



A person who has eye symptoms should be checked by a doctor. However, some eye disorders cause few or no symptoms in their early stages, so the eyes should be checked regularly (every 1 to 2 years or more frequently if there is an eye condition) by an ophthalmologist or an optometrist. An ophthalmologist is a medical doctor who specializes in the evaluation and treatment (surgical and nonsurgical) of eye disorders. An optometrist is a health care professional who specializes in the diagnosis and treatment of vision or refractive problems (refractive errors).
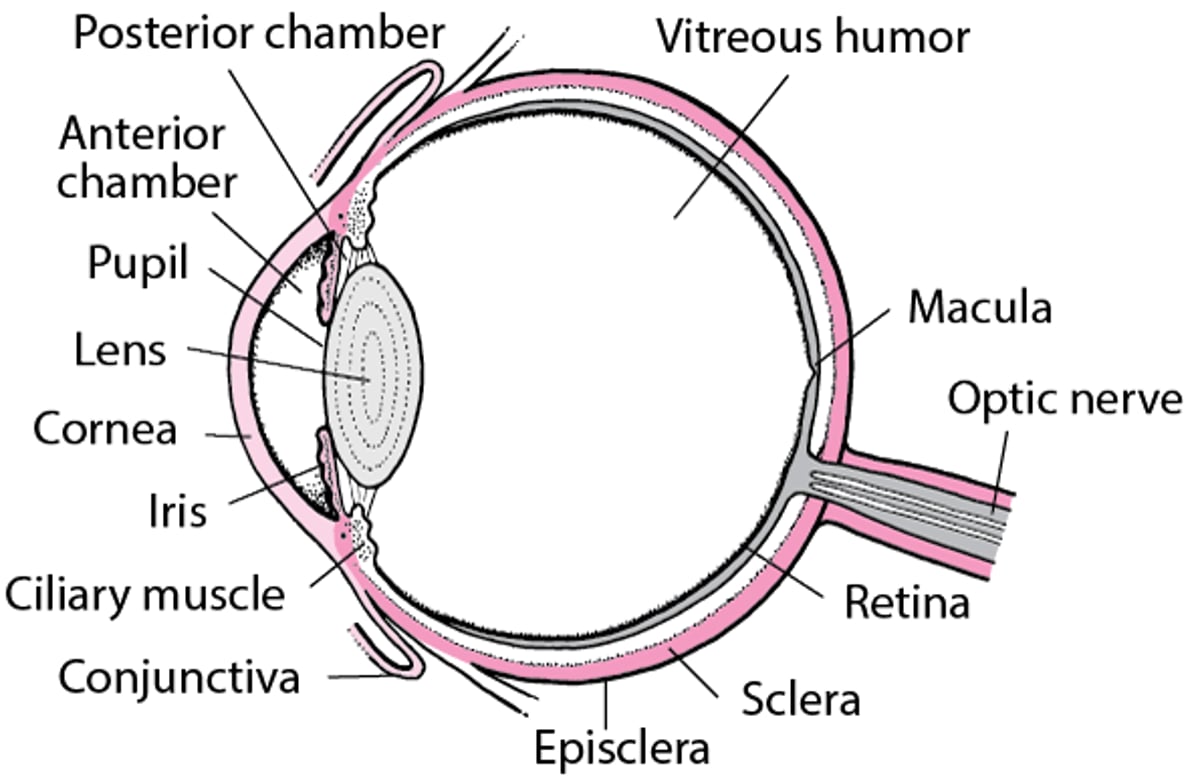
An Inside Look at the Eye

Diagnosis of eye disorders is initially based on the person's symptoms, the appearance of the eyes, and the results of an examination.
A person with eye or vision problems describes the location and duration of the symptoms, and then the ophthalmologist examines the eye, the area around it, and possibly other parts of the body, depending on the suspected cause. An eye examination usually includes refraction, visual field testing, ophthalmoscopy (also called funduscopy), a slit-lamp examination, and tonometry. By having the person look in all directions, the examiner can determine how the cranial nerves supplying the muscles that move the eyes (called extraocular muscles) are functioning.
Refraction
Refraction is the procedure examiners use to assess focusing problems. Problems with visual acuity (sharpness of vision) that result from refractive errors, such as nearsightedness, farsightedness, astigmatism, and presbyopia, are diagnosed by refraction. Acuity is usually measured on a scale that compares a person's vision at 20 feet (about 6 meters) with that of someone who has perfect vision. Thus, a person who has 20/20 vision sees objects that are 20 feet away with the same clarity as a person with perfect vision, but a person who has 20/200 vision sees at 20 feet only as clearly as a person with perfect vision sees at 200 feet (about 61 meters).
One important visual acuity test uses the Snellen chart (eye chart), which is a large card or lighted box that displays rows of letters in smaller and smaller sizes. The chart is read from a standard distance. The degree of visual acuity is determined by the size of the row of letters that the person can read. For people who are unable to read, a modified chart can be used in which the letters are represented by an upper case "E," which is rotated randomly. People are asked to describe which way the "E" is facing. If a person cannot read anything from a chart, the examiner may see whether the person can count the examiner's fingers or see whether the examiner's hand moves. Examiners also test near vision by asking the person to read a standard near card or newsprint at a distance of about 14 inches (35 centimeters).
Automated refraction is done with a device that determines the refractive error of the eye by measuring how light is changed when it enters the eye. The person sits in front of the autorefractor, a beam of light is emitted from the device, and the eye's response is measured. The machine uses this information to calculate the lens prescription needed to correct the person's refractive error. This measurement takes only a few seconds.
A phoropter is the device commonly used, in conjunction with a Snellen chart, to determine the best corrective lenses for a person being assessed for eyeglasses or contact lenses. The phoropter contains a complete range of corrective lenses, allowing the person to compare different levels of correction while viewing the chart. Typically, the eye doctor uses the phoropter to refine the information obtained from the autorefractor before prescribing lenses.
Visual Field Testing
The visual field is the entire area of vision that is seen out of each eye, including the corners (peripheral vision). The visual field may be tested as a routine part of an eye examination. It may also be tested in detail if people notice specific changes in vision, for example, if they keep bumping into objects on one side.
The simplest way to test peripheral vision is for a doctor to face the person and gradually move a finger or another small target (such as a match) toward the person's center of vision from above, below, left, and right. The person tells the doctor when the moving finger or target is first detected. For the result of the test to be valid, the person's vision must be fixed on the doctor's face (and not looking for the finger or target). The eye not being tested is closed.
The visual field may be measured in greater detail with a tangent screen or a Goldmann perimeter. With these tests, the person stares at the center of a black screen or a hollow, white, spherical device (which resembles a small satellite dish). An object or a light is moved slowly from the periphery toward the center of vision from many different directions. The person indicates when light is first seen out of the corner of the eye. A mark is made on the screen or perimeter indicating where the person can see, thus allowing recognition of blind spots. Visual fields can also be measured using computerized automated perimetry. In this test, the person stares at the center of a large shallow bowl and presses a button whenever a flash of light is seen.
The Amsler grid is used to test the central area of vision. The grid consists of a black card covered with a white grid and with a white dot in its center. The person notes any distortion in the lines of the grid while staring at the white dot. Each eye is tested at a normal reading distance and while wearing reading glasses, if the person normally uses them. If an area of the grid cannot be seen, an abnormal blind spot may exist. Beyond the area tested by the Amsler grid, there is a normal, small blind spot where the optic nerve leaves the eye. However, people are not aware of this normal blind spot. Wavy lines or a missing area (other than the normal blind spot) suggests a possible problem with the macula (the area of the retina responsible for central vision). The test is simple enough to be used at home and is useful for monitoring macular degeneration.
Color Vision Testing
A variety of tests can be used to detect a reduced ability to perceive certain colors (color blindness). Ishihara color plates, which are most commonly used, are made of fields of small colored dots crowded together on a white background to form a large circle. Colored numbers or symbols are hidden in the fields of colored dots. The dots are usually arranged so that people with normal color vision see a particular number. People who have color blindness see another number or no number, depending on the type of color blindness.
Ophthalmoscopy
A direct ophthalmoscope is a handheld device that looks like a small flashlight with magnifying lenses. With an ophthalmoscope, doctors shine light into the eye to examine the cornea, lens, vitreous humor (the jellylike substance that fills the back of the eye), retina, optic nerve, and the retinal veins and arteries (see Structure and Function of the Eyes). The person looks straight ahead as the beam of light is shined into the eye. Often, eye drops are given to dilate (enlarge) the pupil, which allows the doctor to have a better view.
Ophthalmoscopy is painless, but if eye drops are used to dilate the pupils, vision may be temporarily blurred, and the person will be more sensitive to light for a few hours afterward.
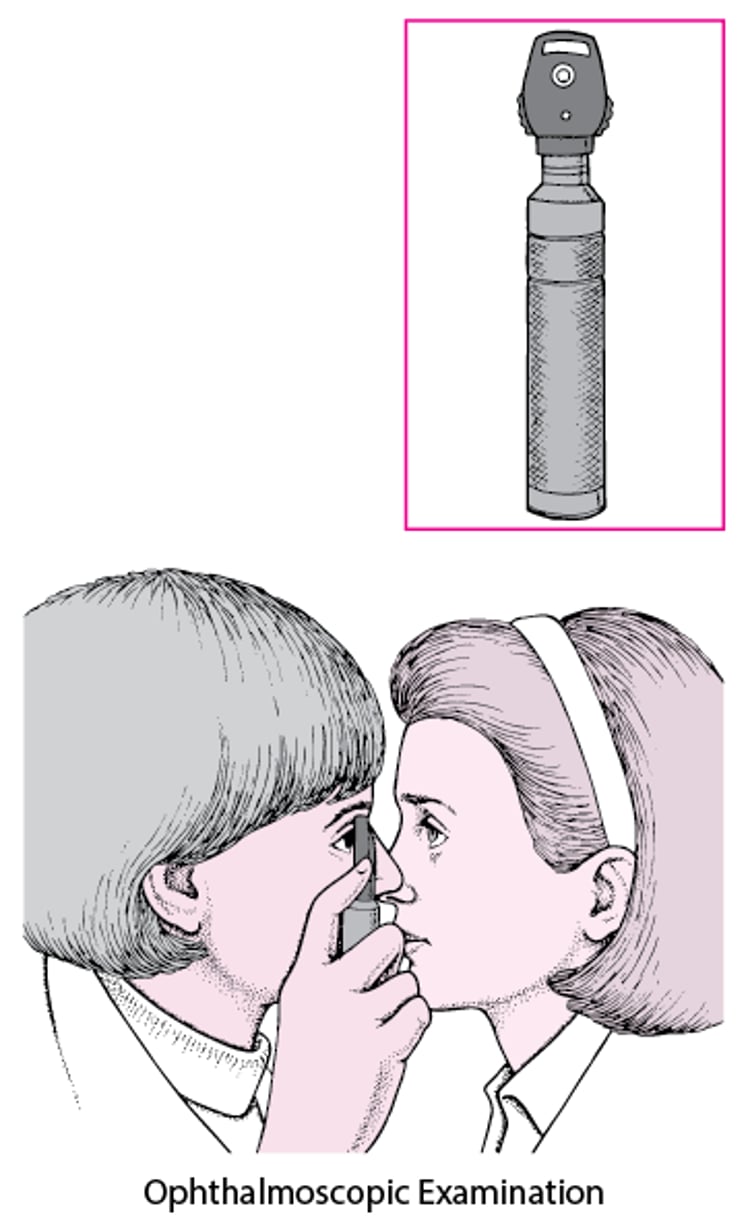
What Is an Ophthalmoscope?
An ophthalmoscope is an instrument that enables a doctor to examine the inside of a person's eye. The instrument has an angled mirror, various lenses, and a light source. With it, a doctor can see the retina, the optic nerve, the retinal veins and arteries, and certain problems that can affect the vitreous humor (the jellylike substance in the eye). |

Ophthalmoscopy is a standard part of every regular eye examination. Ophthalmoscopy is used to detect not only changes in the retina due to eye disease but also changes in the eyes due to certain diseases affecting other parts of the body. For instance, it is used to
Detect the changes that occur in the retinal blood vessels in people who have high blood pressure, arteriosclerosis, and diabetes mellitus
Provide a clue to elevated pressure within the brain, which results in a swelling (pushing-out) of the normally cupped optic disk (papilledema)
Tumors on the retina can be seen with ophthalmoscopy. Macular degeneration can be diagnosed with ophthalmoscopy as well.
Ophthalmologists and optometrists also use an instrument called an indirect ophthalmoscope. During indirect ophthalmoscopy, a binocular device is placed on the doctor's head and a handheld lens is used in front of the person's eye to focus the image inside the eye. This method gives a three-dimensional view, allowing a better view of objects that have depth, including a detached retina. It also allows a brighter light source to be used, which is important if the interior of the eye is cloudy, for instance, because of a cataract. The indirect ophthalmoscope also allows a much wider field of view than a direct ophthalmoscope, so that the doctor can examine more of the retina.
Slit-Lamp Examination
What Is a Slit Lamp?
A slit lamp is an instrument that enables a doctor to examine the entire eye under high magnification and that allows measurement of depth. The slit lamp focuses a bright light into the eye. |

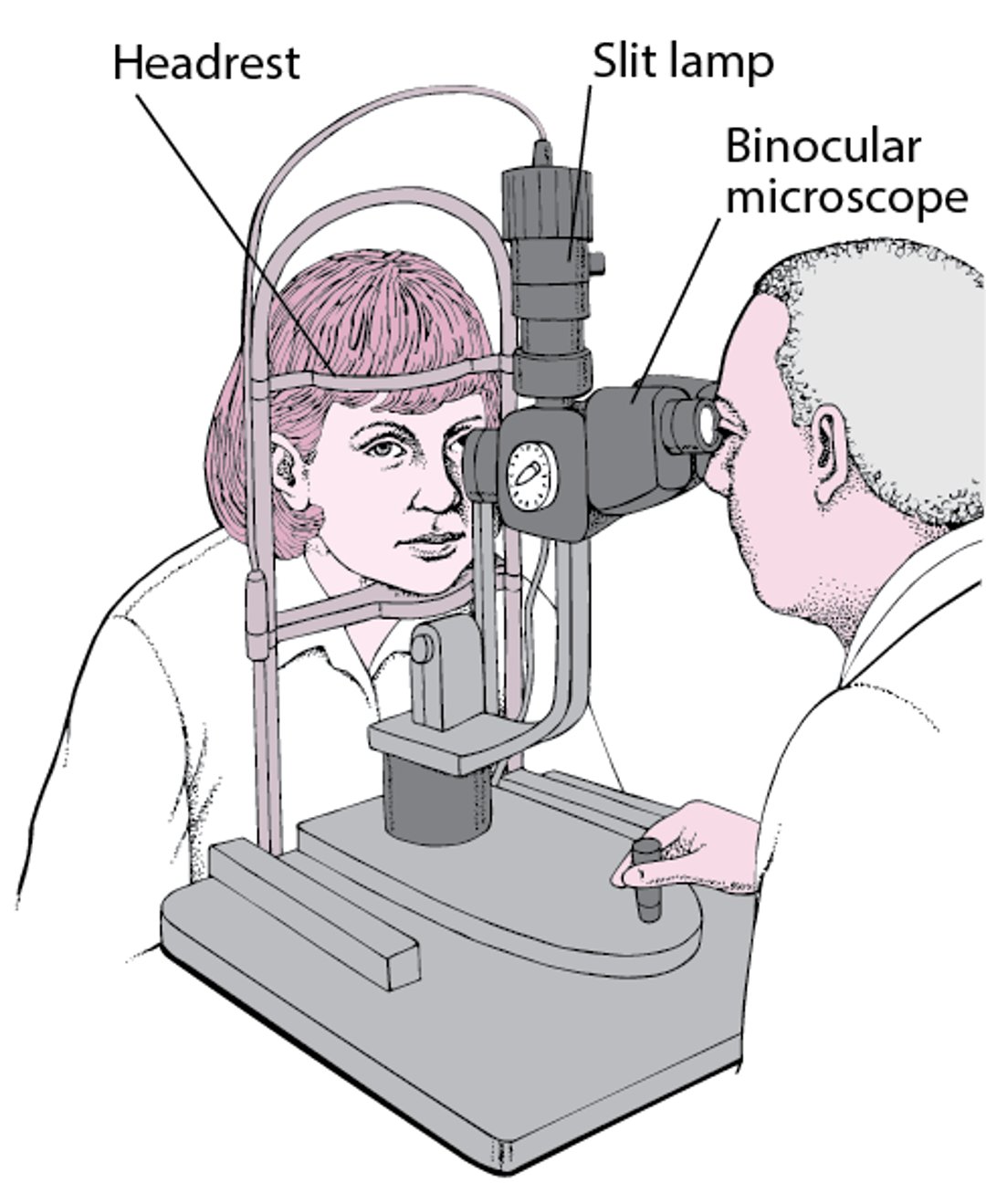
The slit lamp is a table-mounted binocular microscope that shines a light into the eye to allow the doctor to examine the entire eye under high magnification. The slit lamp has better optics than the direct ophthalmoscope, providing magnification and a three-dimensional view, which allows measurement of depth. A slit lamp is the best instrument for examining the following structures:
Eyelids
Tissues and skin around the eyes
Iris
Surface of the eye (including the cornea and conjunctivae)
Aqueous humor (the fluid in the front part of the eye between the cornea and the iris)
Often, eye drops are used to dilate the pupils so that the doctor can view even more of the eye, including the lens, vitreous humor, retina, and optic nerve. Sometimes, in people who have or might have glaucoma, an additional lens is placed on or held in front of the eye to allow examination of the angle between the iris and the front part of the eye (inside surface of the cornea). This examination is called gonioscopy.
Tonometry
With tonometry, the pressure within the eye can be measured. Normal pressure within the eye is 8 to 21 millimeters of mercury (mm Hg). Pressure in the eye is measured to detect certain types of glaucoma and monitor their treatment.
The noncontact air-puff tonometer can be used to screen for elevated pressure in the eye. This device is not highly accurate, but it is useful in identifying people who may need further testing. A small puff of air is blown against the cornea, which causes the person to blink but is not uncomfortable. The puff of air flattens the cornea, and the device measures the time (in thousandths of a second) it takes to do so. It takes less time for the puff of air to flatten the cornea in an eye with normal pressure than it does an eye in which pressure is elevated.
Applanation tonometry is a more accurate method. The applanation tonometer is usually attached to a slit lamp. After numbing the eye with drops, the doctor observes the eye through a slit lamp while the applanation tonometer is gently moved until it rests on the cornea. The amount of pressure it takes to flatten the cornea is related to the pressure within the eye.
Portable, handheld applanation instruments are also used for tonometry. Eye drops that numb the eye are given, then the instrument is gently placed on the cornea and a pressure reading is obtained. Portable applanation tonometers can be used in the emergency department or a doctor's office to quickly detect increased pressure in the eye. A handheld rebound tonometer can be used to measure the pressure within the eye without the use of eyedrops to numb the eye. It is useful in children and is widely used in emergency departments by nonophthalmologists.





