

Herpes simplex keratitis is corneal infection with herpes simplex virus. It may involve the iris. Symptoms and signs include foreign body sensation, lacrimation, photophobia, and conjunctival hyperemia. Recurrences are common and may lead to corneal hypoesthesia, ulceration, permanent scarring, opacification, thinning of the corneal stroma, and decreased vision. Diagnosis is based on clinical suspicion, slit lamp exam findings, and sometimes viral culture. Treatment is with topical or systemic antiviral medications.
Herpes simplex keratitis usually affects the corneal surface but sometimes involves the corneal stroma (the deeper layers of the cornea) or the inner corneal surface (endothelium), anterior chamber, and iris. Stromal involvement is probably an immunologic response to the virus.
As with all herpes simplex virus infections, there is a primary infection, followed by a latent phase, in which the virus enters the nerve roots. Latent virus may reactivate, causing recurrent symptoms.
Herpes simplex keratitis is a major cause of blindness worldwide.
Symptoms and Signs of Herpes Simplex Keratitis
Primary infection
The initial (primary) infection is usually nonspecific self-limiting conjunctivitis, often in early childhood and usually without corneal involvement. If the cornea is involved, symptoms include foreign body sensation, lacrimation, photophobia, and conjunctival hyperemia. Sometimes vesicular blepharitis (blisters on the eyelid) follows, symptoms worsen, vision blurs, and blisters break down and ulcerate, then resolve without scarring in about a week.
Recurrent infection
Recurrent ocular herpes affects the cornea. Three main types of herpes simplex keratitis are
Epithelial keratitis (dendritic keratitis)
Disciform keratitis (localized endotheliitis)
Stromal keratitis

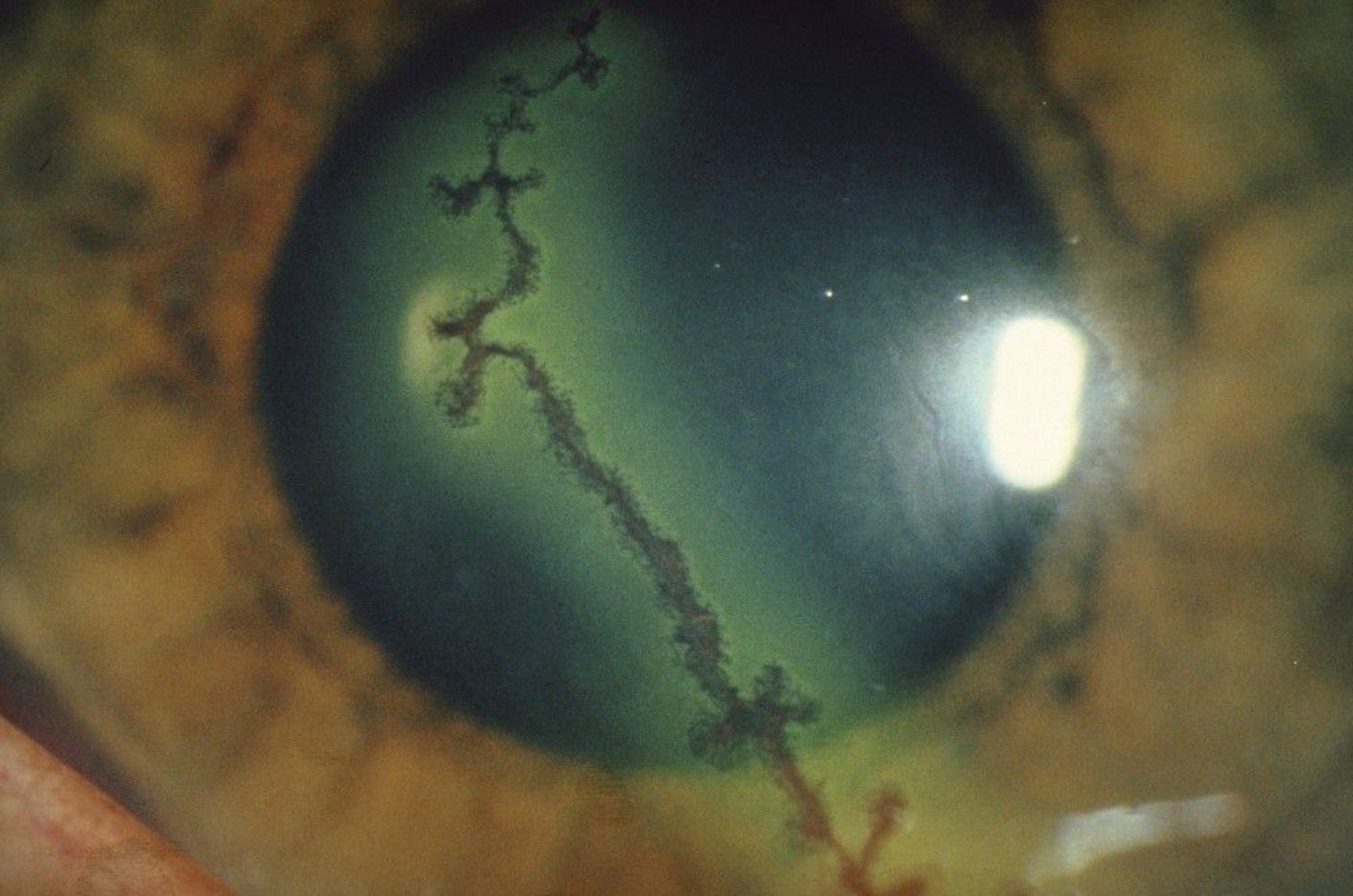
This photo shows dendritic (epithelial) keratitis, characterized by a branched corneal epithelial defect resembling a branching tree. Note the thinness of the dendrite and the enlarged bulbs at the ends of each branch. It is best seen with fluorescein staining (green color). In this photo, the dendrite was also stained with another dye (rose bengal), coloring it red.
ARGENTUM/SCIENCE PHOTO LIBRARY
Reactivation of latent herpes simplex can be triggered by UV light exposure (eg, intense sunlight, corneal cross-linking [an ultraviolet light treatment that stiffens the cornea], or laser refractive procedures), fever, menstruation, significant systemic physical stress (eg, burns or multiple fractures), immunosuppression, or use of glucocorticoids (topical ophthalmic, periocular injection, intraocular injection, or systemic). Recurrences usually take the form of epithelial keratitis (also called dendritic keratitis), with tearing, foreign body sensation, and a characteristic branching (dendritic or serpentine) lesion of the corneal epithelium with bulb-like terminals that stain with fluorescein. Multiple recurrences may result in corneal hypoesthesia or anesthesia, ulceration, permanent scarring, opacification, thinning of the corneal stroma, and decreased vision.Reactivation of latent herpes simplex can be triggered by UV light exposure (eg, intense sunlight, corneal cross-linking [an ultraviolet light treatment that stiffens the cornea], or laser refractive procedures), fever, menstruation, significant systemic physical stress (eg, burns or multiple fractures), immunosuppression, or use of glucocorticoids (topical ophthalmic, periocular injection, intraocular injection, or systemic). Recurrences usually take the form of epithelial keratitis (also called dendritic keratitis), with tearing, foreign body sensation, and a characteristic branching (dendritic or serpentine) lesion of the corneal epithelium with bulb-like terminals that stain with fluorescein. Multiple recurrences may result in corneal hypoesthesia or anesthesia, ulceration, permanent scarring, opacification, thinning of the corneal stroma, and decreased vision.
Most patients with disciform keratitis, which involves the corneal endothelium primarily, have a history of epithelial keratitis. Disciform keratitis is a deeper, disc-shaped, localized area of secondary corneal stromal edema and haze accompanied by anterior uveitis. This form may cause ache, photophobia, and reversible vision loss.
Stromal keratitis is likely to cause necrosis of the stroma and severe ache, photophobia, foreign body sensation, ulceration, permanent scarring, opacification, neovascularization, thinning of the corneal stroma, and irreversible decreased vision.
Diagnosis of Herpes Simplex Keratitis
Slit-lamp examination


This photo shows a dendritic (branching) ulcer (green) on a patient's cornea. The ulcer is green because it has been stained with fluorescein.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Slit-lamp examination is mandatory. Finding a dendrite is enough to confirm the diagnosis in most cases of HSV dendritic keratitis. The diagnosis of herpes disciform keratitis and herpes stromal keratitis is predominantly clinical, based on a history of herpetic ocular disease and slit lamp exam findings. Herpes stromal keratitis is characterized by a stromal opacity often accompanied by neovascularization and inflammation. Herpes disciform keratitis causes stromal edema due to corneal endothelial dysfunction.
When the appearance is not conclusive, viral culture or a nucleic acid amplification tests (NAAT) swab of the lesion can confirm the diagnosis.
Treatment of Herpes Simplex Keratitis
Topical ganciclovir or trifluridine Topical ganciclovir or trifluridine
Oral or IV acyclovir or valacyclovir Oral or IV acyclovir or valacyclovir
For stromal involvement or uveitis, topical corticosteroids in addition to antiviral medications
Most patients are managed by an ophthalmologist. If stromal or uveal involvement occurs, treatment is more involved and referral to an ophthalmologist is mandatory (1).
Dendritic (epithelial) keratitis can be treated with topical therapy (eg, ganciclovir or trifluridine). Topical therapy is usually effective and is tapered off over 2 to 3 weeks.Dendritic (epithelial) keratitis can be treated with topical therapy (eg, ganciclovir or trifluridine). Topical therapy is usually effective and is tapered off over 2 to 3 weeks.
Alternatively, oral therapy (eg, acyclovir or valacyclovir) is also effective. Acyclovir or valacyclovir may be prescribed as suppressive therapy to prevent frequent recurrences as well as to preserve eyesight in patients whose vision has been threatened. The dose of each medication should be adjusted in patients with renal dysfunction. Alternatively, oral therapy (eg, acyclovir or valacyclovir) is also effective. Acyclovir or valacyclovir may be prescribed as suppressive therapy to prevent frequent recurrences as well as to preserve eyesight in patients whose vision has been threatened. The dose of each medication should be adjusted in patients with renal dysfunction.
Immunocompromised patients may require IV antivirals (eg, acyclovir). Immunocompromised patients may require IV antivirals (eg, acyclovir).
Topical corticosteroids are contraindicated in epithelial keratitis, but they may be effective when used with an antiviral to manage later-stage stromal involvement (disciform or stromal keratitis) or uveitis. In such cases, patients may be given prednisolone acetate. . In such cases, patients may be given prednisolone acetate.
If the epithelium surrounding the dendrite is loose and edematous, debridement by gentle swabbing with a cotton-tipped applicator before beginning pharmacotherapy may speed healing. Topical medications to relieve photophobia include atropine 1% and scopolamine 0.25% 3 times a day.If the epithelium surrounding the dendrite is loose and edematous, debridement by gentle swabbing with a cotton-tipped applicator before beginning pharmacotherapy may speed healing. Topical medications to relieve photophobia include atropine 1% and scopolamine 0.25% 3 times a day.
Treatment reference
1. White ML, Chodosh J: Herpes simplex virus keratitis: A treatment guideline — 2014. American Academy of Ophthalmology. Accessed July 1, 2024.
Key Points
Herpes simplex keratitis typically is a recurrence of primary herpes simplex eye infection that was usually a nonspecific, self-limiting conjunctivitis.
Characteristic findings include a branching dendritic or serpentine corneal lesion (indicating dendritic keratitis), disc-shaped, localized corneal edema and haze plus anterior uveitis (indicating disciform keratitis), or stromal scarring (indicating stromal keratitis).
Diagnosis is confirmed by characteristic clinical findings, by viral culture, or by NAAT swab.
Treatment requires antivirals, usually topical ganciclovir or trifluridine or oral acyclovir or valacyclovir.Treatment requires antivirals, usually topical ganciclovir or trifluridine or oral acyclovir or valacyclovir.
Drug Information for the Topic





