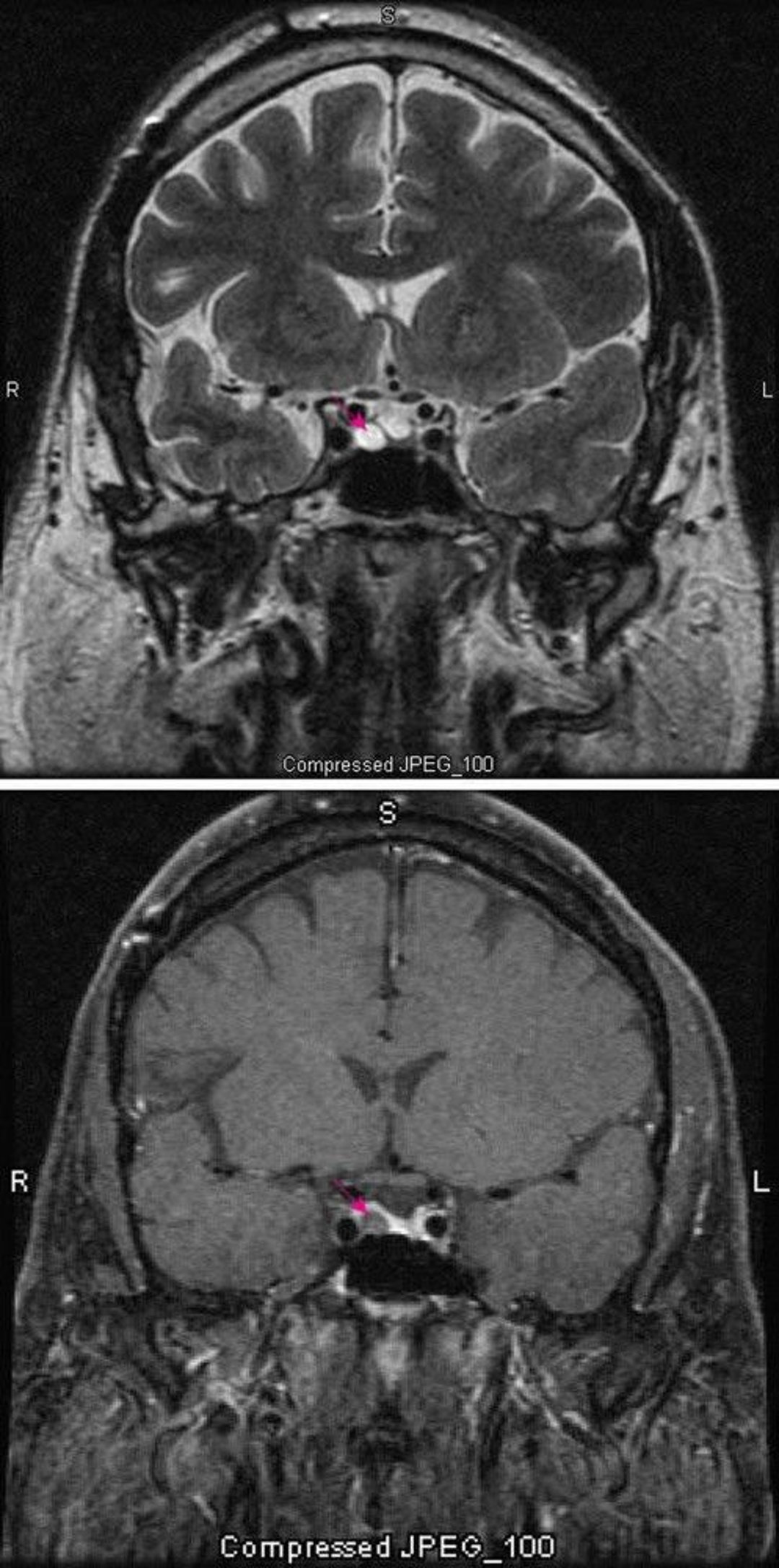
T2-weighted MRI scan (top) shows a pituitary microadenoma (red arrow). Contrast (bottom) normally enhances the pituitary (red arrow). The adenoma appears lighter.
Images courtesy of William R. Shapiro, MD.
Pituitary tumors are suspected in patients with unexplained headaches, characteristic visual abnormalities, or endocrinopathies. Neuroimaging with 1-mm thick slices is done. MRI is usually much more sensitive than CT, particularly for microadenomas.
Treatment of Pituitary Tumors
Surgical excision when needed and possible
For some endocrinopathies, medications
Endocrinopathies are treated.
Pituitary tumors that produce ACTH, growth hormone, or thyroid-stimulating hormone, and non-secretory adenomas are surgically excised, usually using a transsphenoidal approach. Sometimes, particularly for surgically inaccessible or multifocal tumors, radiation therapy is required.
Adenomas that produce prolactin are treated with dopaminergic agonists (eg, bromocriptine, pergolide, cabergoline), which lower blood levels and often shrink the tumor. Surgery and radiation therapy are usually unnecessary.Adenomas that produce prolactin are treated with dopaminergic agonists (eg, bromocriptine, pergolide, cabergoline), which lower blood levels and often shrink the tumor. Surgery and radiation therapy are usually unnecessary.
Key Points
Most pituitary tumors are adenomas, which may be secretory or nonsecretory.
Secretory adenomas may cause diabetes insipidus, galactorrhea, Cushing syndrome, or gigantism or acromegaly.
Any pituitary tumor may compress optic nerve tracts, causing bitemporal hemianopia, unilateral optic atrophy, or contralateral hemianopia, or it may compress pituitary tissue, causing a deficiency of pituitary hormones.
Excise tumors and treat endocrinopathies; adenomas that produce prolactin may require only treatment with dopaminergic agonists.





