



The liver produces approximately 500 to 600 mL of bile each day. Bile is isosmotic with plasma and consists primarily of water and electrolytes but also organic compounds: bilirubin, bile salts, phospholipids (mostly lecithin), cholesterol, and proteins that regulate gastrointestinal function and medications or their metabolites.
Bilirubin is a degradation product of heme compounds from senescent red blood cells (RBCs) and is the pigment that gives bile its yellow-green color.
Bile salts (bile acids) are the major organic component in bile. Hepatocytes use active transport to secrete bile salts into the canaliculi, the channels between adjacent cells. Canalicular transport is the rate-limiting step in bile formation. Once secreted, bile salts draw other bile components (particularly sodium and water) into the canaliculus by osmosis. Bile salts are also biologic detergents that enable the body to excrete cholesterol and potentially toxic compounds (eg, bilirubin, drug metabolites). The function of bile salts in the duodenum is to solubilize ingested fat and fat-soluble vitamins, facilitating their digestion and absorption. From the canaliculi, bile flows into the intrahepatic collecting system, then into the right or left hepatic duct, and finally into the common hepatic duct.
During fasting, approximately 75% of the bile secreted passes from the common hepatic duct into the gallbladder via the cystic duct. The rest flows directly into the common bile duct (formed by the junction of the common hepatic and cystic ducts) into the duodenum. Also during fasting, the gallbladder absorbs up to 90% of bile water, concentrating and storing bile.
View of the Liver and Gallbladder

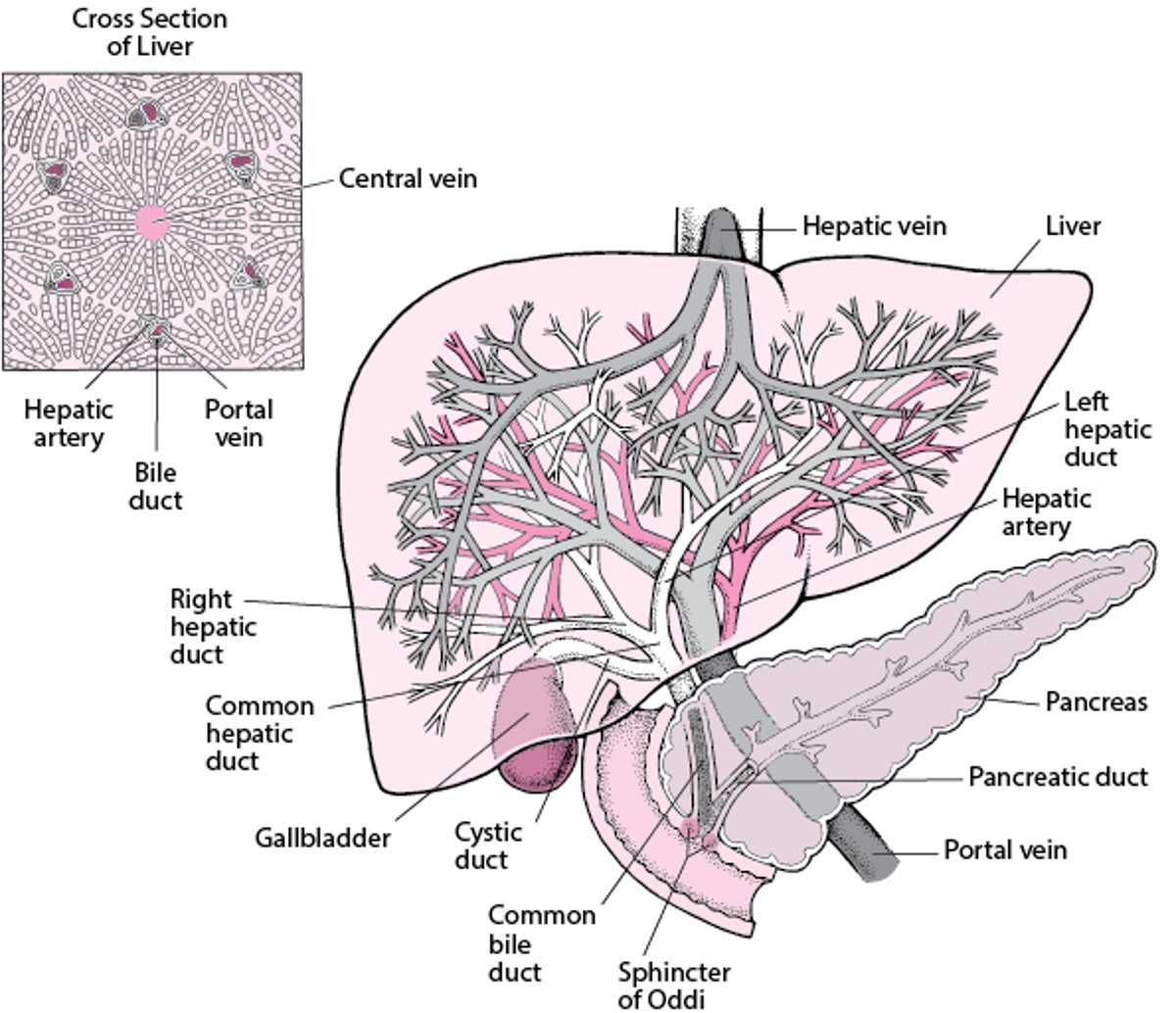
Bile empties from the gallbladder into the common bile duct via the cystic duct. The common bile duct joins with the pancreatic duct to form the ampulla of Vater, which empties into the duodenum. Before joining the pancreatic duct, the common bile duct tapers to a diameter of ≤ 0.6 cm.


1 = Bile duct branch; 2 = hepatic artery branch; 3 = portal vein branch; 4 = hepatocytes.
Image courtesy of Danielle Tholey, MD, and M. Isabel Fiel, MD, MS, FAASLD.
The sphincter of Oddi, which surrounds both the pancreatic duct and the common bile duct, includes a sphincter for each duct. Bile does not normally flow retrograde into the pancreatic duct. These sphincters are highly sensitive to cholecystokinin and other gut hormones (eg, gastrin-releasing peptide) and to alterations in cholinergic tone (eg, by anticholinergic medications).
Eating releases gut hormones and stimulates cholinergic nerves, causing the gallbladder to contract and the sphincter of Oddi to relax. As a result, the gallbladder empties 50 to 75% of its contents into the duodenum. Conversely, during fasting, an increase in sphincter tone leads to gallbladder filling.
In the proximal small bowel, bile salts undergo passive diffusion and are poorly absorbed; most intestinal bile salts reach the terminal ileum, which then actively absorbs 90% of bile salts into the portal venous circulation. Returned to the liver, bile salts are efficiently extracted, promptly modified (eg, conjugated if they arrive in the free form), and secreted back into bile. Bile salts circulate through this pathway from liver to gut to liver—the enterohepatic circulation—10 to 12 times per day.
Gallstones are hardened deposits of cholesterol, bile salts, or pigment that form in the gallbladder or biliary tract, primarily as a result of imbalances in the composition of bile. Most disorders of the biliary tract result from gallstones, although gallstones in the gallbladder (cholelithiasis) are usually asymptomatic. Bile flow may be blocked by gallstones in the bile ducts (choledocholithiasis), causing biliary colic and cholangitis (inflammation of the bile duct), most commonly due to infection in the setting of biliary obstruction. Alternatively, gallstones in the cystic duct can cause inflammation of the gallbladder (cholecystitis). Cholecystitis may be acute, developing over hours, or chronic, persisting for a long time.
Bile flow can also be slowed (called cholestasis) by liver disease such as cirrhosis or hepatitis, and slowed or blocked by tumors. In patients who have late-stage HIV, bile flow can be slowed or blocked by strictures caused by opportunistic infections (HIV-related cholangiopathy). Cholestasis resulting from bile duct strictures (called sclerosing cholangitis) can also lead to inflammation and liver fibrosis. Usually, the cause of sclerosing cholangitis is unknown (called primary sclerosing cholangitis). Parasite infestation can also block biliary flow.
Biliary disorders not specifically related to gallstones include postcholecystectomy syndrome, which occurs after the gallbladder has been removed, and acalculous biliary pain.





